
Introduction
ARDS causes shunting of deoxygenated blood through the lungs. Most therapies for ARDS naturally combat this shunting (e.g. opening alveoli with PEEP). However, there is often a limit to which pulmonary shunting is treatable.
Jujitsu is a Japanese martial art based on flexibility and technique, rather than a directly confronting an opponent with force. In the spirit of jujitsu, this post explores how to support ARDS patients without directly confronting lung dysfunction. This is useful in refractory ARDS, when frontal assault has failed.
 Part 1: Understanding the physiology
Part 1: Understanding the physiology
Basics: systemic oxygen delivery
The amount of oxygen delivered to the body (DO2) is calculated with the equation below. Oxygen delivery results from a synergy of cardiac, pulmonary, and hematologic function:
![]()
Oxygen extraction ratio (O2ER) is a ratio of the body's oxygen consumption (VO2) compared to the systemic oxygen delivery (DO2, formula below). A normal O2ER is ~25%. If oxygen delivery decreases, the O2ER increases as tissues extract more of the delivered oxygen. O2ER is a nice way to describe the adequacy of systemic oxygen delivery.
![]()
Shunt oxygenation equations
The core physiologic abnormality in ARDS is shunting of blood through the lungs. We must understand how cardiac, pulmonary, and hematologic variables will affect oxygenation in this situation. Takala 2007 derived equations to describe this: (1)
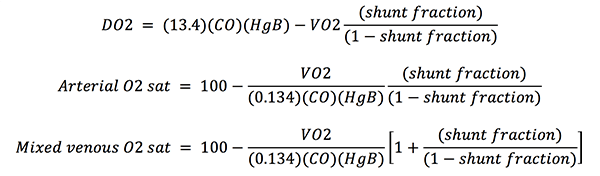
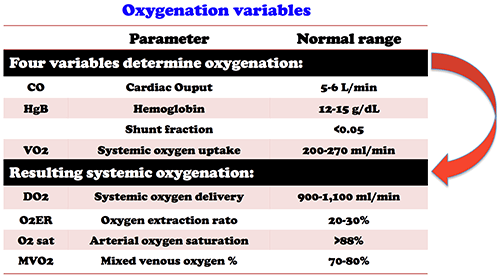
The associated units and normal ranges are as follows.
Shunt oxygenation equations: Understanding the variables
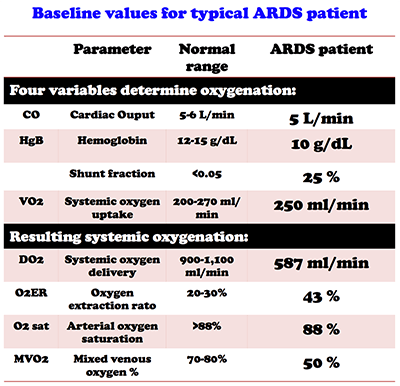 Let's start by imagining a typical ARDS patient with baseline values as shown here. The next sections examine the effects of adjusting each variable. Some trends will become apparent:
Let's start by imagining a typical ARDS patient with baseline values as shown here. The next sections examine the effects of adjusting each variable. Some trends will become apparent:
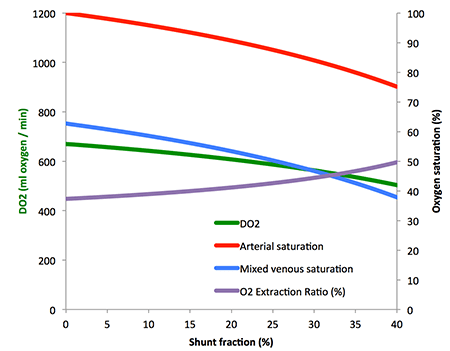
- Shunt fraction directly affects arterial oxygen saturation.
- Optimizing cardiac output, hemoglobin, and VO2 indirectly improves arterial oxygen saturation, secondary to increasing the mixed venous oxygen saturation (if the mixed venous oxygen saturation is higher, then blood shunting past the lungs will contain more oxygen).
Cardiac output & Hemoglobin

The figures above show the effect of changing either the cardiac output or hemoglobin on oxygenation. These variables have neighboring positions in the oxygenation equations, so they behave similarly. Cardiac output and hemoglobin both have strong effects on the DO2 and O2ER. Increasing cardiac output and hemoglobin concentration also increases arterial oxygenation saturation, but to a lesser extent.
