 Introduction with a case
Introduction with a case

I was once called to admit a patient with idiopathic pulmonary fibrosis to the ICU because of severe hypoxemia. On exam, I was surprised to find a patient who was quite comfortable, saturating 100% on BiPAP with an FiO2 of 100%.
It turned out that the patient had previously had an oxygen saturation of 90% on four liters nasal cannula (her home oxygen prescription). An ABG had been performed, revealing a PaO2 of 54 mm. The medicine team was alarmed by this low PaO2, so they titrated up her oxygen while monitoring serial ABGs. They were unable to increase her PaO2 very much using a nasal cannula, so eventually she was placed on BiPAP.
My recommendation was to stop obtaining ABGs and to titrate the oxygen based on pulse oximetry. She was weaned back to four liters and didn’t require ICU transfer.
This case may seem silly, but it highlights some common issues. In a patient with an adequate pulse oximetry waveform, what is the best way to monitor oxygenation? What if the ABG and pulse oximetry seem to disagree?
Ten reasons why pulse oximetry is generally the best way to monitor oxygenation.
For a patient with a good pulse oximetry waveform, pulse oximetry has numerous advantages compared to ABG monitoring:
#1. Pulse oximetry is a better measurement of oxygen delivery to the tissues.
PaO2, the oxygen tension in arterial blood, is the best way to determine how well the lungs are working. However, oxygen saturation is a better measurement of the systemic oxygen delivery to the tissues (DO2)(7):
DO2 = 13.4(cardiac output)(hemoglobin)(oxygen saturation)
#2. ABG is an invasive, painful, and expensive procedure.

An ABG is painful for the wrist and the wallet. The total cost of drawing and analyzing an ABG is nearly $200 (1). In contrast, pulse oximetry is noninvasive, painless, and free (2).
#3. One ABG begets another ABG…
 If you’re using the ABG as a therapeutic monitoring tool, then one ABG is rarely enough. The first ABG will often reveal some abnormality, leading to a minor change in the ventilator and repeat ABG. But the second ABG isn’t quite right, so you tweak the ventilator some more and get another ABG. Before you know it, you’ve ordered a cascade of ABGs and minor ventilator adjustments (with no real benefit to the patient).
If you’re using the ABG as a therapeutic monitoring tool, then one ABG is rarely enough. The first ABG will often reveal some abnormality, leading to a minor change in the ventilator and repeat ABG. But the second ABG isn’t quite right, so you tweak the ventilator some more and get another ABG. Before you know it, you’ve ordered a cascade of ABGs and minor ventilator adjustments (with no real benefit to the patient).
Occasionally, an arterial catheter might even be placed for the purpose of measuring frequent ABGs. This is generally a terrible idea. The availability of an easy source of arterial blood encourages frequent ABGs and other labs as well. For example, one study found that the presence of an arterial catheter correlated with a four-fold greater volume of phlebotomy (Tarpey 1990).
 #4. ABGs occasionally reflect venous samples
#4. ABGs occasionally reflect venous samples

Infrequently, ABGs will actually represent a venous or mixed sample. The oxygen extraction of the hand isn’t very high, so the level of oxygen in these venous samples may be only slightly lower than arterial blood. Thus, it may not be obvious that the sample was venous.
#5. Point-of-care ABG analyzers don’t actually measure oxygen saturation
 Many hospitals utilize point-of-care ABG analyzers. These devices typically measure PaO2 and subsequently use this to calculate the oxygen saturation (assuming a normal PaO2 vs. oxygen saturation curve). For patients with abnormal hemoglobin dissociation curves, this calculated saturation will be wrong.
Many hospitals utilize point-of-care ABG analyzers. These devices typically measure PaO2 and subsequently use this to calculate the oxygen saturation (assuming a normal PaO2 vs. oxygen saturation curve). For patients with abnormal hemoglobin dissociation curves, this calculated saturation will be wrong.
#6. ABG measurement may delay critical decisions.
 Measuring an ABG may delay interventions, such as ICU transfer or intubation. Sometimes it seems like physicians check an ABG when they don’t know what to do, in order to buy some time to think. At other times, it may seem like the ICU team requests an ABG to delay accepting a patient. Occasionally, physicians may feel obligated to check an ABG before calling for help, to exercise due diligence. Regardless, the practice of delaying treatment to obtain an ABG is usually unnecessary, particularly when oxygenation is concerned (3).
