

Introduction with a case
Once upon a time at Genius General Hospital, I arrived a bit early for a shift. The outgoing attending was happy to see me: “Hi Josh, you got here just in time to intubate the patient in Bed 8. He was supposed to get an upper endoscopy with ketamine sedation, but he couldn't be sedated.”
The patient in Bed 8 was a 40-year-old man with a history of alcoholism, currently presenting with an upper GI bleed. He had received 130 mg of ketamine (2 mg/kg), which caused him to become partially dissociated and mildly agitated. Airway equipment was at the bedside and preparations were underway to perform intubation.
Instead of proceeding with intubation, I decided to attempt giving more ketamine. We gradually up-titrated the ketamine dose in increments of 70-100 mg. He ultimately required a total of 500 mg IV ketamine in order to reach full dissociation (~8 mg/kg). Endoscopy was performed without problems and his recovery was uneventful.
The clinical phenomenon of ketamine tolerance
This is one of about a half dozen patients I've encountered with ketamine tolerance. These patients do not fully dissociate at 2 mg/kg, a dose which should be adequate. Tolerance can be overcome by using higher doses of ketamine (e.g. 400-600 mg IV in divided doses).
Ketamine tolerance seems to be limited to patients with a history of substance or alcohol abuse. Unfortunately I haven't been systematic about obtaining rigorous histories in these patients, so I'm not sure.
This phenomenon isn't widely reported in the literature or well known among clinicians. Most guidelines and review articles indicate that a dose of 2 mg/kg will reliably cause dissociation (e.g. Green 2011).
The ketamine-tolerant patient presents a quandary to clinicians who aren't familiar with this phenomenon. The first time I encountered this, I was baffled and aborted the procedure after giving 200 mg ketamine. Eventually I realized that the drug isn't “failing” to work, but rather we are failing to administer a sufficiently high dose.
Evidentiary support for ketamine tolerance
Two reports from the 1980s documented the development of tolerance to ketamine anesthesia among patients treated with repeated doses (Khan 1988, MacLennan 1982). These are both freely available online and reproduced here in full:

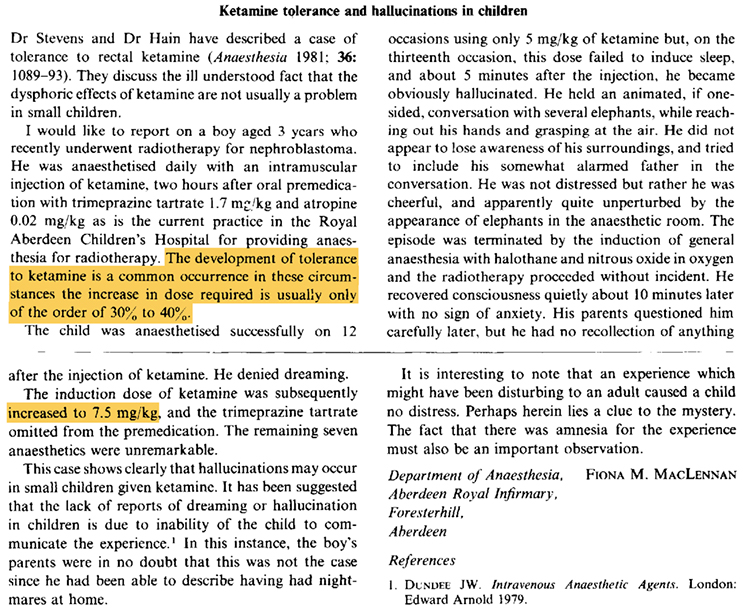
More recently, several reports have documented tolerance to ketamine's psychoactive effects (Bonnet 2015). This is a well-known phenomenon in the context of illicit ketamine abuse. Thus, the ability to develop tolerance to ketamine is established in the literature.
