 Background: Devil in the details
Background: Devil in the details

Airway management is a detail-oriented sport. Minor nuances of patient positioning can be essential. Or gentle laryngeal manipulation. Apneic oxygenation can improve first-pass success. Placing the pulse oximeter on the same arm as the blood pressure cuff can cause real headache. Failure to recognize and remove dentures is an enormous pitfall. An endotracheal tube placed too deep can cause hypoxemia and pneumothorax.
The difference between success and failure hinges on details. Optimizing each detail increases the likelihood of success. This post explores what might seem like a trivial detail: the ideal order of administration of rocuronium and ketamine for rapid sequence intubation (RSI).
The question: Rocketamine vs. Keturonium
Let's start with a common scenario. You need to perform RSI on a man with morbid obesity in hypoxemic respiratory failure. Even with perfect preoxygenation, you can't get his oxygen saturation above 96%. What is the best order of administration of medications?
- (a) Push rocuronium, then push ketamine.
- (b) Push ketamine, then push rocuronium.
Defining time intervals in RSI
 Safe Apnea Time
Safe Apnea Time
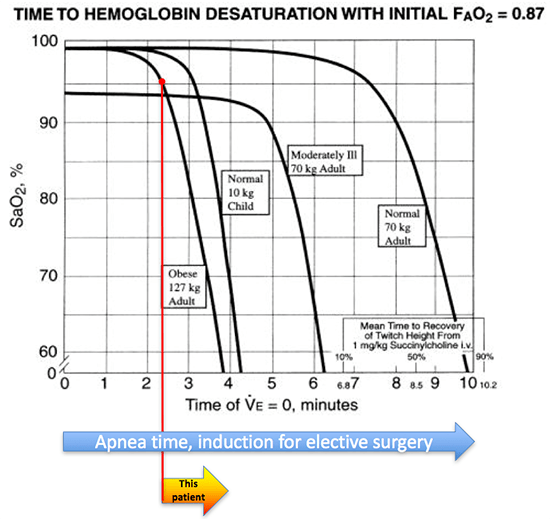
The safe apnea time is the amount of time that a patient will tolerate apnea,
before developing critical hypoxemia. For normal people undergoing elective anesthesia, this may be close to ten minutes (blue arrow above). For this patient, the apnea time is probably closer to 2 minutes (yellow arrow above). He is starting off with a saturation of 96%, near the steep portion of the desaturation curve. Given his morbid obesity, he is likely to de-recruit, shunt, and desaturate rapidly.
Sedation lag time
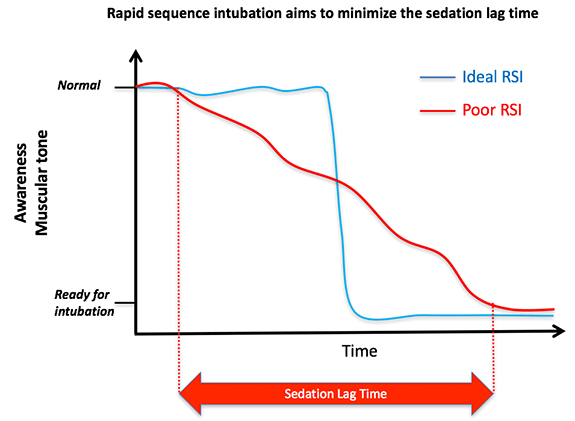
The sedation lag time is the interval in between onset of sedation and when the patient reaches complete paralysis. During the sedation lag time, bad things are happening: the patient's respiratory efforts drop, the lungs start to de-recruit, PaO2 starts falling, and PaCO2 is increasing. A prolonged sedation lag time will cut into the safe apnea time, reducing the time available to perform laryngoscopy.
The entire concept behind rapid sequence intubation is that the sedation lag time should be as short as possible. Ideally, the patient would go directly from breathing deeply (recruiting their lungs and clearing carbon dioxide) to a state of unconscious paralysis (blue curve below).