Measuring an ABG may delay interventions, such as ICU transfer or intubation. Sometimes it seems like physicians check an ABG when they don’t know what to do, in order to buy some time to think. At other times, it may seem like the ICU team requests an ABG to delay accepting a patient. Occasionally, physicians may feel obligated to check an ABG before calling for help, to exercise due diligence. Regardless, the practice of delaying treatment to obtain an ABG is usually unnecessary, particularly when oxygenation is concerned (3).
#7. PaO2 values are frequently misinterpreted.
We are constantly exposed to oxygen saturation values, leading to the development of a good sense about what they mean. Meanwhile, we are exposed to PaO2 values far less often, so we may struggle to interpret them.
The most common error is panicking about a low PaO2 value. PaO2 values are always much lower than oxygen saturation values. This is simply a reflection of the oxygen saturation curve (figure above). For example, a saturation of 88% correlates to a PaO2 of ~55mm. We’re generally comfortable with a saturation of 88%, but a PaO2 of 55mm may cause concern. The lower number is scarier.
This cognitive bias is often seen when ABGs are obtained in patients on mechanical ventilation. For a patient with mild hypoxemia, the PaO2 value will often be surprisingly low. This may lead to unnecessary increases in FiO2 and PEEP, delaying extubation.
#8. Checking the A-a gradient is over-utilized and potentially misleading.
The A-a gradient is the difference in oxygen tension between arterial blood and alveolar gas. Medical school courses love this. However, trying to use the ABG to diagnose the etiology of respiratory failure works poorly in real life:
- A normal A-a gradient doesn’t exclude pulmonary embolism (Stein 1995).
- ABG analysis usually fails to distinguish between different causes of respiratory failure (H&P, ultrasonography, and radiology are more accurate).
I sometimes see practitioners measure the A-a gradient of a critically ill patient who is requiring moderate to high levels of supplemental oxygen (e.g. >3 liters/min). Measuring this is pointless, because such patients will invariably have an elevated A-a gradient (if the patient had a normal A-a gradient, then they would require at most a low amount of supplemental oxygen)(4).
#9. A single ABG only measures a snapshot in time.
We’ve all been called to evaluate a patient for low oxygen saturation. Often, the saturation will bounce back rapidly on its own. Thus, we are constantly paying attention to oxygenation trends and averaging the oxygen saturation over time. Nurses are often keenly aware of this (“yeah, he desats whenever he starts coughing, don’t worry he’ll be fine in a minute”).
If we obtain an ABG, this sort of trending and averaging is impossible. We have access to only one point in time. It is impossible to know whether the oxygen saturation was transiently low, or if it was continuously low. The usual assumption is that the ABG reflects the patient’s ongoing condition (for example, if the patient was hypoxemic 15 minutes ago, then they must still be hypoxemic now). This assumption is frequently wrong.
#10. Changes in PaO2 are widely misinterpreted.
Let’s imagine that we obtain two ABGs to determine if there has been any change in oxygenation after initiating BiPAP. After starting BiPAP, the PaO2 decreases from 56 mm down to 49 mm. The oxygenation is worsening, so this indicates that we must intubate the patient.
No, it doesn’t. Please step away from the laryngoscope. Mallat 2015 compared back-to-back ABGs drawn via arterial catheters in 129 ICU patients to determine the repeatability of this test. There are large differences between these nearly simultaneous PaO2 values. The 95% confidence interval in comparing two PaO2 values was +/- 9mm:
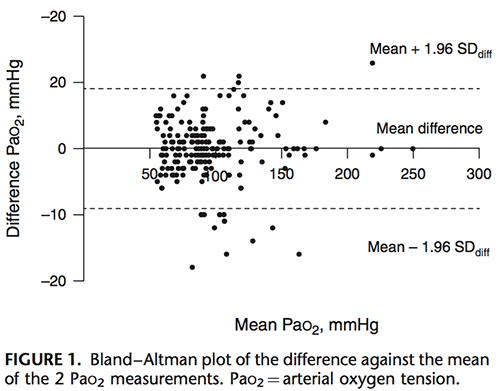 This is consistent with previous studies (5). Therefore, PaO2 differences in sequential ABGs will often reflect merely random variation. To be >95% confident that a difference doesn’t represent random noise, it should be >9mm. However, to be >95% confident that the a clinically significant change occurred (let’s say, >10mm change), the measured difference must be even higher, perhaps >19mm.