Systemic oxygen utilization (VO2)

Reducing VO2 causes a mild improvement in arterial oxygen saturation and DO2. However, the strongest effect of VO2 is to directly drive the O2ER:
![]()
Shunt Fraction
Most therapies for ARDS focus on reducing the shunt fraction (e.g. PEEP, proning, APRV)(2). The shunt fraction is the variable with the greatest effect on arterial oxygen saturation. However, of all variables, shunt fraction has the weakest effect on the O2ER.
Shunt oxygenation equations: Understanding complex interventions
We can now build on this background, to understand more complex therapies.
Inhaled pulmonary vasodilator
An inhaled pulmonary vasodilator may:
- improve ventilation-perfusion matching, increasing the arterial oxygen saturation.
- reduce afterload on the right ventricle, increasing the cardiac output.
This is a win-win, explaining the ability of pulmonary vasodilators to stabilize some crashing ARDS patients.
Increased airway pressure (e.g. increased PEEP, APRV)
This may have positive and negative effects:
- Increased airway pressures may open alveoli, thereby reducing the shunt fraction (3).
- Increased airway pressure may reduce cardiac output (due to reduced preload and increased pulmonary vascular resistance)
The balance of these effects is complex. However, it must be recognized that even if increased airway pressures improve the shunt fraction, depression of cardiac output can have a dominant effect on the DO2 and O2ER. For example, if PEEP reduces the shunt fraction from 25% to 10% while reducing the cardiac output from 5 L/min to 4 L/min, the net effect is to reduce systemic oxygen delivery:
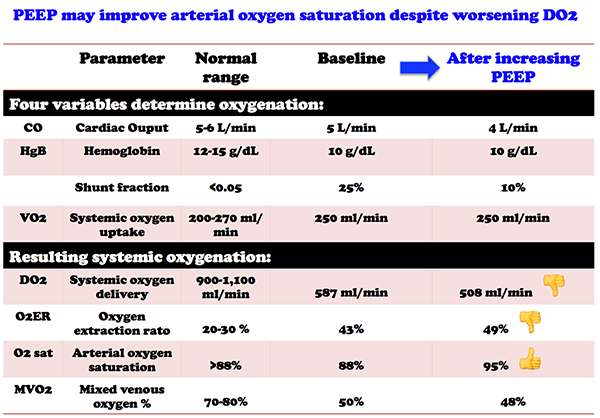
We've all encountered this situation, when increased PEEP improves the patient’s arterial saturation but drops the blood pressure. In this case PEEP appears beneficial, but it is probably reducing systemic oxygen delivery.
 Low tidal volume ventilation
Low tidal volume ventilation

The classic ARDSnet 2000 trial demonstrated mortality benefit from 6 ml/kg tidal volume ventilation compared to 12 ml/kg tidal volume ventilation. This led to the religious adoption of 6 ml/kg tidal volume ventilation. However, its unclear why lower tidal volumes improved outcome (low volume? low plateau pressure? low driving pressure?)(4).
Natalini 2013 exposed 16 ARDS patients sequentially to both 6 cc/kg and 12 cc/kg tidal volume ventilation. Low tidal volume ventilation significantly improved O2ER, due to improvements in the cardiac output (figure below)(14). Re-examination of the original ARDSnet study confirms that patients treated with low tidal-volume ventilation experienced more days without circulatory failure (19 vs. 17, p = 0.004). Thus, it's conceivable that low tidal volume ventilation is beneficial largely because it improves perfusion. If true, this might suggest that we should worry less about tidal volumes and worry more about perfusion.

Oxygenation goals: What are we chasing now?

 Oxygenation monitoring is similar to hemodynamic monitoring. Arterial saturation, like blood pressure, is the easiest value to obtain. These measurements are universally obtained on all patients, so we are quite comfortable with them.
Oxygenation monitoring is similar to hemodynamic monitoring. Arterial saturation, like blood pressure, is the easiest value to obtain. These measurements are universally obtained on all patients, so we are quite comfortable with them.
Arterial oxygen saturation is a measurement of lung function, but it's not a good measurement of systemic oxygen delivery (DO2, O2ER). DO2 depends on the trifecta of lung, cardiac, and hematologic function, with lung function (~ arterial saturation) being only one third of this. We have already seen examples where arterial saturation didn't correlate well with systemic oxygen delivery:
- Cardiac output, hemoglobin, and VO2 have a strong effects on O2ER, but little effect on arterial saturation.
