{kind=link}
As an Emergency Medicine doctor we are trained to function in varying degrees of uncertainty. We work in a world of risk of benefits vs harms. When the benefit to harm ratio reaches a threshold for action we are taught to do so swiftly and decisively. Given this, there is no pathology more frustrating than that of TIA. An event that heralds a stroke in the near future and yet so often, this prophesy is too late to prevent the catastrophic future it predicts. The threshold for action has been met and yet we have so few tools of proven benefit with which to intervene. So we give these patients an aspirin, elevate the bed, order a swallow study, and admit for further diagnostic testing. The authors of the recently published NEJM paper on the acute treatment of TIA and minor stroke used dual antiplatelet inhibition in the hopes to reduce recurrent stroke. Given just how many of these patients go on to have a recurrent stroke and the failure of earlier trials attempting such interventions it is entirely appropriate they entitled their paper the CHANCE trial.
TIA has been a vexing problem for Emergency Physicians since 2000 when Johnson et al published their landmark paper in JAMA(2) asserting that 10% of TIA patients will go on to have a full-blown stroke in the next 90 days, with half in the first 48 hours. What followed was a 10-year search to identify a subset of TIA patients who were low risk enough to be safely discharged from the ED for an outpatient evaluation. To do this researchers from California and Great Britain attempted to derive and validate a decision rule to identify this very cohort. They developed the ABCD score, followed by the ABCD2 score, followed by the ABCD2I score, followed by the…
On and on they went, each derivation bringing renewed hope that this time the score would identify a subgroup that was safe for discharge and with each validation those hopes were crushed. The ABCD scores as a whole were expertly derived and validated, and they consistently demonstrated that a higher score correlated with an increased risk of a poor outcome over the next seven days. What the score failed to do was to identify a super low risk group. An ABCD score of 0-1 has consistently been found to have a sensitivity of 98.2% for 2 day risk of recurrent stroke. Unfortunately a specificity of 4% makes it clinically worthless. Using an ABCD2 score of 2 or less drops the sensitivity to 94.7%(4). 1 in 20 will have a recurrent stroke in the next 2 days. This is a risk no physician is comfortable sending home. Given its test characteristics, the ABCD rules in all their derivations have taken a more philosophical role in the management of TIA patients, while doing little to help decision-making in the ED.
What has now become the standard of practice, as well as part of the AHA guidelines for the management of TIA, is to admit these patients for a rapid battery of diagnostic tests (13). Some institutions have initiated a protocol allowing the tests to be done on ED patients, but regardless the standard TIA patient will not leave the hospital without receiving: an MRI of the brain, echocardiogram and some form of imaging of the carotid vasculature. The goal of the expedited workup is to identify a fixable cause of the TIA and initiate treatment that can prevent future strokes. Specifically anticoagulation for those with atrial fibrillation and endarterectomy for those with significant carotid stenosis. The authors of the CHANCE trial attempted to further risk stratify these patients into those who may benefit from dual antiplatelet therapy.
What Wang et al have done is to take the ABCD2 score and instead of using it to identify very low risk patients, they used it to find the TIA patients with the highest risk for stroke and thus may possibly benefit from dual antiplatelet therapy. They chose an ABCD2 score greater or equal to 4. This patient population has an approximate risk of stroke of 8% in the next 7 days (14). Traditionally the ABCD2 score was derived in an attempt to find a test threshold below which the patient could be safely discharged home without an inpatient workup. In this capacity it has consistently failed. What Wang et al did was to instead use it as a treatment threshold above which you would initiate dual antiplatelet therapy. They were attempting to find the metaphoric sweet spot on the gradient that is stroke pathology whose risk of hemorrhagic conversion is low enough and risk of secondary infarct is high enough that they will benefit from the added platelet inhibition that clopidogrel provides. In short they were successful in identifying such a group. Who this group is and to what extent they truly benefitted is a far more complex question.
There is a known risk to adding clopidogrel to aspirin for the treatment of vascular pathologies. Throughout the cardiac trials where clopidogrel and aspirin were compared to aspirin alone there has been a consistent 1% increase in absolute risk of bleeding (8,9,10,11,12). Though adding clopidogrel to aspirin for cardiac patients never demonstrated a significant mortality benefit, researchers were able to find a questionable reduction in rates of myocardial infarction by selecting the highest risk populations. In fact halfway through the CURE trial, published in the NEJM in 2000, the authors altered the inclusion criteria so as to increase the acuity of the population because more patients were being harmed by the increased risk of bleeding than helped by the added platelet inhibition (9).