This is consistent with previous studies (5). Therefore, PaO2 differences in sequential ABGs will often reflect merely random variation. To be >95% confident that a difference doesn’t represent random noise, it should be >9mm. However, to be >95% confident that the a clinically significant change occurred (let’s say, >10mm change), the measured difference must be even higher, perhaps >19mm.
Changes in pulse oximetry are more likely to be meaningful, because the provider will typically look at numerous values over time. For example, if a patient had been consistently saturating in the high 90’s and is now consistently saturating in the 80s, we can be fairly confident that there has been a change (rather than representing two data points, this represents dozens of data points).
When is ABG useful to investigate oxygenation?
There are some situations when it may be helpful to use an ABG to investigate oxygenation.
#1. Pulse oximetry waveform is unreliable.
The most common situation where ABG is needed to test oxygenation is when pulse oximetry cannot provide a reliable waveform. For example, some patients have non-pulsatile blood flow from a ventricular assist device (VAD) or ECMO. Poor perfusion may lead to an erratic waveform.
#2. Diagnosis of methemoglobinemia.
Methemoglobinemia will artificially lower the patient’s measured oxygen saturation, usually producing saturations between 85-90%. This will typically cause providers to give more oxygen, which doesn’t improve the measured oxygen saturation. In this context, mismatch between the low saturation versus the PaO2 (which will often be elevated) suggests a diagnosis of methemoglobinemia (6).
#3. Calculation of the PaO2/FiO2 ratio to guide a specific therapeutic decision.
The PaO2/FiO2 ratio is often used as an index of severity of hypoxemia among patients who are intubated. Most evidence on proning in ARDS was performed using the PaO2/FiO2 ratio, including cutoffs determining which patients benefit. Thus, knowing the PaO2/FiO2 ratio may be helpful if you are contemplating whether to prone a patient.
🛑 ADDENDUM 12/21/20: New research shows that pulse oximetry may have a bias of +2% in patients with darkly pigmented skin. This could cause clinical errors in patients with borderline oxygen saturation (e.g. ~90%). For further discussion of this problem please see a blog here.
Why measuring PaO2 is generally unhelpful.
More information isn’t always better. One example of this can be borrowed from a post by Rory Speigel about the use of brain natriuretic peptide (BNP) for diagnosing heart failure. BNP has very good test characteristics for diagnosing heart failure. However, in clinical practice it doesn’t seem to help much. Why not?
The answer is that clinicians are very good at diagnosing heart failure without BNP (8). Thus, it’s unlikely that the BNP will improve our performance much. BNP could also point us in the wrong direction. It adds more information, but not necessarily superior information to what we already have.
Adding a PaO2 to an oxygen saturation is similar. Oxygen saturation alone is an excellent measurement of the patient’s oxygenation. For most patients, it is unclear what PaO2 adds above and beyond the oxygen saturation. The added information may be more likely to mislead than to inform.

For patients with an adequate oximetry waveform, pulse oximetry is usually superior to ABG for measuring oxygenation. The top ten reasons for this are:
- Saturation is a more direct measurement of tissue oxygen delivery than PaO2.
- ABG is a painful and expensive test.
- One ABG typically leads to a cascade of ABGs, multiplying costs and blood loss.
- ABGs may be contaminated with venous blood.
- Point-of-care ABG monitors calculate oxygen saturation, rather than measuring it directly.
- Obtaining an ABG may delay management.
- PaO2 values are easily misunderstood.
- Measuring the A-a gradient is over-utilized and potentially misleading.
- ABG only measures oxygenation at a single time point.
- Changes in PaO2 are widely misinterpreted.
Related: developing a sensible approach to gas exchange physiology
- ABG unhelpful in diagnosis of cardiopulmonary failure
- ABG/VBG not helpful in DKA
- Understanding oxygen delivery in ARDS
- Oxygen-ICU trial: 100% isn't an A+
- The Case of the Dubious Squire (Rory Spiegel discusses BNP in heart failure)
Notes
- Costs obviously vary based on location, perhaps within a range of roughly $100-$200. Costs include materials themselves, procedure costs, and analytic costs.
- All critically ill patients are monitored with pulse oximetry, so there is no added cost required to obtain this.
- I used to think that getting an ABG before starting BiPAP or intubation would be essential, to know what the patient’s “baseline” was. However, the patient is in a state of flux when acutely ill, so there is no real “baseline” during this period.