- Shunt fraction has a strong effect on arterial saturation, but little effect on DO2 or O2ER.
- It is possible to improve the arterial saturation despite decreasing the DO2 (e.g. excessive airway pressures).
Systemic oxygen delivery (DO2 and O2ER) has similarities with cardiac output and cardiac index. From a physiologic standpoint, these seem like the most important variables. Unfortunately, they are hard to monitor. Thus, we usually don't check them. When we do measure them, its unclear exactly what value we are targeting.
Do we pay too much attention to arterial oxygen saturation?
 We often focus on minor variations in the arterial oxygen saturation. For example, a saturation of 90% may be regarded as “good” whereas 85% is “bad.” It is commonly believed that if the saturation falls under 88%, the patient will spontaneously burst into flames.
We often focus on minor variations in the arterial oxygen saturation. For example, a saturation of 90% may be regarded as “good” whereas 85% is “bad.” It is commonly believed that if the saturation falls under 88%, the patient will spontaneously burst into flames.
Like any diagnostic test, arterial oxygen saturation requires clinical context. For example, an arterial saturation of 85% on six liters nasal cannula may be a baseline value in a patient with idiopathic pulmonary fibrosis. However, this same oxygen requirement in the context of an acute asthma exacerbation would be alarming.
Excessive focus on arterial saturation may drive excessive use of interventions which reduce the shunt fraction. These interventions carry substantial risks (e.g. increased airway pressures may cause barotrauma and shock, elevated FiO2 may cause lung toxicity).
Oxygen extraction ratio (O2ER): Closer to the truth?
![]()
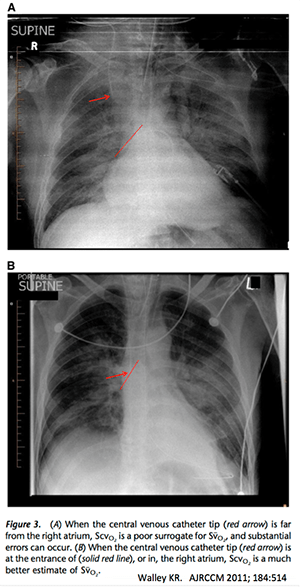 DO2 and O2ER are better measurements of systemic oxygenation, but harder to monitor. O2ER may be the most easily measured (5). Many patients have a central venous catheter placed in the superior vena cava. This can be used to estimate the mixed venous saturation, with debatable accuracy (Beest 2011).
DO2 and O2ER are better measurements of systemic oxygenation, but harder to monitor. O2ER may be the most easily measured (5). Many patients have a central venous catheter placed in the superior vena cava. This can be used to estimate the mixed venous saturation, with debatable accuracy (Beest 2011).
A simple approach to more accurately measure O2ER may be to place a central line deeper than usual, so that its tip sits in the right atrium (6). This is safe. The saturation in the right atrium is close to the mixed venous saturation (7). Of course, definitive measurement of the mixed venous saturation could be performed using a pulmonary artery catheter.
The greatest limitation of O2ER may be that there is little experience using it as a monitoring tool in ARDS. The target O2ER remains unclear. Some sources suggest that a target should be below 50% (8). However, this probably doesn't work in patients with ARDS plus sepsis (wherein microvascular and mitochondrial dysfunction reduce the O2ER).
Bottom line on oxygenation goals?
The vast majority of ARDS patients respond well to conventional therapies, guided by arterial oxygen saturation. In these patients, there is probably little benefit from monitoring O2ER.
However, occasional patients will develop refractory ARDS which doesn't respond to conventional therapy. This is largely an evidence-free zone, too rare to study well. For patients failing conventional therapy, measuring and optimizing O2ER may be a physiologically sensible approach.
Improving systemic oxygen delivery via adjusting VO2, CO & HgB: Is there any evidence?
 (1) Interventions to reduce VO2
(1) Interventions to reduce VO2

 Paralysis improved the adjusted mortality in one RCT (Papazian 2010)(13). This could reflect better ventilator synchrony. Another possible explanation is that paralysis decreases VO2 by reducing the oxygen utilization of respiratory muscles (Marik 1996, figure above). Reducing VO2 could metabolically off-load the cardiopulmonary system, improving the O2ER and facilitating oxygen delivery to vital organs. Short of paralysis, deeper sedation may also reduce VO2.
