
This page is a compilation of all things Delayed Sequence Intubation (DSI)
The Delayed Sequence Intubation (DSI) Publication is in Ann Emerg Med 2014 and is currently available as FOAM (http://dx.doi.org/10.1016/j.annemergmed.2014.09.025)

DSI is one of 4 things that I think need to be used for cutting edge airway management in the critically ill

To See Information regarding these other Concepts
Come to the EMCrit Preox Page
Listen to the DSI Podcast (Ep. 137)
Podcast: Play in new window | Download (Duration: 20:56 — 19.2MB) | Embed
The Bottom Line Review of the DSI Paper
Figures and Thoughts from the DSI Publication
Here is the DSI Algorithm

Table 1 from the Paper

David Shriger Made this Excellent Figure for the Publication
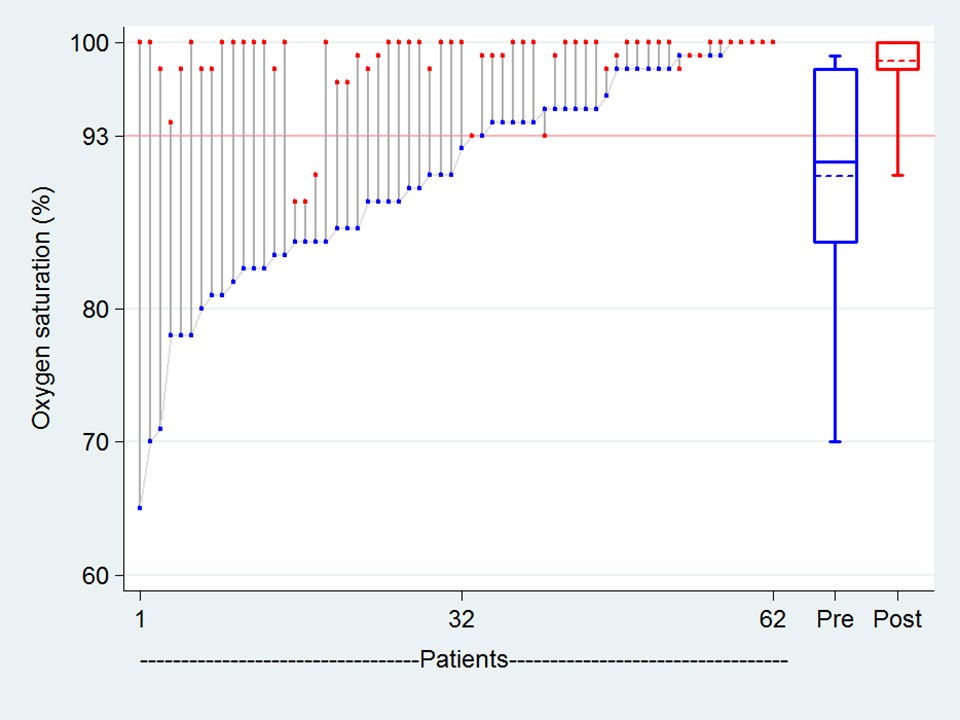
But the Patients I really cared about were the ones whose SpO2 was <=93% after maximal Preox Attempts. Here's how they did with DSI:

Additional DSI Resources
- EMCrit Podcast 40 was on the topic of DSI (but Ep. 137 is the superior version)
- Interview by my friend: Minh Le Cong interviewed me on DSI on his amazing PHARM Podcast. It is an additional 45 minutes on newest thoughts on DSI.
- Rob Bryant Implementing DSI
- Here is the reference for the incredible guidelines on ketamine in the ED.
Additional DSI Literature
- DSI In Kids (Case Report)
A Bit of Discussion
The Case
You have a 50 y/o male with bad bilateral pneumonia. BP 108/70, HR 96, RR 28. He is delirious, agitated, and looks sick, sick, sick! Saturation is 70% on a nasal cannula; when you try to place the patient on a non-rebreather (NRB) he just swats your hand away and rips off the mask. It is obvious to everyone in the room that this patient needs intubation, but the question is how are you going to do it?
Your first impulse may be to perform RSI, maybe with some bagging during the paralysis period. This is essentially a gamble. If you have first pass success, you (and your patient) may just luck out, allowing you to get the tube in and start ventilation before critical desaturation and the resultant hemodynamic instability. However, the odds are against you: bagging during RSI predisposes to aspiration, conventional BVM without a PEEP valve is unlikely to raise the saturation in this shunted patient, and if there is any difficulty in first-pass tube placement your patient will be in a very bad place.
A Better Way
Sometimes patients like this one, who desperately require preoxygenation will impede its provision. Hypoxia and hypercapnia can lead to delirium, causing these patients to rip off their NRB or non-invasive ventilation (NIV) masks. This delirium, combined with the low oxygen desaturation on the monitor, often leads to precipitous attempts at intubation without adequate preoxygenation.
Standard RSI consists of the simultaneous administration of a sedative and a paralytic agent and the provision of no ventilations until after endotracheal intubation (1). This sequence can be broken to allow for adequate preoxygenation without risking gastric insufflation or aspiration; we call this method “delayed sequence intubation” (DSI). DSI consists of the administration of specific sedative agents, which do not blunt spontaneous ventilations or airway reflexes; followed by a period of preoxygenation before the administration of a paralytic agent.(2)
Another way to think about DSI is as a procedural sedation, the procedure in this case being effective preoxygenation. After the completion of this procedure, the patient can be paralyzed and intubated. Just like in a procedural sedation, we want our patients to be calm, but still spontaneously breathing and protecting their airway.
The ideal agent for this use is ketamine. This medication will not blunt patient respirations or airway reflexes and provides a dissociative state, allowing the application of preoxygenation. A dose of 1–2 mg/kg by slow intravenous push will produce a calmed patient within ~ 30 seconds. Preoxygenation can then proceed in a safe controlled fashion. This can be accomplished with a NRB, or preferably in a patient exhibiting shunt, by use of a non-invasive mask hooked up to ventilator with a CPAP setting of 5-15 cm H20 (or some of the new masks that don't require a machine, but more on that soon). After a saturation of > 95% is achieved, the patient is allowed to breathe the high fiO2 oxygen for an additional 2–3 min to achieve adequate denitrogenation. A paralytic is then administered and after the 45–60 second apneic period, the patient can be intubated.
In patients with high blood pressure or tachycardia, the sympathomimetic effects of ketamine may be undesirable. While, these effects can be blunted with small doses of benzodiazepine and perhaps, labetalol (3), a preferable sedation agent is available for these hypertensive or tachycardic patients. Dexmedetomidine is an alpha-2 agonist, which provides sedation with no blunting of respiratory drive or airway reflexes (4-5). A dose of 1 mcg/kg administered over 10 minutes will lead to a sedated patient who will accept preoxygenation after 3-5 minutes in most cases.
Another advantage of DSI is that frequently, after the sedative agent is administered and the patient is placed on non-invasive ventilation, the respiratory parameters improve so dramatically that intubation can be avoided. In these cases, we then allow the sedative to wear off and reassess the patient's mental status and work of breathing. If we deem that intubation is still necessary at this point, we can proceed with standard RSI by administering a conventional sedation agent (e.g. etomidate or additional ketamine) in combination with a paralytic, as the patient has already been appropriately preoxygenated.
A video demonstrating the above concepts is at: https://emcrit.org/misc/preox/
A version of this article originally appeared in ACEP News.
- Walls RM, Murphy MF. Manual of emergency airway management, 3rd edn. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.
- Weingart SD. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. J Emerg Med2010 Apr 7. [Epub ahead of print]
- Aroni F, Iacovidou N, Dontas I, Pourzitaki C, Xanthos T. Pharmacological aspects and potential new clinical applications of ketamine: reevaluation of an old drug. J Clin Pharmacol 2009;49:957–64.
- Carollo DS, Nossaman BD, Ramadhyani U. Dexmedetomidine: a review of clinical applications. Curr Opin Anaesthesiol 2008;21:457–61.
- Abdelmalak B, Makary L, Hoban J, Doyle DJ. Dexmedetomidine as sole sedative for awake intubation in management of the critical airway. J Clin Anesth 2007;19:370–3.
Updates
- Prehosp Emerg Care. 2018 Feb 6:1-7. doi: 10.1080/10903127.2018 (Prehospital Doc DSI)
- Another Prehospital DSI Paper
- DSI RCT