- The only scenario in which calculating the A-a gradient could be useful is in a patient with mild occult hypoventilation and normal lungs. In this case, the ABG will reveal a normal A-a gradient with elevated PaCO2, proving that hypoventilation is the cause of hypoxemia. If the hypoxemia is purely due to hypoventilation, then it should be easily overcome by increasing the FiO2 slightly (e.g. using 1-2 liters of oxygen). Thus, the use of ABG to determine A-a gradient may occasionally be helpful, but only in selected cases of very mild
- Thorson 1983 and Sasse 1994.
- Of course, most patients with saturation in the 80s don’t require an ABG to exclude methemoglobinemia. Investigation for methemoglobinemia may be justified when the patient has been exposed to drugs which may cause methemoglobinemia, and when there are other signs of methemoglobinemia (e.g. disproportional cyanosis).
- Of course, oxygen saturation is only part of DO2. It's possible to have a dangerously low DO2 despite having 100% oxygen saturation (e.g. if cardiac output and/or hemoglobin are low). Nonetheless, oxygen saturation is more closely related to DO2 than PaO2 is.
- Particularly with the use of lung ultrasonography. Prior to the availability of bedside cardiac and lung ultrasonography, I think BNP might have had more of a role.
Image credits: Leeches, Doctor wearing mask, oxygen dissociation curve.
{kind=link}

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Definitely agree with lots of this. “Blood gases” are most useful for understanding acid base disturbances, and I think have pretty limited utility for understanding how well someone is breathing, or how well their lungs are working….I trust my mark one eyeball and measurements of breathing, over a blood test that was relevant (maybe) 10 minutes ago when it was taken….. I really liked the points above about balancing blood gas results with clinical information when deciding about respiratory support……. My indications for BiPap are pretty simple and not really based on PaO2 or PaCO2. If you have respiratory distress… Read more »
Thanks. Agree 100% that your clinical judgment is better than an ABG (assuming a reasonable amount of training/experience). Agree also that indications for BiPAP are clinical and should not require ABG.
I’m working on a pair of posts about my approach to noninvasive respiratory support (BiPAP, HFNC, etc.), hopefully they’ll be out in a few weeks. (Spoiler alert: treat the patient, not the ABG… or better yet, treat the patient and don’t check an ABG.)
The only reasonable argument I’ve heard for demanding ABGs to monitor oxygenation is the “shoulder” argument: it may help you appreciate to a finer degree when a patient whose sat is adequate (low 90s, say) has a PaO2 (say barely over 50) that suggests they’re perched on the brink of their oxyhemoglobin dissociation curve and may decompensate with only a small loss of arterial oxygenation.
To what extent you could guess this from the sat alone is unclear. Presumably due to differences in affinity, sometimes the correlation does seem poor.
In theory that makes sense, but I’m not sure that an ABG would give you more insight into this than oxygen saturation. For example, when the patient’s saturation is 85-88% you could probably infer that they’re on the shoulder of the saturation curve. In practice, factors such as clinical appearance, work of breathing, and respiratory rate are probably better predictors of future deterioration (supported by stronger evidence, particularly respiratory rate).
Yes, but that relationship of Pa02 to Sa02 from the memorized hg dissociation curve is based on a normal pH, temperature, and ideal patient (no sickle cell, poisoning, etc), You’re not going to be able to infer that if the patient is a acidotic or alkylotic because the curve shifts. Hence 90% RA in a patient with a lower pH represents less of a concern than someone with a normal pH. You need an BG to evaluate pH. Am I seeing this incorrectly?
As a respiratory therapist, I don’t know how many times I’ve had this discussion with physicians and nurses in particular.
I feel like this article needs to be a poster to hang in our ICUs.
Thanks. Leave some room on the poster though, I’m planning some future posts on additional situations/reasons when ABG isn’t necessary. My overall feeling is that given the combination of pulse oximetry, end tidal CO2, and venous blood gas analysis it should be possible to nearly eliminate ABGs.
Great article Dr. Farkas. I’ve been working as a respiratory therapist for over 6 years now and I can tell you that a lot of the ordered ABGs are nonsense that are just really meant to make the clinical staff feel better.. I’ve questioned ABG orders too many times that I care to count and when I did, many were canceled. There is a time and a place for an ABG but when a rapid medical intervention is needed, a close assessment of your patient and a good clinical judgment will always be superior to an arterial blood gas.