Past attempts at proving the benefit of dual antiplatelet therapy were done on a stroke population so low risk that the risk of bleeding outweighed the added benefit of clopidogrel. In both the MATCH study and the SPS3 trials the study included only those patients who suffered a stroke within the past 180 days (8,12). Both cohorts were far beyond the high-risk period for having a secondary stroke. The rate of secondary ischemic stroke was 2.4% per year. It would be next to impossible to make a clinically significant difference in an incidence as low as this. It was due to this low acuity that clopidogrel caused more harm than benefit.
It was not until the FASTER trial published in Lancet Neurology in 2007 by Kennedy et al, that a group examined the effects of dual antiplatelet therapy in the hyperacute period directly after symptom onset(3). Using high risk symptoms the authors attempted to identify a population that had a higher rate of large vessel strokes (higher risk of reoccurrence) and high risk TIAs. It was in this population that the authors found success. There was a 3.1% decrease in strokes at 90 days in the clopidogrel + aspirin group compared to the aspirin alone group. As in every other trial there was a 1% increase in the rate of major bleeding in the clopidogrel group, but for the first time they were able to overcome this risk by identifying a population at such high risk for stroke that the risk of hemorrhage was overshadowed.
The authors of the CHANCE trial followed a model constructed by the authors of the FASTER trial, in which they enrolled patients within 24 hours of their TIA or minor stroke. Both groups of investigators hypothesized that since they were capturing patients at the summit of risk for stroke that this group would gain the most benefit from dual antiplatelet therapy. Following this model Wang et al enrolled patients with minor strokes (positive findings on CT or MR and an NIHSS <4) or the highest risk TIA patients (ABCD2 score of a 4 or greater). To ensure the optimal response, the authors excluded all patients with an embolic source, primarily patients with atrial fibrillation. As we know from the ACTIVE trials these patients do not benefit from dual antiplatelet therapy when added to warfarin (5,6). By eliminating these patients from the cohort they increased their likelihood of success and simultaneously decreased their external validity. In fact the authors entire selection process was an attempt to identify the “ideal patient”. Not only did they exclude patients with atrial fibrillation, with their exclusion criteria eliminating sensory only strokes and TIAs with an ABCD2 score less than 4, they attempted to enroll primarily large vessel strokes and TIAs, which from prior research are known to have the highest risk of early reoccurrence (7). In turn ensuring inclusion of as few lacunar sources as possible which from the SPS3 (8) trial we know do not benefit from dual antiplatelet therapy and have and increased risk for bleeding.
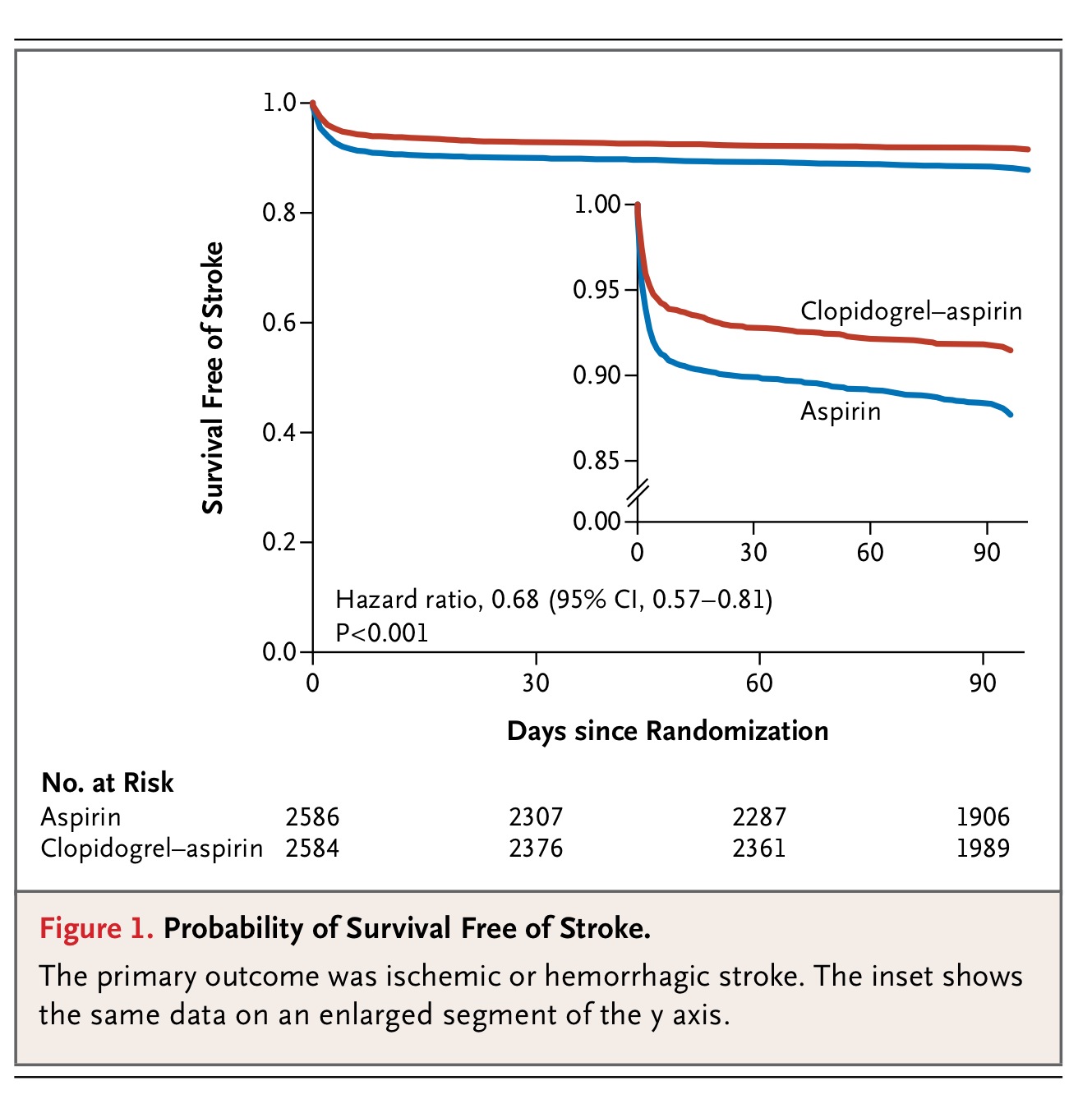
As with the FASTER trial the authors of the CHANCE trial were able to identify a population high enough risk to benefit from dual antiplatelet therapy. Similar to the FASTER trial there was a 3.5% absolute difference in incidence of stroke at 90 days. In fact if you examine the Kaplan-Meyer curve (Figure 1.) you will see that the entire benefit of clopidogrel occurred within the first few days after a patient's stroke or TIA, after which the lines run exactly parallel. Seemingly their theory is true. In this hyperacute period shortly after an acute stroke or TIA, when the patients are at highest risk for a secondary stroke, there is potential to benefit from added platelet inhibition.