 Pharmacokinetics of rocuronium & ketamine
Pharmacokinetics of rocuronium & ketamine
Rocuronium
Using higher doses of rocuronium (e.g. ~1.2-1.4 mg/kg), paralysis typically occurs about 50-90 seconds after injection. Most patients will paralyze by 50-60 seconds, but shock may cause delays due to sluggish circulation of drug into the muscle.
Based on this onset time, it's generally wise to wait at least ~60 seconds after pushing rocuronium before starting laryngoscopy. Before 50-60 seconds, the patient is unlikely to be adequately paralyzed, leading to a risk of vomiting. This has been discussed previously (Pearl #9).
The pharmacokinetics of rocuronium may be roughly represented as follows:
 Ketamine
Ketamine

Ketamine has a fairly fast onset of action following a bolus. Most sources suggest an onset time of ~30-40 seconds following IV bolus (1). Notably, a large bolus of ketamine (e.g. 1.5-2 mg/kg) will often cause a short period of complete apnea and unconsciousness. The pharmacokinetics of ketamine may be represented as follows:
 Rocketamine vs. Keturonium
Rocketamine vs. Keturonium

 Now let's return to our initial question of how to sequence rocuronium and ketamine. It takes about 15 seconds to give the first drug and flush the IV before giving the second drug. This leads to two scenarios.
Now let's return to our initial question of how to sequence rocuronium and ketamine. It takes about 15 seconds to give the first drug and flush the IV before giving the second drug. This leads to two scenarios.
Rocketamine (Rocuronium then ketamine)
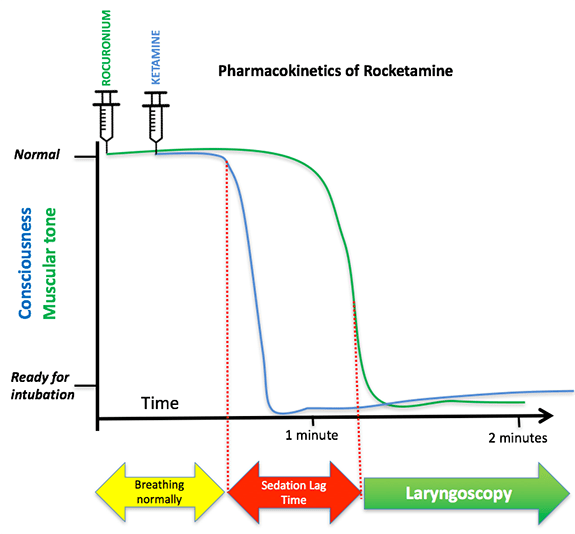 In this scenario, ketamine is pushed second, but it works faster so it still tends to kick in first. Meanwhile, rocuronium will start to take effect around 50-90 seconds. The net effect is that both drugs will take effect between ~45-90 seconds. This leads to a fairly short sedation lag time.
In this scenario, ketamine is pushed second, but it works faster so it still tends to kick in first. Meanwhile, rocuronium will start to take effect around 50-90 seconds. The net effect is that both drugs will take effect between ~45-90 seconds. This leads to a fairly short sedation lag time.
Keturonium (Ketamine then rocuronium)
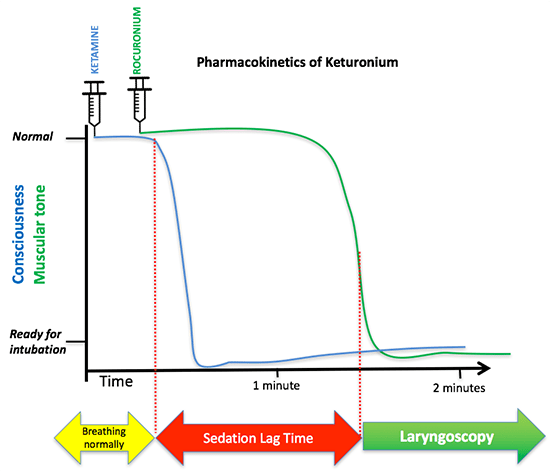 If ketamine is given first, the kinetics are as shown above. The ketamine bolus will typically cause apnea and unconsciousness in ~30 seconds. However, the rocuronium is pushed later and it takes longer to work, so paralysis won't occur until 65-105 seconds. This creates a sedation lag time of about one minute during which the patient is apneic (from the ketamine), but not paralyzed.