And what about hypercarbia and respiratory acidosis in obstructive patients? and in known chronic COPD patients with a story of hypercapnia and acidosis when they actually “compensate” and get a normal pH with high bicarbonate levels (we strive not to ventilate this kind of people, but we place them on low-flow O2 even hypercarbic…)
Pulse oximetry tells you nothing about PaCO2, pH, or ventilation. In order to get that sort of information you need either ABG, VBG, or end tidal CO2… which is another debate entirely… hopefully we will go there soon but not in this post.
Bill Brewer Great article…but though clearly stating ” oxygenation” several time the Premise of why an abg is drawn is wrong..we don’t usually use abg to monitor o2 unless the pulse ox issss unreliable…we draw abgs to determine ventilation..he refrences low pao2 and bipap several times bipap is not for oxygenation cpap is..as rts we often have that conversation….serial abgs are drawn for ventilation not usualy oxygenation..also yes it’s a snap shot butttt as I already said its about ventilation..drawing a baseline gas is usually to see if they have an elevated bicarbonate to destigish between an acute, chronic, or… Read more »
The fact of the matter is that millions of abgs are ordered reflexively based on calls from nurses, etc that “we can’t keep the patient’s sats up” or similar report. It is true that it is often ordered to “buy time” to think through the process, especially if the physician isn’t by the bedside. In fact, I would argue that face to face encounters between the patient and MD should drastically reduce the number of “needed” abgs, especially if you don’t have a POC blood gas machine (which we don’t in our hospital and get by just fine). Bedside evaluation… Read more »
I am trying to figure why Dr. Farkas wrote DO2 = 13.4(cardiac output)(hemoglobin)(oxygen saturation)
instead of DO2 = 1.34…
Can’t find out.
Misspelling?
Regards, C.
I don’t think this is a mistake. When you derive these equations, a factor of 10 ends up getting added along the way to make the units work (involved in conversion from ml/dL to ml/L). For the equation as written in the blog, I’m using the following units:
DO2 measured in ml/min
CO measured in liters/min
HgB measured in mg/dL
O2 sat has no units (should generally be close to 1)
yes agreed abg’s can be helpful for ventilation though you do understand this is largely not necessary in many of our pts for ie the pt you want to extubate who has good mental status breathing comfortably etc. And many people I know focus too much on the oxygen variables of an abg. The bicarb is calculated not measured, and you can get this on VBG as well. As far putting pulse ox on forehead maybe you are misinformed because there is a nice study comparing finger, earlobe and forehead pulse ox with the latter 2 being way more accurate… Read more »
What i forgot: wonderful article, many thanks.
Excellent article, as usual, from Dr. Farkas. I would just want to point out that the DO2 formula (DO2 = 10* 1.34(cardiac output)(hemoglobin)(oxygen saturation)) is missing the + 10 * 0.003 *PaO2 (mmHg) * cardiac output (L/min) component, which is both trivial and important. It is trivial, because it doesn’t contribute much at normal atmospheric pressures (and that’s why it’s usually not mentioned). It is also important for the same reasons: to show people that SaO2 matters much more when talking about oxygen delivery. Normal DO2 on room air = 10 *(1.34 * 5 * 14 * 1 + 0.003… Read more »
Excellent points, thanks. Directly dissolved oxygen (independent of hemoglobin) may also become a significant factor in patients with profound anemia (e.g. hemorrhage in a patient who is a Jehovah’s Witness, leading to a situation where the patient has extreme anemia).
Mr. Brewer,
You will get much further in an academic discussion if you use proper English, grammar, punctuation, and tact. As a side note, there are pulse oximeter probes that are made for the forehead and they generally work much better on patients that are very ill. Follow the link below for an example of such.
http://www.medtronic.com/covidien/products/pulse-oximetry/nellcor-spo2-forehead-sensor
Regards,
Derek
Yes!!!
The Sat is what matters for oxygen delivery. I don’t care what the Pao2 is most of the time, as long as the sat is good and the Pao2 isn’t 300. Somebody should make people who ask for a gas on an awake, oriented patient to try it on themselves.
Its annoying that some people think that you have to frequently check ABG’s just to find out what the Pao2 or PaCo2 are. Just asses the patient’s mental status, work of breathing, etc. capnography, and spo2.
Amen. Or maybe we could require the ordering doc to pay a $20 penalty for ordering an ABG. I bet people would rapidly figure out how to manage patients without ABGs.