{kind=link}
There are a number of caveats that must be considered before starting a patient on clopidogrel after a stroke or TIA. The CHANCE cohort is a highly selected group of patients, all of which have received multiple imaging modalities to grade their event as high risk. They have also been eliminated from having an embolic source for their infarct. Most importantly, nowhere in the authors' documents (article, supplementary appendix, or justification paper) can I find if or how they screened patients for extensive carotid disease, whether these patients were included in the study and if so whether a carotid endarterectomy when appropriate was performed. The only possible mention of such patients can be found in the exclusion criteria:
“Planned or likely revascularization (any angioplasty or vascular surgery) within the next 3 months (if clinically indicated, vascular imaging should be performed prior to randomization whenever possible)”.
Apparently I am not the only reader that found this vague and unclear. In a letter to the editor published in the NEJM on October 3rd 2013 Dr. Stavros and Loannis ask the very same question. They write the following:
“Recent evidence favors early carotid endarterectomy in patients with severe carotid stenosis who have neurologic symptoms similar to those listed as inclusion criteria in this trial. We wonder whether carotid atherosclerosis was identified in patients in the CHANCE trial and, if so, how it was managed in the two study groups. We also wonder about the results of a subgroup analysis stratified according to this characteristic. We suspect that patients with carotid stenosis might have had a more pronounced clinical benefit because of the unstable plaque behavior, which could not only explain at least part of the benefit for patients in this trial, but also help readers to comprehend in-depth the results of the trial.”(15)
The author's reply was frustratingly brief:
“We concur with Kakkos and Tsolakis that patients with carotid stenosis might have had greater clinical benefit with the combination of clopidogrel and aspirin because of the instability of atherosclerosis plaque. We assessed extracranial atherosclerosis in a substudy, and data are not yet available.”(15)
It is possible in China that stroke care is different (a fact the authors state as a limitation in their discussion section) and patients are not rapidly screened for carotid pathology that may be the source of the infarct(1). We know that medical therapy is far inferior to surgical intervention for symptomatic carotid stenosis(16). It may be that patients with carotid stenosis who do not undergo carotid endarterectomy benefit from added platelet inhibition. The CLAIR trial published in Lancet Neurology in 2007 may suggest both of these points (17). This was a RCT conducted in China examining whether patients after a TIA or minor stroke who had large vessel disease benefited from the added inhibition clopidogrel provides. Though there were some surrogate endpoints that suggested benefit, none of these patients received carotid endarterectomies. Without a more definitive answer to this question it is difficult to interpret the data from the CHANCE trial. (hopefully the authors have a future publication planned that will answer this question).
