
Standard approach to Torsade de Pointes (TdP)
 A common approach to TdP is shown above. The initial episode is controlled with magnesium and perhaps defibrillation. The patient is sent to ICU for close observation. Usually the patient will be fine, but sometimes TdP does recur. Recurrence triggers second-tier therapies, often including overdrive pacing.
A common approach to TdP is shown above. The initial episode is controlled with magnesium and perhaps defibrillation. The patient is sent to ICU for close observation. Usually the patient will be fine, but sometimes TdP does recur. Recurrence triggers second-tier therapies, often including overdrive pacing.
Why the standard approach fails
 This is largely a matter of pharmacokinetics:
This is largely a matter of pharmacokinetics:
- Magnesium is poorly absorbed by cardiomyocytes. Following a bolus of 2-4 grams of magnesium, relatively little magnesium gets into cardiac tissue. Most is excreted in the urine. Unless the patient has severe renal failure, magnesium levels will drop back to baseline over several hours (figure below).1
- Conditions that cause TdP often out-last a single bolus of magnesium. For example, dofetilide is a common cause. With a half-life of 10 hours, dofetilide will lurk around long after the magnesium bolus has worn off.
 This is analogous to treating a methadone overdose with naloxone. Naloxone works great, but it wears off rapidly. Methadone easily out-lasts the naloxone, so a single bolus of naloxone only works transiently. A naloxone infusion is needed for sustained efficacy.
This is analogous to treating a methadone overdose with naloxone. Naloxone works great, but it wears off rapidly. Methadone easily out-lasts the naloxone, so a single bolus of naloxone only works transiently. A naloxone infusion is needed for sustained efficacy.
The standard approach to TdP will therefore sometimes lead to TdP recurrence. In a critical care unit, the vast majority of these patients will do OK. However, TdP recurrence may trigger invasive interventions (e.g. defibrillation, intubation, insertion of a temporary transvenous pacemaker). Complications from these interventions can include aspiration pneumonia and broken ribs. Recurrent TdP rarely kills someone within the ICU, but it’s still harmful.
A better approach to TdP
 My preferred approach to TdP is shown above. Following resolution of the initial episode, the patient is immediately placed on a protocolized magnesium infusion, as shown below.2
My preferred approach to TdP is shown above. Following resolution of the initial episode, the patient is immediately placed on a protocolized magnesium infusion, as shown below.2
 The rationale for using a magnesium infusion is as follows:
The rationale for using a magnesium infusion is as follows:
- A magnesium infusion will maintain elevated magnesium levels for at least 24 hours. Like a naloxone infusion for methadone poisoning, this will allow magnesium to out-last other drugs that caused the TdP (e.g. dofetilide).
- Many patients with TdP have an intracellular magnesium deficiency (which can occur despite normal serum levels, since most magnesium is located intracellularly). Magnesium isn’t absorbed by cells very efficiently, so a couple grams of magnesium won’t replete the intracellular magnesium deficiency. However, a 24-hour exposure to elevated serum magnesium allows magnesium to eventually soak into the cardiomyocytes. Repletion of intracellular magnesium stores provides ongoing protection against TdP, even after the infusion is stopped and the patient leaves the ICU.
- A protocolized magnesium infusion is quite safe. Compared to the risk of recurrent arrhythmia and cardiac arrest from inadequately treated TdP, magnesium infusion is almost certainly the safer route to go.
The protocol should be included in the patient’s chart in a prominent location, so that everyone caring for the patient can literally be “on the same page.” This is essential to achieve continuation of the magnesium infusion. Without a well-defined protocol, high serum magnesium levels will provoke anxiety, causing the infusion to be shut off prematurely.
Some more detail about the magnesium infusion
The magnesium protocol shown above is based on clinical trials involving atrial fibrillation (in fact, it is more conservative than these studies, to establish a greater margin of safety). Thus, there is a literature base demonstrating that this is safe among sick ICU patients, in the absence of severe renal failure.3 4
 Magnesium infusions for TdP are often mentioned in textbooks (e.g. UpToDate above). In fact, the classic paper that originally introduced the use of magnesium for TdP reported using magnesium infusions in 9 of 12 patients treated.5 In six of these patients, magnesium infusion was given preemptively following the first episode of TdP, as advocated in this post. The magnesium infusion protocol shown above fits within the range of magnesium infusion rates which is recommended by these sources (3-20 mg/min equals 0.2-1.2 grams/hr).
Magnesium infusions for TdP are often mentioned in textbooks (e.g. UpToDate above). In fact, the classic paper that originally introduced the use of magnesium for TdP reported using magnesium infusions in 9 of 12 patients treated.5 In six of these patients, magnesium infusion was given preemptively following the first episode of TdP, as advocated in this post. The magnesium infusion protocol shown above fits within the range of magnesium infusion rates which is recommended by these sources (3-20 mg/min equals 0.2-1.2 grams/hr).