Paralysis improved the adjusted mortality in one RCT (Papazian 2010)(13). This could reflect better ventilator synchrony. Another possible explanation is that paralysis decreases VO2 by reducing the oxygen utilization of respiratory muscles (Marik 1996, figure above). Reducing VO2 could metabolically off-load the cardiopulmonary system, improving the O2ER and facilitating oxygen delivery to vital organs. Short of paralysis, deeper sedation may also reduce VO2.
Fever control can cause a dramatic reduction in VO2 (adjacent figure). Thus, something as simple as acetaminophen could reduce VO2 and improve O2ER. The benefit of antipyretics among ICU patients is debatable (Young 2016). Nonetheless, fever control is safe and might be beneficial in a minority of patients with tenuous systemic oxygenation.
(2) Interventions to increase hemoglobin
 Avoid nonessential labs It's tempting to order tons of ABGs on ARDS patients, but this is rarely beneficial (9). The presence of an arterial catheter correlates with greater blood removal for labs, so placing a catheter to “facilitate frequent ABGs” is dangerous (Tarpey 1990). Mindless cycling of other labs should be curtailed. You're not going to win a gold medal for making all the labs euboxic.
Avoid nonessential labs It's tempting to order tons of ABGs on ARDS patients, but this is rarely beneficial (9). The presence of an arterial catheter correlates with greater blood removal for labs, so placing a catheter to “facilitate frequent ABGs” is dangerous (Tarpey 1990). Mindless cycling of other labs should be curtailed. You're not going to win a gold medal for making all the labs euboxic.

Transfusion? Available evidence on transfusion in ARDS has been negative or neutral. This isn't surprising, as most patients with ARDS have adequate systemic oxygen delivery. It remains unknown whether transfusion could benefit selected patients with insufficient systemic oxygen delivery.
(3) Interventions to increase cardiac output (CO)
Inotropes Dobutamine has the following effects:
- Increased systemic oxygen delivery: increased DO2, decreased O2ER, increased mixed venous oxygen saturation.
- Pulmonary vasodilation may worsen ventilation-perfusion matching in the lung, causing a slight decrease in arterial oxygen saturation (10).
Dobutamine might be beneficial in the sickest ARDS patients, who have very low mixed venous oxygen saturation and high shunt fraction (11).
The future: Permissive arterial hypoxemia?
What about the patient whose oxygenation can't be improved despite maximal conventional therapy and optimization of CO, HgB and VO2? For example, imagine this patient with severe ARDS at a non-ECMO center:
 There might be a temptation to try high-frequency oscillatory ventilation, a therapy proven to increase mortality (Ferguson 2013)(12). However, the O2ER is low, suggesting adequate systemic oxygenation. Thus, the best approach here might be to continue current management, rather than pursuing dangerous interventions to increase the arterial oxygen saturation (Martin 2013). However, there is currently no evidence to support this strategy of permissive hypoxemia.
There might be a temptation to try high-frequency oscillatory ventilation, a therapy proven to increase mortality (Ferguson 2013)(12). However, the O2ER is low, suggesting adequate systemic oxygenation. Thus, the best approach here might be to continue current management, rather than pursuing dangerous interventions to increase the arterial oxygen saturation (Martin 2013). However, there is currently no evidence to support this strategy of permissive hypoxemia.

- Four variables determine systemic oxygen delivery in ARDS:
- cardiac output
- hemoglobin concentration
- systemic oxygen consumption (VO2)
- fraction of blood shunted through the lungs without being oxygenated
- Therapies for ARDS focus on reducing the shunt fraction (e.g., PEEP, proning, APRV). Patients with refractory shunting will be refractory to these therapies.
- Among patients with refractory ARDS, manipulations of other variables could improve systemic oxygen delivery:
- reduced systemic oxygen consumption (paralysis, temperature control)
- increased hemoglobin concentration (blood conservation, possibly transfusion)
- increased cardiac output (inotropes)
- Arterial oxygen saturation is not a reliable measurement of systemic oxygen delivery (DO2).
- It's notable how little we know about oxygenation goals when treating ARDS. Over-emphasis on normalizing arterial oxygen saturation may be leading us astray.
