 the question
the question
Some patients with HSV encephalitis may initially have a negative CSF PCR for HSV, with a repeat being positive some days later. This has led to confusion regarding who, exactly, needs a repeat lumbar puncture?
Montmollin E et al: HSV encephalitis with initial negative PCR: Prevalence, associated factors, and clinical impact.
This is a fresh retrospective analysis of a multicenter database including all patients with HSV encephalitis who were admitted to 47 ICUs in France between 2007-2017. It represents the best available data on this topic.
Of 273 patients with HSV encephalitis, 11 patients (4%) initially had negative PCR results. So this is a real phenomena, albeit uncommon. Additionally, case descriptions of these patients indicate that they were sick (e.g., often with seizures, encephalopathy, or coma). So, we can begin by concluding that PCR-negative HSV encephalitis is a clinically significant thing in ICU.

All 11 patients who were initially PCR negative had lumbar punctures performed within 3 days of symptom onset (figure below, left panel). This is happily consistent with prior, smaller case series.(Weil et al. 2002) So false-negative PCR results appear to be restricted to patients early in their disease course.

A supplemental data table describes the 11 patients who were initially PCR-negative. All 6/6 patients who had an MRI within a day of admission had abnormalities in the temporal or frontal lobes consistent with HSV encephalitis (although not all were deemed “typical” for HSV). Although this is a small sample size, it is consistent with the excellent sensitivity of modern MRI scanners for HSV encephalitis (particularly among a population of critically ill patients who have substantial brain dysfunction – which should be mirrored by substantial radiological abnormalities). Thus, it seems that a negative HSV PCR plus a normal MRI could generally exclude HSV as the cause of a patient's encephalopathy.
Many of the 11 initially PCR-negative patients also underwent EEG, with four being found to have temporal lateralized periodic discharges (LPDs, the EEG abnormality formally known as “PLEDs” a.k.a. Periodic Lateralized Epileptiform Discharges). Temporal LPDs are characteristic of HSV encephalitis, albeit nonspecific. No patient with a normal MRI had LPDs – so it's unclear whether LPDs add independent information beyond what is provided by the MRI.
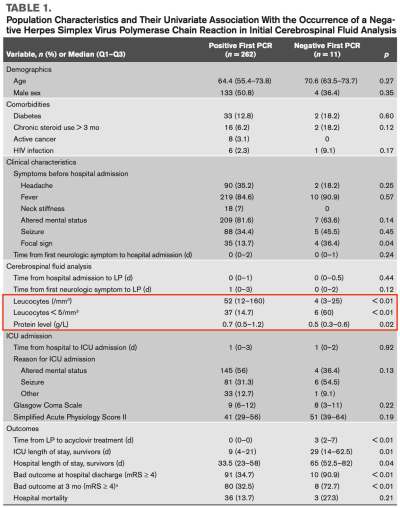
Patients who were PCR-negative tended to have less marked abnormalities of their CSF chemistries (table above; red box). Three of these patients who were initially PCR-negative also had stone-cold normal CSF chemistries (e.g., <5 cells/mm3 and normal protein levels). This is a reminder that it is possible for CSF chemistries to be completely normal in HSV. Within the entire population of 273 patients with HSV encephalitis, 17% had a normal CSF leukocyte count (<5 cells/mm3). The use of CSF chemistries to risk-stratify for HSV encephalitis was explored previously in the blog here.
so where does this leave us?

This leads to the general schema above. Of course, this is just a general schema which should not be followed by rote. For example, if an investigation reveals an alternative cause for the patient's presentation, then it's unnecessary to rigorously exclude HSV. The true goal isn't to rule out HSV, but rather to figure out what disorder the patient actually does have! Becoming fixated on ruling out a single disorder usually isn't a successful diagnostic strategy.
This approach is consistent with recent French guidelines, with the exception that these guidelines don't incorporate MRI data.(Stahl et al. 2017) Ultimately, whether to repeat a lumbar puncture in a patient with a normal MRI and a negative HSV PCR is a clinical decision depending on the totality of available evidence, as well as other factors (e.g., presence of anticoagulation and risk involved in performing the lumbar puncture).
An evolving theme in neurocritical care is taking a systematic approach to combining multimodal diagnostic information. Thus, rather than approach a patient with suspected encephalitis solely by performing a lumbar puncture and then waiting for the results – a more fruitful strategy may be to simultaneously pursue an MRI as well as a lumbar puncture, and possibly an EEG as well (if there is a concern for nonconvulsive status epilepticus). Front-loading numerous modalities may facilitate a more rapid and robust diagnostic approach.
It's worth noting that this approach is intended for critically ill patients who have a moderate pre-test probability of having HSV encephalitis. Alternatively, if someone presents to the emergency department with a headache and fever (but no evidence of parenchymal brain dysfunction), this algorithm would not apply.

- HSV PCR had a 96% sensitivity in this large series of critically ill patients with HSV encephalitis. All false-negatives occurred in patients who had been symptomatic for three days or less.
- The combination of a negative HSV PCR as well as a high-quality MRI with no evidence of HSV encephalitis is likely sufficient to exclude HSV as the cause for a critically ill patient's altered mental status.
- The following general approach may be reasonable (with additional tailoring to individual patient specifics).

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
A Pt could be Negative for HSV Encephalitis but other infections should be considered. West Nile Virus & Valley Fever are 2 Examples we see in Southern California. Los Angeles Hospitals will test for these if there is a decrease in LOC, H/As, etc…. There was a Pt airlifted from Kenya back home to Los Angeles after testing positive for WNV (West Nile Virus) & admitted to a Teaching Hospital in LA. Unbeknownst to her, she had been bitten by an infectious Mosquito before boarding her plane in LA for Kenya, as she was symptomatic on arrival in Kenya. The… Read more »
Excellent Josh as always.. and thank you Anne for your comment…