If ketamine is given first, the kinetics are as shown above. The ketamine bolus will typically cause apnea and unconsciousness in ~30 seconds. However, the rocuronium is pushed later and it takes longer to work, so paralysis won't occur until 65-105 seconds. This creates a sedation lag time of about one minute during which the patient is apneic (from the ketamine), but not paralyzed.
This prolonged sedation lag time is dangerous for two reasons:
- First, as discussed above, this promotes desaturation and thereby reduces the amount of time that laryngoscopy can be performed safely.
- Second, there is a risk of initiating laryngoscopy after the ketamine has caused apnea, but before the rocuronium has taken effect. This is a natural mistake to make, because the patient is apneic and may seem to be paralyzed. However, the patient isn't truly paralyzed at this point in time, so they may still vomit and aspirate.
Midazolam pre-treatment before RSI?
On a related note, imagine a patient who is a bit anxious prior to intubation. Perhaps they should receive a dose of midazolam as an anxiolytic, to reduce the emotional stress of the peri-intubation period?
This is fine for most patients, but not a great idea for patients with severe respiratory failure. A little anxiety prior to intubation is physiologically beneficial to the patient, as this will cause:
- Tachypnea (may reduce pre-intubation PaCO2, preventing respiratory acidosis later on during the apneic period).
- Deep breathing (causes recruitment of lung bases, improving oxygenation).
I've gotten into trouble a few times by trying to be a nice guy and give midazolam before intubation to patients with respiratory failure. In some patients, this will cause somnolence which exacerbates hypoxemia and decruitment, thereby increasing the risk of peri-intubation desaturation. Thus, my current practice is generally to avoid any premedication if possible (one notable exception being that if the patient is truly unmanageable then delayed sequence intubation is indicated). This is part of the paradigm of taking a patient from full arousal to anesthesia very quickly:
 Comparison to textbook approach & concerns about awareness
Comparison to textbook approach & concerns about awareness

Many standard textbooks recommend pushing the sedative prior to the paralytic. The principle guiding this sequence is that we would never want a patient to be paralyzed without sedation (anesthetic awareness). Hopefully this discussion has explained why pushing rocuronium immediately prior to ketamine won't cause anesthetic awareness.
Anesthetic awareness is a serious concern in the critical care arena. More realistic causes of awareness include:
- Not giving adequate sedation after intubation with rocuronium (the rocuronium out-lasts most sedatives provided during induction, so sedation must be re-dosed aggressively until paralysis wears off).
- Inadequate sedative doses in patients with a history of alcoholism and/or substance abuse (causing them to be refractory to standardized sedative dosing).
Additional strategies to prevent derecruitment during sedation/paralysis
Preoxygenation & apneic oxygenation
The cornerstones of achieving adequate safe laryngoscopy time are adequate preoxygenation and apneic oxygenation. Although critical, these have already been explored extensively here.