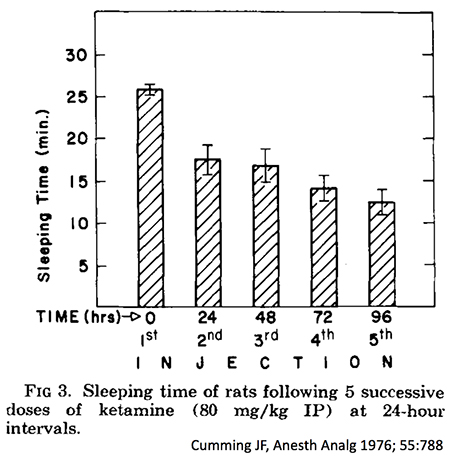
Ketamine tolerance has been proven to exist in rats and monkeys. Tolerance evolves rapidly in both species (figure below). Among rats, cross-tolerance exists between ketamine and fentanyl (but not morphine). This raises the possibility that cross-tolerance in humans could exist between ketamine and some synthetic opioids.
 Ketamine causes dissociation by inhibiting NMDA receptors. Other drugs which inhibit NMDA receptors include ethanol, gabapentin, nitrous oxide, dextromethorphan, methadone, and phencyclidine. It might be predicted that patients who use or abuse such substances would develop cross-tolerance with ketamine. Cross-tolerance between ketamine and either phencyclidine or ethanol has been demonstrated in animal models (Fidecka 1989; Wegner 1982; Rocha 1995).
Ketamine causes dissociation by inhibiting NMDA receptors. Other drugs which inhibit NMDA receptors include ethanol, gabapentin, nitrous oxide, dextromethorphan, methadone, and phencyclidine. It might be predicted that patients who use or abuse such substances would develop cross-tolerance with ketamine. Cross-tolerance between ketamine and either phencyclidine or ethanol has been demonstrated in animal models (Fidecka 1989; Wegner 1982; Rocha 1995).
The safety of high-dose ketamine
There is relatively little evidence in the literature regarding ketamine tolerance. However, there is substantial evidence that high doses of ketamine are safe. For example, intramuscular doses of 500 mg have been utilized for the management of agitated patients. The FDA-approved ketamine package insert recommends a dose of 9-13 mg/kg for intramuscular induction of anesthesia (1). The literature contains examples of inadvertent administration of massive doses of intravenous ketamine with minimal adverse effects (aside from prolonged dissociation; Green 1999).
The safety of ketamine is based upon its mechanism of action as a dissociative anesthetic. It's impossible to “over-dissociate” a patient: once they are dissociated, additional drug can't dissociate them further. This creates a ceiling effect on the neurologic action of ketamine. There may be some concern about hemodynamic effects of very large doses, because ketamine can cause catecholamine release (increasing the Bp) and also has some negative inotropic properties (potentially dropping the Bp). However, with gradual dose titration and hemodynamic monitoring this should be safe.
Ketamine to facilitate procedures in the “difficult to sedate” patient
We are sometimes called upon to perform procedural sedation for non-intubated patients with a history of being “difficult to sedate.” A common scenario is a patient with alcoholism who requires an endoscopy or bronchoscopy. Such patients often respond poorly to a traditional sedation regiment for endoscopy (midazolam and fentanyl), due to cross-tolerance between alcohol and benzodiazepines.
Ketamine monotherapy is a uniquely useful drug for this situation. Even in a patient with ketamine tolerance, eventually a high enough dose should achieve full dissociation. As discussed above there is little risk of “overdosing” the patient with ketamine. This is in distinct contrast to other commonly used agents (e.g. midazolam, fentanyl, propofol), where escalating doses do increase the risk of respiratory complications.
Some pitfalls to using ketamine for procedural sedation
In fairness, the following points should be mentioned:
- Bolusing ketamine may cause short and self-limited apnea (~30 seconds). This may be avoided by giving each dose gradually (e.g. 100 mg over a minute). As with any procedural sedation, the provider should be ready to provide a jaw thrust and a few breaths via a bag-valve mask if needed.
- According to textbooks, ketamine causes retention of airway muscle tone. However, I have seen patients with obstructive sleep apnea who develop airway obstruction following ketamine. This may be managed with basic maneuvers including airway repositioning and a nasopharyngeal airway (note that ketamine doesn't suppress vomiting, so patients who are fully dissociated can still vomit in response to placement of an oropharyngeal airway).