The authors of the CHANCE trial have managed to identify a group of patients who may benefit from clopidogrel after a stroke or TIA, but these are not the undifferentiated patients we see in the Emergency Department. This trial is the perfect example of a high acuity bias and how through the use of rigid inclusion and exclusion criteria a benefit can be found. There may be a group of ED patients who would benefit from clopidogrel, but unfortunately because CHANCE's exclusion criteria and the uncertainty involving patients with carotid stenosis, this trial does not provide us those answers. We can hope that trials in progress, such as the POINT trial and the TARDIS trial (For all the Who fans we hope this answers the question once and for all, “are two hearts are better than one no matter what antiplatelet agent you take?” ), may help guide us as to which patients in the ED may benefit from added platelet inhibition. Until then we must continue to balance the risk of harm and the CHANCE of benefit clopidogrel may provide our patients.
A brief aside, I just want to express my gratitude to Dr. Mike Cadogan for his help. As most of you I am sure aware Dr. Cadogan has single-handedly converted almost the entirety of the FOAMverse to wordpress. It is thanks to him I have this brand new shiny website. For this and for his support I thank him. He truly is the Godfather of FOAM.
Sources Cited:
1. Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-19.
2. Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA 2000;284:2901-2906.
3. Kennedy et al et all. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomized controlled pilot trial. Lancet Neurol. 2007 Nov;6(11):961-9.
4. Perry et al. Prospective validation of the ABCD2 score for patients in the emergency department with transient ischemic attack. CMAJ July 12, 2011 vol. 183 no. 10.
5. ACTIVE Investigators Effect of Clopidogrel Added to Aspirin in Patients with Atrial Fibrillation. N Engl J Med 2009; 360:2066-2078.
6. ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomized controlled trial (2006) Lancet, 367 (9526) , pp. 1903-1912.
7. Lovett et al. Early risk of recurrence by subtype of ischemic stroke in population-based incidence studies Neurology 2004 62:569-573.
8. The SPS3 Investigators Effects of Clopidogrel Added to Aspirin in Patients with Recent Lacunar Stroke. N Engl J Med 2012; 367:817-825.
9. The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N Engl J Med 2001; 345:494-502.
10. COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group Addition of clopidogrel to aspirin in 45?852 patients with acute myocardial infarction: randomised placebo-controlled trial. The Lancet – 5 November 2005; Vol. 366, Issue 9497, Pages 1607-1621.
11. The CLARITY Study Group et al. A Placebo-Controlled Trial of Oral Cladribine for Relapsing Multiple Sclerosis. N Engl J Med 2010; 362:416-426.
12. Diener et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004 Jul 24-30;364(9431):331-7.
13. Easton et al. Definition and Evaluation of Transient Ischemic Attack: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease: The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40:2276-2293.
14. Johnson et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack The Lancet – 27 January 2007; Vol. 369, Issue 9558, Pages 283-292.
15. Letter to Editor, Clopidogrel with Aspirin in Minor Stroke or Transient Ischemic Attack N Engl J Med. 2013 Oct; 369:1375-1377.
16. North American Symptomatic Carotid Endarterectomy Trial CollaboratorsBeneficial Effect of Carotid Endarterectomy in Symptomatic Patients with High-Grade Carotid Stenosis. N Engl J Med. 1991 Aug; 325:445-453.
17. Wong et al. Clopidogrel plus aspirin versus aspirin alone for reducing embolisation in patients with acute symptomatic cerebral or carotid artery stenosis (CLAIR study): a randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010 May;9(5):489-97.

University of Georgetown
Resuscitation and Critical Care Fellowship Graduate
Creator
EMNerd.com
- EM Nerd-The Case of the Partial Cohort - May 24, 2020
- EM Nerd: The Case of the Sour Remedy Continues - January 20, 2020
- EM Nerd-The Case of the Adjacent Contradictions - December 23, 2019
love your blog. content is on point. i’m also really impressed with your design. suggestions for making a more awesomely designed blog for a novice blogger like me? i’m not a programmer, but i’m enthusiastic to learn even more technical means of making a cool blog.
Thanks for the support! I unfortunately I cannot take credit for the site design. That is entirely the brilliant work of Dr. Mike Cadogan from Life in the Fast Lane. I, like you am a novice blogger who up until last week was fumbling through my tumblr posts. Here’s to the FOAMed family!!
Happy to help…drop me a line