Intentional hyperventilation
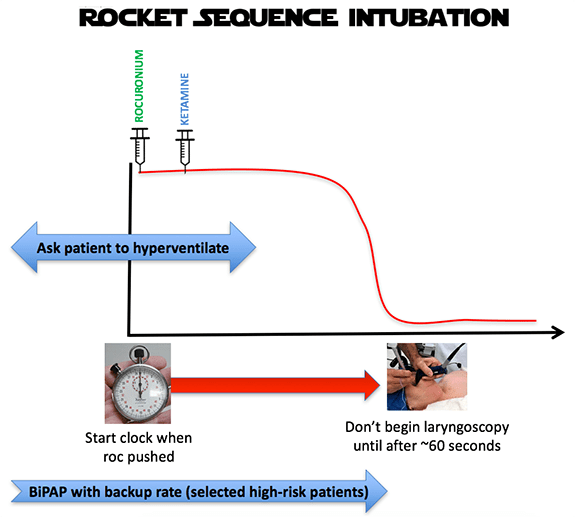
Patients who are awake may be encouraged to intentionally hyperventilate immediately preceding induction. The main effect of this is probably to drop the pre-induction PaCO2, thereby minimizing hypercapnia (3). It is possible that hyperventilation could improve recruitment and oxygenation as well.
Noninvasive ventilation during sedation/paralysis
Perhaps the most powerful strategy to reduce desaturation is noninvasive ventilation during sedation and paralysis. In short, this consists of attaching the patient to a BiPAP machine with a backup rate. As soon as the patient becomes apneic, the machine rate will immediately initiate gentle, controlled ventilation. Continuous administration of positive pressure avoids de-recruitment. Compared to manual ventilation, this has the advantage that it is seamless and provides perfectly-controlled breaths (unlike adrenergically-charged operators who tend to bag too hard).
Apneic ventilation using BiPAP generally works nicely, but it does depend on the ability to maintain a patent airway (e.g. gentle jaw thrust provided by the operator as the patient becomes sedated). There is no guarantee that it will work perfectly (2). Therefore, the best overall strategy may be to combine this with a rocuronium-ketamine sequence such that if the apneic ventilation fails, then the apneic time will still be limited.

Strategies to optimize laryngoscopy time may be summarized as follows:
- No benzodiazepine pre-treatment.
- Induction with high-dose rocuronium (e.g. 1.2-1.4 mg/kg) followed by ketamine.
- Adequate preoxygenation & apneic oxygenation.
- Voluntary hyperventilation before induction (if possible).
- In select high-risk patients, BiPAP with a backup rate may be used to provide positive pressure and gentle, controlled ventilation throughout this entire time period (VAPOX).
Related
- Fresh commentary on this post by Scott Weingart here and Pharmacy Joe here. Huge thanks to Scott, Joe, and many other experts who have offered opinions here and on those sites. This is a true demonstration of FOAM, wherein open-sourced collaboration and debate has taken this beyond something that I could have created alone.
- PREOX
- Weingart & Levitan, Preoxygenation & desaturation prevention, Ann Emerg Med 2012 (free).
- Supplemental information & preox updates (EMCrit)
- VAPOX (a.k.a., vent-as-bag strategy during induction)(4)
- Using pressure-limited ventilation (PulmCrit)
- Using volume-cycled ventilation (EMCrit)
- Grant S et al. VAPOX protocol & case series. Emerg Med Australasia 2016
Notes
- For example, Emergency Medicine Procedures by Reichman EF, 2nd edition, 2013, page 49.
- Note that even if the airway occludes, this strategy still works fairly well. Airway occlusion while on BiPAP will trap ~100% oxygen at positive pressure within the lungs. The positive pressure of the trapped oxygen will tend to keep the lungs open, preventing derecruitment. Unfortunately, airway occlusion will cause cessation of all ventilation, so PaCO2 will rise more rapidly than it would if the airway was open and there was ongoing ventilation. Thus, airway occlusion is potentially more problematic with regards to ventilation than oxygenation. In a situation where apneic ventilation was very important (e.g. severe metabolic acidosis), placing a nasal trumpet could be considered to improve ventilation during sedation and paralysis.
- Peri-intubation hypercapnia probably isn't a big issue for most patients (with some exceptions including patients with metabolic acidosis or elevated ICP). However, it is possible that peri-intubation hypercapnia causes peri-intubation hypertension in many patients (however, again, this generally isn't a big problem).
- Scott Weingart and I do VAPOX slightly differently. Either method will work fine. I would use whichever method you are more comfortable with (depends on which machines you use and how you generally set them up).