- Some individuals who abuse high-dose ketamine could conceivably develop a level of tolerance so great that they wouldn't dissociate even in response to large doses of ketamine (e.g. 10 mg/kg). I'm not aware of any evidence that this exists, but it might (2).
Thus, giving ketamine isn't entirely foolproof. However, when titrated with attention to airway and vital signs, it is very safe.
Ketamine tolerance & rapid-sequence intubation
When performing rapid sequence intubation, we generally give the patient a standard dose of sedative (e.g. 2 mg/kg ketamine) with the assumption that this will cause dissociation. Unfortunately, if this assumption is wrong, then it is possible for a patient to be paralyzed without adequate sedation. This is problematic regardless of what paralytic is used, but it is especially undesirable with rocuronium (because it is possible for the patient to have an extended period of paralysis with awareness).
There seem to be two main risk factors for awareness during rapid-sequence intubation using ketamine:
- History of substance abuse or alcoholism.
- Patient has intact mental status prior to intubation (e.g. patients who aren't that severely ill, who are being electively intubated to facilitate a procedure). Most critically ill patients are delirious prior to intubation, which provides some protection from awareness.
For patients with these risk factors, an alternative strategy is needed. This scenario can generally be managed nicely by a “delayed-sequence intubation“-style approach. Ketamine may be gradually up-titrated until the patient is dissociated. After the patient is dissociated, intubation may be performed with confidence that the patient is adequately sedated. A similar dose of ketamine may be repeated after 30 minutes to maintain sedation if rocuronium was used.

- Occasional patients are tolerant to ketamine. This seems to occur primarily among people with a history of substance or alcohol abuse.
- Ketamine tolerance doesn't mean that ketamine won't work. However, much higher doses of ketamine may be required to reach full dissociation (e.g. 400-600 mg IV).
- Ketamine remains an outstanding drug for the “difficult-to-sedate” patient, with the understanding that some patients may need more than others (like any other sedative).
Related
- The ketamine-brain continuum (Rubin Strayer)
- Clinical practice guideline for ketamine sedation (Green 2011 Ann Emerg Med)
- Ketamine (Chris Nickson, LITFL)
- Delayed Sequence Intubation (EMCrit)
- Rocketamine vs. keturonium for RSI (PulmCrit) – In some ways this prior blog may seem to contradict the current post, but they're written in reference to different patient populations & clinical scenarios.
Notes
- Intramuscular ketamine is 93% bioavailable, so presumably doses of 9-13 mg/kg IM would be equivalent to administration of a similar cumulative dose of IV ketamine in divided doses over several minutes.
- The recklessness of substance abusers and plasticity of the human brain almost certainly exceed the courage of physicians. Thus, someone is probably out there somewhere abusing ketamine at doses greater than any physician would have the courage to use. This level of tolerance (the “super-tolerant” patient), if it exists, is probably exceedingly rare.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Thanks for this interesting post. As an anaesthesiology resident I have seen a couple of patients with ketamine tolerance. All of these patients had been subjected to repeated ketamine administration in the context of chronic pain management, wound/burn care or procedural sedation. I believe that anaesthesiologists that practice in burn patient care will be very familiar with this phenomenon. I remember a burn patient who would simply and calmly just tell me he wasn’t dissociated until he was. What I noticed most was how short the duration of action for each bolus was.
Hey Josh, that was a great thought provoking post! Ketamine is incredibly useful for many ICU procedures, where there isn’t an effective alternative, However for procedural sedation in a difficult to sedate patient it may not be optimal. I have personally seen these effects described, especially during change of dressings in burns patients. These patients require a massive dose of ketamine and experience a particularly long recovery, during which their airway may be at risk. I’m not really convinced of the safety of these high doses, from personal experience and especially in an unprotected airway. Alcohol abuse is a known… Read more »
Anecdotally I have also found that alcoholics are more likely to have a dysphoric emergence reaction to ketamine. Has that been your experience as well?