While 5 is correct, a clarification: the machines don’t entirely assume a normal curve, but rather they calculate the curve based on the measured CO2 and pH. This curve is still an estimation, as it doesn’t include the influence of 2,3DPG or dyshemoglobinemia, it still gives you an approximation of where they are on the oxyhemoglobin dissociation curve. If you’re smart, you can take this calculation back to where you’re measuring pulse oximetry and puzzle out why these two numbers may be different. Perfusion? Anatomical shunting? Dyshemoglobinemias?
Thanks so much, you don’t know hiow many eye rolls I get in our hospital when reciting these facts, including from other physicians.
Printing… 😉
Thank you Doc for posting this (sometime ago now). Remote medics such as myself do not typically have access to a lot of the high tech clinical tools typical of a Western hospital so the importance of knowing the capabilities and limitations of all assessment tools and strategies cannot be overstated. I also appreciate the comments affirming and also challenging your well researched thoughts on this topic. The risk to benefit ratio for ABG as compared to SpO2 is one thing that stood out to me in this paper as well as the obvious “treat the patient, not the… Read more »
While this article is fantastic and is a great resource to those of us trying to get these points across, I feel it is missing the due diligence of the value an appropriate ABG can have. The biggest reason i advocate for an abg is the mechanically vented patients I worry are over oxygenated. In all patients there’s no reason, besides pts on RA, to saturate above 95 and yet every profession seems to chase that 100%, especially in the ER. While SpO2 does benefit in all the ways explained in this article, there is the fact that it is… Read more »
why is this circle here???
CORRECTION: 12/22/20
to ADDENDUM 12/21/20: “New research shows that pulse oximetry may have a bias of +2% in patients with darkly pigmented skin. This could cause clinical errors in patients with borderline oxygen saturation (e.g. ~90%).”
This study found SpO2 bias was +3% vs ABG median in people who self identified as blacks and +1% in whites, with 2% difference between them. Notably, all SpO2 measures for whites from 89 to 96% were within +/- 3%of ABG as US FDA requires, but only half of black measures were (at any level!). It did not assess or report results by pigmentation.
I’ve had an issue with a couple COVID patients in the ICU where a pulse ox reading on the finger reads 60-70%, and a reading on the earlobe reads above 90%. Good pleth waves on both sites. Both appeared alert, calm and were watching TV. ABG was ordered on one patient and the PaO2 was in the 30s, and they were intubated, even with their presentation.
I know every patient is unique, but I’m just wondering which pulse ox reading to trust with our patients, especially with all that we need to consider for treating patients with COVID.
Jacob, intubation is not required in that situation, even if positive pressure ventilation is needed. You see, mechanical ventilation can be provided using bi-level settings and a non-invasive mask. Intubation, and tracheostomies, are rarely needed to provide oriented patients the breathing support they need in the hospital or at home/community settings.
Thanks for a great article. I have noted in several instances where oxygen saturation on pulse oximetry does not correlate with oxygen saturation on an ABG eg. it is 89% on pulse ox but the ABG shows a high PaO2 with oxygen saturation say 98-99%. I have noted this more during the pandemic for some reason. Any insights on this? Would you still go with the pulse oximetry in this situation?
Oh my goodness this article had me chuckling, what a great read! Almost every point helped me understand whole new concepts I haven’t been exposed to before.
Really useful piece of information. I was sent home from hospital on ambulatory O2 at 4lpm, from continuous at 1Lpm. After 60 mins of O2 my paO2 was >7.3kpa but my SpO2 was 86-93% HR 90-100. Therefore, I didn’t meet the guidelines for continuous O2 at home (<7.3kpa or 8.0 I’d oedematous). On waking my first morning home 9 hrs without O2) my SpO2 was 77% but o was told, this was not significant, that despite having a headache, high HR and feeling wobbly. Because my PaO2 was fine 20 hours earlier, I was not hypoxic!!! When asked, how do… Read more »
Hi Josh, this is great topic for my residents with great insight.
quite often there is significant discrepancy between SpO2 and SaO2. Which one do you believe is more accurate. I have scoured the literature but everyone seems to keep on comparing both. But in reality, we are comparing SpO2 to a calculated value from PaO2.
Is there any study which compared “real oxygen sats” to SpO2 ?
[…] PulmCrit-Top 10 Reasons Pulse Oximetry Beats ABG for Assessing Oxygenation […]
[…] PulmCrit-Top 10 Reasons Pulse Oximetry Beats ABG for Assessing Oxygenation […]