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
It may be worth considering why “RSI” in the first place? If we consider hypoxia / hypotension as the biggest predictors of airway-related death, why not prioritize avoiding them instead of prioritizing avoidance of passive regurgitation / aspiration (an infrequent event with limited morbidity) as advocated in the “RSI” approach? This may involve EARLY administration of ketamine to allow optimal pre-oxygenation with positive airway pressure / PEEP, continuation of oxygenation during the apneic period with positive airway pressure / PEEP, and provision of nasal cannula oxygen during laryngoscopy. All outside-of-OR intubations occur in sick patients, many (most?) of whom have… Read more »
When to use RSI is a great question, for example should we be using awake intubation for severely hypoxemic patients? This is an important question but a bit outside the scope of this post.
What does de-recruit mean? Never heard that term before.
De-recruitment is basically the development of atelectasis that occurs following apnea, which causes desaturation. For more on this see Scott Weingart’s post on preoxygenation, there are some neat videos of lungs there that explain this concept beautifully: https://emcrit.org/preoxygenation/
Very insightful post Josh.
I’ve thought about this concept of sedation lag. While it can be problematic with other sedatives, I think Ketamine is the perfect drug for this problem. My solution in a patient in whom those extra seconds can make a difference has been to simply push Ketamine slow, then slam in the paralytic. Ketamine should rarely cause apnea with slow push (we do this all the time for procedural sedation). So, slow Ketamine push to dissociation (unaltered spontaneous respiration), then fast paralytic push. No unnecessary, compounded apnea time.
Sam
Excellent point Sam. Agree that if ketamine is given before rocuronium it should ideally be given slowly to avoid apnea. I’ve done this several times, generally within a delayed-sequence intubation (DSI)-type strategy with success.
My only reservation about ketamine-first is for patients with severe hypoxemia who are struggling to breathe, sedation may cause them to relax and struggle less, leading to desaturation. Ketamine when given slowly doesn’t cause apnea, but these folks will often have reduced breathing effort after sedation which can work against you.
This is one of the reasons why I prefer the faster acting succinylcholine.
Succi is imho totally contra indicated in the critical patient. Hd roc is almost as fast acting.
can you please justify this broad, sweeping and totally wrong statement? I think the FOAMed community has done a great disservice by its scorn of succinylcholine, which does act faster and has very rare true contraindications.
Jordan, I’m with you on this one. Admittedly, I’ve probably only administered Ketamine less than 100 times. But apnea? Really? Maybe I’ve never pushed it fast enough. . . And I can’t count the number of times I’ve pushed Sux (hundreds) and have NEVER experienced clinically relevant hyperkalemia. So to Stephan who says it is “totally contra-indicated in the critically patient” – well, wow I must have really harmed a lot of patients. And despite being the ED QA director for 6 years and the ED medical director for another 2+ years, my ICU colleagues have never informed me about… Read more »
The onset time for high-dose rocuronium (1.2-1.4 mg/kg) is equivalent to succinylcholine, eg: http://europepmc.org/abstract/med/7902034, http://europepmc.org/abstract/med/7978469
Those papers show that high dose rocuronium has a “similar” onset time although if you look at the raw numbers sux is still quite a bit faster (34 versus 54 sec at the laryngeal adductors, 56 versus 65 sec at the adductor pollicis). The Cochrane review also found in general that succinylcholine is faster although high dose roc is pretty close. I’ve never seen a paper finding that roc is as fast. And the contraindications for sux are quite rarely encountered. They do include things like neuromuscular disease, hyperkalemia (though not renal dysfunction) and history of MH. Critical illness is… Read more »
Hyperkalemia is absolutely not rare, for muscular disease/ mh you are more or less right. And in pulmonary crit care we’ll see a fair share of patients with muscular diseases in respiratory distress. But since you usually don’t know the history of a new critically patient wheeled in into your Unit, I think it is best to opt for security. Anyway ICUs at our hospital and the paramedical services decided long ago to get rid of succi. It is even rarely it almost not at all used in our anaesthesiological department. But I think every Doc needs to find strategies… Read more »
I completely agree. Sux has gotten a bad rap for no good reason at all.
