
Introduction with a case
A 40YO woman was admitted to the ICU for status epilepticus. Her past medical history was notable for a Chiari malformation managed with prior VP shunt placement. More recently she had sustained moderate head trauma while inebriated (with negative head CT). She presented to the emergency department with sustained generalized tonic/clonic seizure refractory to benzodiazepine and requiring intubation. As part of her evaluation she underwent lumbar puncture with the following result:
- CSF was clear with a normal opening pressure (11 cm)
- Glucose: 66 mg/dL
- Total protein: 116 mg/dL (normal <50)
- Nucleated cells: 1 (normal <6)
- Red blood cells: 134
Does this patient require empiric acyclovir while awaiting the results of HSV PCR? Acyclovir was initially started in the emergency department. The nocturnal intensivist felt that HSV was unlikely and discontinued acyclovir. The following day, acyclovir was re-started when the patient spiked a low-grade fever. Ultimately, the HSV PCR returned as negative and acyclovir was stopped.
Empiric acyclovir: to cover or not to cover?
HSV encephalitis can occur without dramatic CSF findings. Thus, HSV is often covered empirically while awaiting the results of HSV PCR. However, empiric acyclovir causes problems:
- Acyclovir may lower the seizure threshold, which is counterproductive in a patient who is being admitted with neurologic injury (especially status epilepticus).
- Acyclovir is nephrotoxic. These patients often receive vancomycin, which may synergize with acyclovir to promote kidney injury.
There is significant practice variation regarding whether to give empiric acyclovir while awaiting PCR results. The goal of this post is to search for an evidence-based approach to this issue.
Brief Literature Review
Articles have focused on developing decision rules to determine which CSF samples require testing for HSV PCR. However, these decision rules can also be applied to determine which patients require empiric acyclovir.
Tang et al. 1999
This was a large study from the Mayo Clinic which attempted to correlate CSF chemistries with the detection of various viruses, including HSV. Between 1995-1997, 716 CSF samples were tested for HSV, of which 13 (1.8%) were positive. Nearly all of these samples had elevations of both protein and leukocyte count (11/13). Two positive specimens had elevated protein and normal leukocyte count (0-5 WBC), suggesting that a normal leukocyte count cannot exclude HSV.
Simko et al. 2002
This was a large study from three Harvard-affiliated hospitals which correlated CSF chemistries with HSV PCR. Between 1996-2001, 2759 CSF samples were tested for HSV. 55 tested positive, including 16 patients with clinical HSV encephalitis. All HSV-positive patients had an elevated CSF leukocyte count (>5 cells/mm3), elevated protein (>50 mg/dL), or both. One patient with HSV encephalitis had a leukocyte count of 2 cells/mm3, and three patients had a leukocyte count below 10 cells/mm3. Similar to the Tang's study above, this shows that a normal leukocyte count doesn’t exclude HSV.
Reller et al 2007
Reller Criteria requires one or more of the following:
- Elevated CSF cell count (>5 nucleated cells)
- Elevated CSF protein (>50 mg/dL protein)
- Immunocompromise (HIV or organ transplant)
- Age <2 years old
This was a prospective study at Duke performed to validate a decision tool used to determine which CSF samples were appropriate for HSV testing. Between 1999-2004, only CSF samples meeting the above criteria were tested for HSV. Rejected specimens were frozen and tested later on, to validate these criteria.
A total of 1,659 CSF specimens were submitted over this time period. Of these, 347 were rejected for HSV PCR because they didn’t meet the above criteria. 222 of these rejected specimens were frozen for subsequent analysis. Zero of these 222 specimens were positive for HSV-1. Two specimens tested positive for HSV-2, but upon further investigation these specimens came from patients with HIV (which hadn’t initially been communicated with the laboratory).
Bouza et al. 2013
Bouza Criteria requires one or more of the following:
- CSF WBC count >10 nucleated cells
- Immunocompromise (HIV or organ transplant)
- Age <2 years old
This is a single-center study with a similar design compared to Reller 2007. Between 2008-2011, only CSF samples meeting the above criteria were tested for HSV. Samples which were rejected were frozen and stockpiled for subsequent analysis.
Bouza Criteria is more narrow than Reller Criteria, raising concerns that Bouza Criteria could reject CSF samples which are positive for HSV. To address this, the study focused on CSF samples which met Reller Criteria but not Bouza Criteria.
During the study period, 466 CSF specimens were submitted for analysis. Seventy were identified which had been rejected on the basis of the Bouza Criteria, but would have been accepted for testing using Reller Criteria. These were tested for HSV PCR, and none of the samples was positive.
This study suggests that Bouza Criteria has equal sensitivity for the detection of HSV compared to Reller Criteria, but greater specificity. However, only seventy specimens were analyzed wherein the two criteria disagreed. The 95% confidence interval of the proportion 0/70 is equal to 0-5.2%, indicating that a clinically meaningful difference might have been missed.
Wilen et al. 2015
These authors at the Barnes-Jewish Hospital in St Louis set out to determine a set of criteria that would exclude viral infection based on CSF chemistries (including HSV 1&2, VZV, CMV, and enterovirus). They used retrospective data from patients between 2008-2012 to test various criteria, and then applied these criteria to data from 2013.