Notes:
- This derivation is based on simple algebraic manipulations of the Fick equation. It is assumed that dissolved oxygen not bound to hemoglobin has no significant effect on the oxygen content of the blood. This is a reasonable assumption unless the patient has an extraordinarily low hemoglobin.
- In reality hypoxemia is often due to a combination of shunting and ventilation-perfusion imbalance. In order to mathematically model lung oxygenation, these equations divide blood flow into two components: a “shunt fraction” which participates in no gas exchange, and a “perfused fraction” which is saturated to reach 100% saturation. This is a simplification of reality, wherein some blood passing through the lungs may be partially oxygenated (e.g. due to ventilation-perfusion mismatch). Thus, the “shunt fraction” in these equations doesn't correlate precisely with blood passing through consolidated lung tissue. Furthermore, improving the patient's ventilation-perfusion matching (e.g. using inhaled pulmonary vasodilators) will improve the mathematical “shunt fraction.”
- However, in a patient with a patent foramen ovale (PFO), it is possible for an increase in right-sided pressure to increase shunting through the PFO and thereby increase the shunt fraction. Patients with PFO may respond beautifully to inhaled pulmonary vasodilators (which reduce shunt via the PFO) but poorly to increased airway pressures (which increases shunting via the PFO). If you think you might be encountering this physiology, a simple bedside echocardiographic microbubble study can quickly determine if there is intracardiac right-to-left shunting.
- The gold standard in medicine for proving the utility of an intervention is the RCT, which ideally manipulates one variable while using randomization to control for all other variables. This is, quite simply, impossible with ARDS because manipulating any variable on the ventilator causes variation in a number of other variables. Thus, proving causation is impossible (for example, it has not been proven that reduced tidal volumes cause reduced mortality — it is equally possible that low plateau pressures reduce mortality). Without understanding why 6 cc/kg tidal volumes were beneficial in this study, it is impossible to generalize these results to other clinical contexts (e.g. patients with higher PEEP, patients on APRV).
- An alternative approach would be to calculate DO2 based on the arterial oxygen saturation, hemoglobin, and cardiac output (e.g. measured via echocardiography). However, accurate measurement of cardiac output in ARDS patients via transthoracic echocardiography can be technically challenging. Additionally, this approach requires estimating VO2 or measuring it by indirect calorimetry.
- For example, in an average-sized patient a central line placed 20cm deep in the right internal jugular position is likely to lie in the right atrium. If available, real-time echocardiographic imaging of the heart may assist in positioning. Chest radiography may also help confirm position relative to the heart. Clinical studies have demonstrated a close relationship of right atrial and mixed venous saturation regardless of how the line position is confirmed (e.g. via echocardiography or fluoroscopy).
- Alkhouli 2014, Cavaliere 2014, Kopterides 2009, Gutierrez 2007, Edwards 1998.
- O2ER >50% is typically quoted in the literature as correlating with hypoperfusion, lactic acidosis, and poor outcomes (Walley 2011, Natalini 2013, Orlov 2009, Park 2015). Unfortunately, use of this as a resuscitation target has not been validated prospectively.
- If the pulse oximetry waveform is adequate, that should be fine for monitoring arterial oxygenation. Based on the concept of permissive hypercapnia, the exact PaCO2 isn't mission-critical. Cycling ABGs often leads to endless minor adjustments on the ventilator, without meaningful improvement in the patient's condition.
- Any intravenously administered agent that causes pulmonary vasodilation will cause diffuse pulmonary vasodilation, which impairs ventilation-perfusion matching (because it vasodilates capillaries in areas of lung that are receiving no ventilation).
- As explored previously, individual patient responses to dobutamine are variable. Thus, if dobutamine were used, O2ER should be monitored to confirm that it is working as intended.
- High frequency oscillatory ventilation appears to improve shunt fraction and arterial oxygen saturation while reducing the cardiac output. Overall, this may have no significant effect on DO2 or O2ER (Velmahos 1999). Lack of benefit on systemic oxygen delivery may explain why recent RCTs have failed to find a benefit in high-frequency oscillatory ventilation.
- Use of adjusted mortality as an outcome in an RCT might be a bit questionable, given that randomization is supposed to create well-balanced groups.