Why aren’t magnesium infusions used more often? Logistics. Textbooks or articles often include a single line recommending a magnesium infusion (e.g. UpToDate above, Tintinalli’s below). It’s hard to translate this into safe clinical practice at the bedside. What exactly should the rate be? How should it be monitored? The use of a standardized, validated magnesium infusion protocol allows this recommendation to be translated into bedside management.
 By starting at a higher rate and then down-titrating the infusion rate as needed, the magnesium protocol is designed to match the physiology of magnesium uptake by the body. Many patients begin with a total body magnesium deficiency. Initially, such patients may clear magnesium from their blood at a relatively rapid rate. As intracellular stores become repleted, magnesium starts accumulating in the blood. The protocol recognizes that the serum magnesium level is rising, so it reduces the magnesium infusion rate accordingly.
By starting at a higher rate and then down-titrating the infusion rate as needed, the magnesium protocol is designed to match the physiology of magnesium uptake by the body. Many patients begin with a total body magnesium deficiency. Initially, such patients may clear magnesium from their blood at a relatively rapid rate. As intracellular stores become repleted, magnesium starts accumulating in the blood. The protocol recognizes that the serum magnesium level is rising, so it reduces the magnesium infusion rate accordingly.
A 24-hour magnesium infusion is generally adequate, for the following reasons. First, 24 hours should be sufficient to replete intracellular magnesium stores. Second, 24 hours is usually adequate to allow various other TdP-inducing drugs to wash out of circulation. Third, most patients will be in the ICU for a day after an episode of TdP anyway, so a 24-hour infusion won’t delay disposition. However, if the patient still has a prolonged QTc after the 24-hour infusion and is felt to be at risk for recurrent TdP, the infusion could certainly be continued longer.5
What is the target magnesium level for a TdP patient?
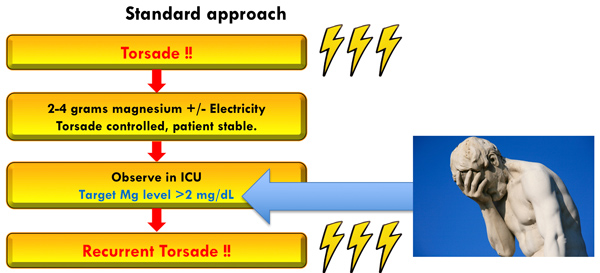 A popular practice is to target a magnesium level >2 mg/dL following TdP. This is illogical, for the following reason. It’s universally acknowledged that IV magnesium is effective for TdP even if the serum magnesium level is normal. This proves that a “therapeutic” magnesium level for TdP is above normal.
A popular practice is to target a magnesium level >2 mg/dL following TdP. This is illogical, for the following reason. It’s universally acknowledged that IV magnesium is effective for TdP even if the serum magnesium level is normal. This proves that a “therapeutic” magnesium level for TdP is above normal.
 Nobody knows what the ideal magnesium level is for treating adult TdP. Targeting a level of 3.5-5 mg/dL is based on the following lines of evidence, which seem to line up reasonably well:
Nobody knows what the ideal magnesium level is for treating adult TdP. Targeting a level of 3.5-5 mg/dL is based on the following lines of evidence, which seem to line up reasonably well:
- The protocol above shoots for a magnesium level of 3.5-5 mg/dL, because this was used for validated magnesium protocols in treating atrial fibrillation.6
- Bellomo et al. recently suggested a similar target range in post-surgical patients with a goal of preventing atrial fibrillation (3.4-5.8 mg/dL).1
- Among children with long-QT syndrome, a magnesium bolus which terminated TdP generated serum magnesium levels of 2.9-5.4 mg/dL.7
- Among adults treated with magnesium for TdP, post-treatment magnesium levels ranged between 3.2-12 mg/dL (with most in the ~3.5-4.5 mg/dL range).5,8
Magnesium infusion protocol: experience at Genius General Hospital
complication #731 from chronic opioid use: methadone-induced torsade. don’t worry: magnesium infusion crushed this & patient did fine. #MAGnification https://t.co/J9zYWAW0hy pic.twitter.com/l3R7qmjy4q
— 𝙟𝙤𝙨𝙝 𝙛𝙖𝙧𝙠𝙖𝙨 (he/him) 💊 (@PulmCrit) December 29, 2017
I've been using this magnesium protocol for four years among selected patients with atrial fibrillation and all patients with TdP (excluding those with GFR<30 ml/min). My impressions are as follows:
- The protocol is easy to use (even for folks without experience using magnesium infusions).
- The protocol appears to be quite safe. Very rarely a patient might accumulate magnesium and develop a rather high level (e.g. 8 mg/dL), but to date this has not caused any clinical signs or symptoms of hypermagnesemia.