Great article, The idea of giving a muscle relaxant after an induction agent has more relevance in the elective anaesthesia setting and is a traditional approach. This comes from the school of thought that one should be able to bvm prior to the relaxant is injected and not fall into a can’t intubate can’t ventilate/ can’t oxygenate. However, not everyone uses this approach and some advocate early injection of relaxant to ensure peak effect and maximising intubating conditions. So its easy to see why the muscle relaxant first” behaviour has made its way across to scenarios where critical care type… Read more »
An induction dose of ketamine (e..g. 1.5 mg/kg) should cause dissociation and loss of any awareness. The only exception I’ve run across were a few patients with alcoholism who seem resistant to ketamine (no data on this, just my own observations for whatever that’s worth).
Thanks for your reply Josh. In certain acute scenarios awareness is low in the priorities and old approaches such as “suxamethonium and an apology”
https://www.google.co.uk/amp/s/lifeinthefastlane.com/ccc/rapid-sequence-induction-of-the-shock-patient/amp/
Regarding your point about alcoholism ( or anyone with an increase MAC), there may be an opportunity to add in adjuvant induction agents to smooth it out?
PS I used Ket then ROC just the night prior to my initial post on a 50 y/o patient with life threatening asthma. It worked very well.
Thanks for your blog!
I have done roc then ketamine a few times over the last couple of years. I know there are averages, but I feel like the onset of these meds are unpredictable. Most recently I did this on a 40 y/o hemodynamically stable patient with ARDS with SpO2 92% on 100% BiPAP (tolerating it fine). Essentially the roc (1.5 mg/kg) was pushed with ketamine (2 mg/kg) right behind then a flush. It was very obvious to all who were threre that the roc took effect before the ketamine. It did lead to the fastest intubating conditions possible and I’m glad she… Read more »
Nice job, sounds like you saved this woman’s life. Did she have any recall? I’d bet that she didn’t. I’ve been doing roc-ketamine for years. Some patients aren’t 100% dissociated before paralysis, but they are close enough to dissociation that they don’t remember anything and are probably well analgesed (ketamine is a good analgesic). Also note that if you start laryngoscopy at 50-60 seconds, it’s probably 60-75 seconds before you’re causing any real stimulation. I’ve yet to have a patient report awareness of intubation due to this sequence. I don’t use sux, but the evidence seems to suggest that onset… Read more »
Thanks for the great blog and for the reply: Not sure if she has recall (or…..whatever it does to the subconscious). It wasn’t pleasant for any of us to watch. I always tell people to think the happiest thoughts they can right before they dissociate with ketamine, because I’m convinced (with no evidence) that it makes the “trip” more pleasant. I am not sure being paralyzed while awake right before makes the trip pleasant. Regardless, I have pushed drugs in this sequence quite a few times, and that’s a relatively rare event. A few of points below that I couldn’t… Read more »
we usaually start with low dose of paralytic (15-25% of the dose), then we give the sedative followed by rest of paralytic. i think this works well.
Yes, that is called “Priming” and is use to get a faster onset of Rocuronium…
Very interesting concept. Looks like we should give it a try. We usually use high dose sufentanil ( sometines plus midazolam/ etomidate)/ roc for true rsi or in hypotensive patients hd s-ketamine and roc( both 2mg/kg patient) in a modified dsi. But we usually opt for giving ketamine first after conventional preoxygenation via mask or hfc. In my experience patients on ketamine are immobilized but don’t stop breathing. Then we iniate bilevel niv to achieve the highest possible saturation, after that we give the roc (2mg/ kg), which works a bit faster than your proposal. Then we intubate. This concept… Read more »
I’m surprised you still use etomidate; your patients sound like they could well be at risk from etomidate-induced adrenal suppression (http://www.medscape.com/viewarticle/773598). Also, bag mask ventilation will provide much better pre-oxygenation. I’m not sure I would consider NP or NRB/HM pre-oxygenation “conventional”.