- Note how many patients in the high tidal-volume group have O2ER > 50%. As discussed below, an O2ER above 50% is quite high, suggesting borderline or frankly insufficient systemic oxygen delivery.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Thanks for another great post.
What do you think of lactate as marker of tissue hypoxia, to evaluate therapeutic intervventions as respirator settings, pressors etc. To me it seams as better measure than o2ER.?
Even in ARDS, the most common cause of elevated lactate levels is probably aerobic generation of lactate due to endogenous catecholamines or exogenous epinephrine (discussed further here: https://emcrit.org/pulmcrit/understanding-lactate-in-sepsis-using-it-to-our-advantage/). Truly inadequate systemic oxygen delivery is relatively uncommon. So I’d be careful about assuming that an elevated lactate indicates insufficient systemic oxygen delivery. The other problem with using lactate as an indicator for how patients respond to therapeutic interventions is that it may lag a bit behind the patient’s current physiology.
But might it not be so that two patients with an identical DO2 might still have important differences in O2 diffusion at the cellular level because of a differing partial pressure gradient? Especially because at the upper (flat) part of the oxygen-hemoglobin saturation curve a small change in saturation implies a large change in pO2, which drives oxygen diffusion at the cellular level. Simplified example: DO2 might be equal for a patient with CO 5L/min with O2Sat 80% versus CO 4L/min with O2Sat 100%, but I can imagine the second might still have better interstitial / cellular oxygenation because of… Read more »
Gas exchange at well perfusion tissue should be evenly, which means the PO2 in blood will equal to which in tissue at the end of gas exchange.Thus, there is no “diffusion rate problem” unless the perfusion or gas exchange is suppressed.On the other hand, if only the SaO2 change could physiologically diminish the gas exchange in tissue level,all other parameters would be useless.And we have no need to discuss which management would be better.
Using O2ER makes sense to me. After all it´s just another way of expressing DO2/VO2-relationship and as such probably helpful to summarize the net effects on oxygen delivery of a given treatment (eg norepi) without having to look at all the single variables (MAP, HR, SpO2 …). I am surprised however that S(c)vO2 alone has fallen out of favour so much, since it is also just a simplification of O2ER. If you have a SvO2 of say 60%, your O2ER can hardly be higher than 40%. So why do we “like” O2ER to help us make decisions and at the… Read more »
A few decades ago there was a big push to examine oxygen delivery and svcO2 in sepsis. svcO2 was popularized by the Rivers trial and EGDT for sepsis. Ultimately this didn’t pan out, which may have left folks with a negative bias towards svcO2. The failure of these strategies in septic shock may be explained by a few features (1) Truly inadequate systemic oxygen delivery in sepsis is extremely rare. (2) Septic shock may be a poor situation to use svcO2 or SvO2, because systemic microvascular dysfunction may cause shunting. This may increase the global svcO2, despite the fact that… Read more »
Josh, that was a beautiful description of relevant physiology! In particular, the bit about Patent Foramen Ovale (PFO) is something close to my heart. I believe that the possibility that a PFO exists in upto 30% of the general population, is very often overlooked in routine clinical practice in ICUs. It is my humble opinion that very often this is what causes a sizeable proportion of our hypoxemic patients to not respond to regular recruitment measures. These are also our PEEP non-responders. I am also daring to believe that this is probably why trial after trial on HFOV as a… Read more »
Thanks. Completely agree with you. I will routinely do echo bubble studies on patients if their shunt/hypoxemia seems to exceed what I would expect based on their imaging (takes about five minutes with a bedside echo, a few trainees, and a three-way stopcock). Usually these are negative, but every once in a while they’re positive. A positive bubble study would bias me towards considering inhaled vasodilator (i.e. epoprostanol) and away from attempts to aggressively increase airway pressure (i.e. APRV). The subset of ARDS patients with patent PFO probably do respond to interventions differently than most patients. It would be nice… Read more »
the example of a mixed venous sat of 14% probably not physiologically possible as there is a significant percentage of oxygen that is non-consumable, i.e. that 02 below a mixed venous p02 of 20 or a mixed-venous sat of 32% at ph 7.4 and 27% at ph 7.3, and 20.3 at ph 7.1 and 15.7 at ph 6.9.
Mark Farber, M.D
Professor of Medicine, Physiology and Biophysics
Indiana University School of Medicine
[…] PulmCrit-Fighting Refractory ARDS with Physiologic Jiu Jitsu […]