Six different criteria were applied to data from 2008-2012. For each type of virus, patients who were PCR-positive were compared to twice as many PCR-negative patients who were selected at random from among hundreds of PCR-negative patients. As shown below, the Reller Criteria and the Bouza Criteria had equal sensitivity for detecting patients who were HSV-positive. However, the Bouza Criteria had higher specificity.
 When applied to the 2008-2012 data, both the Reller Criteria and the Bouza Criteria would have resulted in cancellation of three PCR tests which were positive for HSV. Of these three tests, only one was judged to represent a clinically significant infection.
When applied to the 2008-2012 data, both the Reller Criteria and the Bouza Criteria would have resulted in cancellation of three PCR tests which were positive for HSV. Of these three tests, only one was judged to represent a clinically significant infection.
The Bouza Criteria were subsequently tested on data from 2013. Within this time frame, all seven patients with clinically significant HSV infection would have been detected. Two patients failing to meet these criteria were found to be HSV-PCR positive, but infectious disease consultants didn't believe that they had a clinical HSV infection.
Rawal 2015
This was a case report of a 60-year-old man with HSV encephalitis and normal CSF analysis (WBC count of zero, protein level of 18 mg/dL). The diagnosis was made based upon a positive PCR result and temporal lobe enhancement on MRI. No known cause of immunocompromise was present.
This case illustrates that HSV infection can occur with normal CSF analysis. Two similar cases have been previously reported in the Turkish language literature (Oguz 2006). However, case reports are subject to publication bias, wherein bizarre cases are preferentially published.
Hebant et al 2015
This was a report of two cases of HSV encephalitis among elderly patients (age 80-90) who had normal CSF WBC count. One patient had a history of myeloproliferative disorder and prostate cancer status post radiation therapy, whereas the other patient had no known immunocompromise. These patients did have elevated CSF protein levels, so they met Reller Criteria (but not Bouza Criteria).
Saraya et al. 2016
This is a single-center retrospective chart review study aimed at characterizing the occurrence of normocellular HSV encephalitis. Between 2002-2011, 23 patients with encephalitis and positive HSV-PCR were identified. Among these patients, 6/23 (26%) had 0-5 WBCs in their CSF. One of these patients was immunosupressed with HIV, but some had no identified cause of immunosuppression:
 This study does have some limitations:
This study does have some limitations:
- Performed at single center in Thailand
- Unclear whether immunocompromise was excluded in all patients.
- Unclear that all of these cases represented true clinical HSV infection.
Nonetheless, this study does suggest that some patients may have HSV encephalitis with normal WBC count. Two thirds of these patients had elevated protein levels. Such patients with normocellular CSF and elevated protein would be detected by the Reller Criteria, but not the Bouza Criteria.
Hauser et al. 2017
These authors tested the Reller Criteria using a retrospective study of the entire database of the Veterans Association Hospitals between 2000-2013 (including 85 hospitals). Over this time period, 101 patients were detected with a positive CSF PCR for HSV. Among these patients, only seven (7%) had normal protein, normal WBC, and no immunocompromise. However, chart review demonstrated that these seven patients weren't believed to have true HSV infection. Thus, it appears that Reller Criteria was 100% sensitive for detecting clinical HSV encephalitis.
Evidence Summary
Bouza criteria vs. Reller criteria
 Combining data from these studies yields the above estimates of the sensitivity for detecting HSV infection (1). Although no study directly showed the Reller Criteria to be more sensitive than the Bouza criteria, there is a greater volume of data regarding the Reller criteria which creates a tighter confidence interval. Case studies have identified some patients with HSV infection who have a normal WBC count and elevated protein, suggesting that the Reller Criteria probably does have a somewhat higher sensitivity than the Bouza Criteria.
Combining data from these studies yields the above estimates of the sensitivity for detecting HSV infection (1). Although no study directly showed the Reller Criteria to be more sensitive than the Bouza criteria, there is a greater volume of data regarding the Reller criteria which creates a tighter confidence interval. Case studies have identified some patients with HSV infection who have a normal WBC count and elevated protein, suggesting that the Reller Criteria probably does have a somewhat higher sensitivity than the Bouza Criteria.
Numbers in clinical context
Among all patients with CSF sampled, only ~1.5% are positive for HSV. Therefore, the average likelihood of missing a case of HSV using these criteria is as follows:
- Bouza Criteria: (1.5%)(1.4%) = 0.02% = 1/4,800
- Reller Criteria: (1.5%)(0.4%) = 0.006% = 1/17,000
Of course, these numbers will vary depending on the pre-test probability. For example, consider a patient with seizures and temporal lobe enhancement on MRI, who would have a much higher pre-test probability of disease (perhaps ~80%). For this high-risk patient, the likelihood of missing a case of HSV would be as follows:
- Bouza Criteria: (80%)(1.4%) = 1.1% = 1/90
- Reller Criteria: (80%)(0.4%) = 0.3% = 1/300
Limitations of the evidence
- Studies are underpowered to determine the precise sensitivity of various sets of criteria. Sensitivity is based upon the number of true-positives (patients with HSV). Since this is a rare disorder, this analysis is underpowered despite including thousands of patients overall.