I am all for giving the muscle relaxant before the induction agent where necessary, but in my experience roc can be extremely painful on injection, even in semi-anaesthetised patients. Do you do anything to mitigate this? (eg lignocaine pretreatment?)
BW
Matt
We sometimes administer 10-20mg lidocain in to the line before giving propofol, because a lot of patients say injecting it hurts. ( OR) Might work for roc, too.
That dose is more or less harmless and delivers good veinous anesthesia in my experience.
Though in the ICU, we don’t do this ( dont know why)
Josh, Thanks for tackling this topic. Though we perform RSI on almost a daily basis, we rarely discuss the order of the medications (at least out loud). The post provided a detailed pharmacokinetic/pharmacodynamic case for administering ketamine before rocuronium to achieve optimal intubating conditions more quickly, while minimizing “sedation lag time.” We’d like to offer a few counter points to consider. 1) IV access is sometimes challenging. In a combative trauma patient, a patient with extensive history of IV drug abuse, or an ESRD patient on dialysis, lines frequently blow or are only good for drawing blood (not administering medications).… Read more »
These are all great points. I think it’s important to emphasize that drug onset is unpredictable (note there is a STANDARD DEVIATION in the onset times) and you have to make a risk/benefit decision each time. I am not sure we should standardize roc before sedative (maybe only in those who really can’t afford the extra few seconds…and I admit that some can’t). As I noted above, even if you push both as fast as possible, the onset of roc first can lead to an ugly scene that I think should be reserved for those who can’t tolerate 20 seconds… Read more »
Bryan and Nadia, Thanks for some brilliant points. I’m afraid that I might have just opened up a Pandora’s box of debate (similar to roc v. sux or crystalloid v. colloid) which will now continue eternally. 1. Access: Many patients are very unstable in the post-intubation period (often requiring vasopressors). Thus, bad things may happen if you go into an intubation with poor IV access and lose access midstream. This is true regardless of your induction drug sequence. 2. I would imagine that in a patient with poor perfusion, onset of *both* rocuronium and ketamine would be delayed, but the… Read more »
Ketamine and rocuronium have not been tested for compatibility in the same syringe. Generally, we avoid it if we don’t know. ISMP recommends against mixing more than one med in the same syringe for IV push, except by the pharmacy (http://www.ismp.org/Tools/guidelines/ivsummitpush/ivpushmedguidelines.pdf). The situation it most commonly arises for is ketofol. Based on kinetics, and ISMPs recs, I advocate for separate syringes for these two meds as well (https://www.ncbi.nlm.nih.gov/pubmed/23331657).
Hej!
Thanks for the Post! I got one comment concerning Roc: In my experience a Push Dose of Roc is VERY painful for the Patient, This should be concerned. Maybe we are using a different preperation of Rocuronium in Europe?! Even a consutant told me that she experienced sore pain during injection (too fast inj. after Induction) when she was anaesthetised.
Second thing: You wrote about Rocuronium “Most patients will paralyze by 50-60 seconds, but shock may cause delays due to sluggish circulation of drug into the brain.” Should be …into the muscle..?!
Thanks!
Michael
(resident physician anaesthesia, Austria)
Thanks, I fixed the brain/muscle error.
Must admit that I wasn’t aware of rocuronium-induced pain. However, regardless of the order of rocuronium vs. ketamine, the patient will still be conscious while receiving rocuronium (so this won’t resolve the rocuronium-induced pain issue).
My thoughts on all of this are in this EMCrit Wee: https://emcrit.org/timingprinciple
You say: “Most patients will paralyze by 50-60 seconds, but shock may cause delays due to sluggish circulation of drug into the brain.”