Scott,
Had a sickie who aspirated likely secondary to ileus. Sats were in the garbage, <85%. Would DSI be the ideal way to intubate this tachypnic, agitated patient? My fear is that with a big nasty belly and placing on CPAP that you'd exceed the LES pressure and you could aspirate again. I know you talked about placing an NGT with ketamine but if sats were already trash would you still proceed this way? Much thanks!
I’ve had reasonable success with dexmedetomidine to facilitate NIV in the ED and ICU. Less concern about secretions, and the pharmacists and nurses at my institution tend to feel more familiar with it vs ketamine.
yep, great for NIPPV sedation and post-intubation sedation. Way too slow and not potent enough to treat agitated delirium in time for airway management.
Scott, I’m converted. Was a big fan of the original post and the principles and the physiology made a lot of sense to me when I originally came across DSI on your website. Since that post and this one it has bailed me out big time in resus with a case that scared the crap out of me. Got called to ED to an agitated, obese, alcoholic patient with severe pancreatitis and sepsis. pH of 6.9 from metabolic acidosis, massive respiratory compensation. This guy would not sit up, would not keep any kind of mask on and was pretty much… Read more »
Scott, great paper thanks for doing getting this out there! I’ll be bringing this up at our critical care journal club in conjunction with the paper below, we have a few anesthesiologists who still refuse to use PPV in an altered patient. We do essentially the same thing in the ICU with one caveat, we use HFNC at 70 L/min to maintain apneic oxygenation in the ICU before intubation. In order to maintain ventilatory mass flow there must be passage between your oxygen source and alveoli which can be maintained with low levels of PEEP +/- a jaw thrust. More… Read more »
Yes, the thrive article looked super interesting. You have touched on my trepidation=the mask seal. I’d love to see the video that will prove my fears unfounded.
One variation worth adding is the use of an LMA as a preox/ de-nitorogenation adjunct. Basically you induce with whatever you consider appropriate, add paralytics if you think you need them working for you sooner than later, then slip in an LMA and use this rather than BVM for ventilation prior to intubation. This is helpful for those who have terrible mask fits, have terrible ventilatory mechanics,or degrees of instability that call for more immediate control of respiration. This is just another item for your bag of tricks, but speaks to the usefulness of supraglottic airways as tools to facilitate… Read more »
Any thoughts on nasal cannula flow rate for an infant or child?
write to Andy Sloas on his blog.
Scott, Great podcast and new study, man. At our flight program in California we implemented this protocol a year or so ago and a couple months ago had the opportunity to do it step by step on a traumatic head trauma patient. The small dose of Ketamine worked like a charm on a patient who was struggling so bad that they were drenched in perspiration.(as were the ground medics). We were able to settle the patient down, check his vitals, which were great then (got the SpO2 up to 100%) with NRM and then move the patient to the helicopter… Read more »
Awesome awesome awesome. I learned to use ketamine on sick hypotensive ICU patients for intubations about a year or so ago. It is usually my go to drug for almost all of my intubations. I have used variants of the DSI at times. I guess I was doing some of these things without knowing if others were doing it also. I didn’t do the hi flow o2 stuff but would sometimes use bipap or cpap to bridge them while I was setting up my intubations. I would push sedation and opioids but would sometimes get they way to sleepy to… Read more »
thanks Craig
more fuel to the fire for hfnc in this months ccm
Use of High-Flow Nasal Cannula Oxygen Therapy to Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate Hypoxemia.
do you find you need extra ketamine for intubation or is the initial 1-2mg/kg sedation dose sufficient with a muscle relaxant? Anyone had to use im ketamine in someone like this who was too agitated for safe iv access?
Big fan of the show. I’m Jason Syracuse, Critical Care RN at northern Arizona’s regional referral Level 1 Trauma center. I’ve been trying to get pre-oxygenation per you recommendations protocolized in my ICU but have been meeting resistance. I have two questions related to this: 1) A colleague expressed discomfort with slow playing a patient that “needs a tube now.” I attempted to explain that most of the time a patient does not need a “tube,” he needs oxygenation, ventilation, and PEEP. She stated she would feel more comfortable seeing it done before she tries it. Do you have a… Read more »
In the scenario described, won’t a small (0.5to 2mg) of midazolam have a similar effect? i.e. allow a decent pre oxygenation prior to a ‘RSI’. Maintenance of airway reflexes is not guaranteed with ketamine. When you use it you are still prepared for regurgitation +/- aspiration in someone with true full stomach. I suspect that true full stomachs are less common than we think!
Thank you for this great article! Just for clarification, your dosing recommendation of ketamine (1-2mg/kg) is for the racemic mixture?
yep
Do you top up the ketamine pre paralytic or rely on the initial 1-2mg/kg for the actual intubation?
Love the podcast, it’s always great information and care is taken to be objective. Please keep it going
I thought nasal cannula can provide UPTO 5LITRE OF OXYGEN
[…] or noninvasive ventilation, small boluses of ketamine can be used for sedation. (This is known as delayed sequence intubation). (Weingart […]
[…] Link to EMCRIT episode on DSI. […]
15 L/min via nasal prongs pops the connection tube off from the rotameter and could be uncomfortable for the patient, no?
no, even 50 lpm will not pop it off the flowmeter as established by the Caputo trial and another recent study which you can find at emcrit.org/preox demonstrates that 15lpm is perfectly tolerable to awake patients and I have done it myself for hours