- Studies generally consider “HSV+” patients as a single group, despite the fact that they represent a heterogeneous mixture of HSV encephalitis and HSV meningitis. Among critically ill patients, we're primarily worried about HSV encephalitis. Unfortunately, these two disorders are associated with different CSF patterns: abnormalities are generally more dramatic in HSV meningitis. Therefore, studies which combine both entities will tend to report more dramatic CSF abnormalities than would be expected for a pure population of HSV encephalitis.
- Studies often went back and chart-reviewed data only from patients with discordant test results (e.g. positive HSV with normal CSF chemistries). This sort of selective data verification may tend to increase the performance of the decision rules.
Proposed algorithm
The literature evaluates these criteria as tools to avoid ever checking a HSV PCR. However, a decision never to test for HSV requires that all stakeholders agree on it as a hospital-wide policy. Without such agreement, someone will invariably want the HSV PCR… so you may as well just order it up-front.
These criteria are nevertheless useful as an evidence-based framework for determining which patients require empiric acyclovir (while awaiting the results of HSV PCR). The algorithm below shows how pre-test probability could be combined with various criteria to determine which patients require empiric acyclovir:
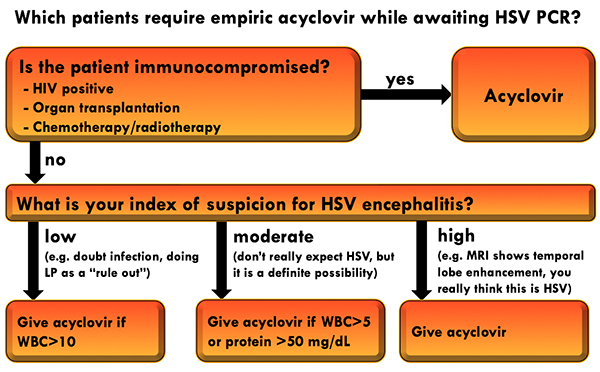 This algorithm isn't perfect, but at least it provides an evidence-based framework to approach this decision. It is based on the following considerations:
This algorithm isn't perfect, but at least it provides an evidence-based framework to approach this decision. It is based on the following considerations:
- A patient with average risk for HSV infection (~1.5% pre-test probability) and negative Reller Criteria has a risk of HSV infection of ~1/17,000. A patient with a low pre-test probability of HSV (~0.5%) and a negative Bouza Criteria has a risk of HSV infection of ~1/14,000. The risk of acyclovir-induced nephrotoxicity from a short course of treatment isn't exactly clear, but probably much higher (e.g. ~1/20; Yildiz 2013). Therefore, the risk/benefit ratio doesn't favor the use of acyclovir in these cases.
- HSV-PCR is generally available within a day, so failure to provide empiric treatment would delay therapy by less than a day. HSV encephalitis is generally a more indolent process than bacterial meningitis, so one day's delay in therapy probably wouldn’t be catastrophic.

- Acyclovir is nephrotoxic and lowers the seizure threshold. Therefore, universal application of empiric acyclovir to all encephalopathic patients while awaiting an HSV PCR would cause harm.
- Various decision tools are available in the literature to exclude HSV infection on the basis of CSF chemistries and immunologic status. Although this remains controversial, these tools have been validated and may provide a framework for determining which patients require empiric acyclovir.
- An algorithm incorporating pre-test probability and published decision tools is proposed:

Notes
- Statistics performed online using http://vassarstats.net/prop1.html.
Image credits: Opening image from Eulante-Bermendi SA et al. Neurologia 2015; 30 (7) 455-457.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Wow man, great review. will be using this in daily practice. Thank you.
thanks much. This was a pretty dry topic to research, but it’s been driving me crazy for a while. I always feel like I’m either under-treating or over-treating.
Absolutely clinically relevant and I face this issue more frequently than I wish. Thanks for the comprehensive review.
hello Josh bet the mountains are lovely up your way now… very cool review. so you are saying that even 24 hours of IV acyclovir (do you use 10 or 20/kg/dose) while waiting for the PCR HSV may be detrimental/nephrotoxic. whats a bit worrisome/curious is the Hauser VA study 2017. you saying that 101 patients were tested positive PCR HSV , but 7 patients were determined not to be true HSV infection. i (mistakenly?) thought that PCR was the “gold standard” for determining try infection. false positive PCR’s in 7%? am i misunderstanding? thank you so much for this thorough… Read more »
Yeah, it’s pretty up here in Vermont. Generally use 10 mg/kg IV q8hr. I have seen acute kidney injury occur in the context of short courses of acyclovir and vancomycin. Unfortunately its impossible to know for sure whether this is due to acyclovir or other elements of critical illness. HSV PCR has excellent performance, but its not perfect (specificity <100%). When applied to a population with a very low pre-test probability, this will lead to some false-positives. Even a very good test if used in a population with a very low disease incidence will yield false-positives - in essence using… Read more »
Great review, Josh! Thanks..
Do you have a citation to support that acyclovir lowers seizure threshold? Can’t find anything online.