It doesn’t change anything about the lag, but paralysis is a peripheral phenomenon, so you might want to correct this sentence about the brain…
Thanks, I fixed it.
Great post, thanks for this Josh. The comment about standard deviation got me thinking & I ran a 5000 patient Monte Carlo simulation using the onset & standard deviation of roc from one of the studies that often is quoted as proving roc is about as fast as sux, and the onset & standard deviation from a study with ketamine. I’ll make a full post about it Monday but here are the top line results: Average sedation lag time when ketamine is given first: 49 seconds (just like you said in the post, about 1 minute) Average sedation lag time… Read more »
It’s not valid to analyze this using a Monte Carlo simulation. This simulation assumes that the onset time of roc and ketamine are independent, whereas in reality the opposite is true. Patients with lower volume of distribution and good perfusion will have fast onset.time of roc and ketamine. Patients with sluggish perfusion will have slower onset of both drugs. Pharmacokinetic parameters will tend to affect the onset time of both drugs in the same way. Thus, it is biologically implausible, for example, that a single patient would have unusually *fast* onset of rocuronium but unusually *slow* onset of ketmamine. As… Read more »
I think the only analysis that could earn the label “valid” is one where the onset for both drugs is determined in the same critically ill patient population. Perfusion time is not the only thing that affects drug distribution. Partition attributes between the plasma and tissue, pH, protein binding, lipid solubility, receptor affinity also play a role…perhaps even larger than perfusion time. If that wasn’t the case then rocuronium 0.6 mg/kg and 1.2 mg/kg should have the same onset. Since the studies the onset data was collected in used healthy surgical patients, and we are assuming that poor perfusion time… Read more »
Thanks Joe, nice work. Now that your post is up I’ve linked to it above, but here is another link as well: https://www.pharmacyjoe.com/the-risk-of-anesthetic-awareness-when-giving-rocuronium-before-ketamine-rocketamine-in-rapid-sequence-intubation/
This is a tricky topic. I’m still not sure that there is a single right/wrong answer to it (like most things in medicine, it probably depends on the clinical scenario). However, the robust debate on EMCrit and your site have certainly helped explore all possible angles on the problem.
Thank you Josh, I agree on all points – highly dependent on the clinical scenario and FOAM is a great thing! If only we had FOAS (Free Open Access Spectrophotometry) as well for the syringe issue!
I am a bedside nurse in an ICU where it seems to be common practice to “keep paralytics on standby” (Rocuronium) if intubating with general anesthetics/sedatives is insufficient. Often times I will see providers make their first attempt at DL after pushing Ketamine, Etomidate, propofol or simply midazolam with fentanyl and fail. They then want the paralytic pushed for the second attempt which usually is made within 30 seconds of pushing the roc… seems pretty pointless. I will be sharing this article with some of my coworkers!
If Versed (which I don’t use) relieves anxiety proportionately more than it depresses respiration (and I wager that it does), its net effect may be to *improve* CO2 prior to intubation via reduced CO2 production. I can hardly say what the net effect on CO2 total body stores will be, but it’s an open question, I think.
What does it mean to de-recruit?
I like to use this approach in a standard patient RSI, to reduce the sedation lag time, but I find trying to get others comfortable to try it difficult, any ideas on teaching this aside from showing literature?
Josh how often do you use the rocketamine approach? Has there been any studies that show there is a risk of anesthetic awareness?
Due to the short onset of action, could we apply the same principle of using rocuronium first when using propofol as sedative agent for RSI?
For what its worth, I had a good minute of paralytic awareness when i was intubated under the Rocketamine RSI. (It was explained later that thus mustve been why, due to obese sleep apneac they pushed the roc 1st ). I dont know why the roc worked so well before the ketamine even hit, maybe they underdosed the K or pushed it too slow. Total psychic terror for at least 60 sec which is a long time. I tried moving toe, muscle groups, “threw” myself from inside, tried blinking morse etc. I thought something had gone horribly wrong and theyd… Read more »