Hey Josh,
I have encountered this phenomenon in acutely intoxicated patients. They mostly are intoxicated with ETOH or PCP, sometimes with coingestions. When they present as trauma in our bay, there is growing disinclination by clinicans to steer clear from Ketamine, since people don’t feel comfortable with IV doses over 2mg/kg. I think this is erroneous, and we can do better. My only concern is the hypersalivation with Ketamine, which could complicated matters in an intoxicated patient who needs to lay flat for CAT studies. Do you use glycop or atropine prophylactically? Would love to hear others input as well.
I looked at the literature about this a couple years ago. At that point there was no rock-solid evidence one way or the other. Most guidelines and reviews tended to recommend against use of an anti-sialogogue. I have used atropine in some cases where I was particularly worried about salivation. My impression (and this is anecdotal based on a few cases) is that the combination of atropine and ketamine had a tendency to drive up blood pressure (possibly due to a combination of tachycardia from the atropine and catecholamine release from the ketamine). My current practice is just to use… Read more »
Hi
this is old news down under for aeromedical folks doing psychiatric retrievals!
We’ve noted this issue 10 yrs ago when we started using ketamine sedation for psychiatric aeromedical missions.
here is a published case report as well as references to other cases
https://prehospitalmed.com/2016/04/06/high-dose-ketamine-sedation-of-an-agitated-patient-during-air-medical-transport/
of late Ive moved to using ketofol rather than increasing ketamine infusion/dosing.
Ketaminh
Minh, I should have known you’d be all over this. Fantastic post, thanks.
thank you, Josh
Perfect timing. Saw this just last week on a 16 yo 75kg post intubation for resp failure. He took 750 mg in about a 30 min transport. We were strongly considering substance abuse.
NRP, FP-C
PHI Air Medical
Had a patient who came in agitated with maxed out Precedex drip dose at 1.2, not even sedated, one bit. I pushed a dose of Ketamind he calmed down for 2 hours then give Ketamine again. I can’t believe the presumption that some people out there abuse this drug. Very good info.
Interesting post Josh on a drug that I’ve been using more frequently in the ICU (mostly for intubating the patient in shock and for refractory status asthmaticus). On a related topic, I would like to pick your brain on the titration and weaning of ketamine drips in intubated patients with status asthmaticus. In these patients, would you presume that tolerance and/or tachyphylaxis is inevitable after a few days on the drip? Have you had asthmatics who seemed to have no benefit from ketamine? And do you have any thoughts on the approach to weaning off ketamine drip on a patient… Read more »
I’m going to post an experience I had recently not because I have an explanation but because it doesn’t fit the already-unusual pattern described above. I had a very difficult to sedate patient with autism who needed to be sedated for a procedure. Ketamine naive, and not on any of the above listed medications. He was on high-dose antipsychotics at baseline, however, for what it’s worth. I gave him 5mg/kg IV ketamine without any apparent sedation. He had already been on high-dose dexmedetomidine and midazolam infusions. Could not assess partial dissociation based on his non-communicative baseline status. I ended up… Read more »
Hello! Ran into this post while trying to figure out why my 3rd & 4th Stabilization infusions for depression/anxiety/PTSD…the usual;) I weigh 106, am 5’4”, 44 yr old female. The highest amount of benzodiazepines I’ve taken in a day is 2MG clonazepam (0.5MG DOSAGE). It’s my anti epileptic (TN) & prevents panic attacks). I have NEVER felt a euphoria on any benzo or narcotic (non-IV). Hydromorphone 8MG does nothing. I don’t drink. Even with MMJ, I may get high 1/20 times, despite qnty, method or qlty.. I actually do have reverse neurotransmitter , ADD/ADHD & may possibly beon the spectrum… Read more »
I am retired but worked for 30 years as an anesthesiologist at a pediatric burn hospital in Galveston, Texas; we used ketamine extensively and often had patients who required high doses and some younger children could not be adequately sedated with very high doses; this occurred occasionally in patients with little previous exposure to ketamine; either clonidine (longer acting and cheaper) or dexmedetomidine potentiate ketamine and small doses can be very helpful as an adjutant
I’d like to speak with you about tolerance. I’m what you’re referring to as a super tolerant patient. It’s scary. Let me know if it’s a possibility to chat.