- My guess is that the infusion has been used by us for about a dozen patients with TdP. It has been uniformly effective for TdP, including recalcitrant cases which outside hospital cardiologists were struggling with.9
- The magnesium infusion protocol has transformed TdP from something occasionally challenging into something which is uniformly boring. Instead of occasionally crashing, patients just sit around watching television and getting magnesium.
 Repletion of magnesium in patients with GFR<30 ml/min
Repletion of magnesium in patients with GFR<30 ml/min

Some studies have used magnesium infusions for patients with GFR<30 ml/min. They’re likely safe in the 15-30 ml/min GFR range. However, the safest approach here is probably to follow levels carefully (e.g. q4hr) and give 2-4 grams magnesium as needed. The key here is to shoot for a therapeutic magnesium level of ~3.5-5 mg/dL (as discussed above).
Magnesium is cleared by the kidneys. Therefore, extra caution is required for a patient who is anuric (if you overshoot, you will be stuck). Alternatively, it’s safe to be a bit more aggressive in a patient with GFR 15-30 ml/min who is producing urine.
Controversy: Some articles recommend low magnesium dosing
The magnesium protocol, doses, and target levels listed above are consistent with the bulk of published evidence on TdP (including standard references such as UpToDate and Tintinalli's). However, recommended doses vary widely, with some authors recommending low doses. For example, Charlton et al. recommended an infusion at 0.18-0.6 grams/hour.10 Infusion at very low doses may fail to work. Indeed, Charlton’s publication focuses on three patients who were “refractory” to magnesium and consequently required overdrive pacing. I suspect that an adequate magnesium infusion regimen would have been successful, thereby abrogating the need for overdrive pacing.11 Although this article is framed as an illustration of the strengths of overdrive pacing, it may actually represent a cautionary tale regarding the complications of inadequate magnesium dosing.

- Magnesium is the naloxone of TdP: it works great temporarily, but TdP may recur after magnesium is excreted by the kidneys.
- After an episode of TdP, the optimal magnesium level seems to be ~3.5-5 mg/dL (not the traditional target of Mg >2 mg/dL).
- Initiation of a protocolized magnesium infusion immediately following the first episode of TdP may prevent recurrence and thereby avoid complications (e.g. cardiac arrest, rib fractures). This is part of textbook management of TdP, but it is underutilized because the nuts & bolts of running an infusion are unclear.
- A standardized, evidence-based magnesium infusion protocol may increase the ease and safety of magnesium infusions. This translates magnesium infusion into something which is reproducibly achievable at the bedside.
- Patients with impaired renal function (GFR<30 ml/min) may be treated with repeated measurement of magnesium levels and PRN boluses, with a target magnesium level of 3.5-5 mg/dL.
Related
- Mg infusions for AF and TdP (PulmCrit) – This earlier post focuses mostly on AF.
- Torsade de Pointes (First 10 in EM)
Addendum: by popular demand a Mg protocol using SI units:
 References
References

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Interesting post, thanks. Can we have it in SI units as well please? (After all pretty much everywhere in the world outside the US uses SI units).
sure, I added a Mg protocol using SI units (see the bottom of the post)
(to convert from mg/dL to mMol multiply by 0.412)
(to convert from grams to mMol multiply by 8.3)
Thanks Josh
Dear dr. Farkas,
great article, I`ve already printed the protocol and have it in my notebook!
I have one question – I was double-cheking the conversion to SI units and found two different formulas in my sources. One of them gives the same numbers as stated in your protocol but according to the other 1 g of magnesium sulfate is equivalent to about 4 mmols of magnesium, 4 grams thus being equal to 16 mmols.
Could you double check these calculations? Thank you!
Thank you Dr. Farkas. What a-fib patients would you recommend treating with mag? In my service area Cardizem has become scarce and our treatment protocols now edge us in the direction of utilizing Lopressor as a first line treatment in stable patients with rapid a-fib. Any thoughts you have are appreciated.
see the blog about this here: https://emcrit.org/pulmcrit/magnesium-infusions-for-atrial-fibrillation-torsade/ Overall can be used in a similar fashion to amiodarone – it may be used to cardiovert patients into sinus or simply for rate control. Works best in patients with total body Mg deficiency (but this can occur with a normal serum Mg level, so a normal Mg level doesn’t mean that the drip is worthless). It’s not incredibly powerful but it is safe – causes less hypotension than metoprol0l/diltiazem. Often used as an adjunct with another agent because alone it may not be sufficient.
Very cool, as usual, Josh. excellent post.
it would be interesting to see what a mag drip in our place would look like. it seems to create (at least in the few times i used it for pre-eclampsia) a major bit of work for the nursing staff.
but this post seems to bear out its utility. so thanks again.
tom
good luck, a simple protocol should take a lot of the work out of it. once you’ve done this a couple times it’s not a big deal.
Very important topic! What apresentations of IV magnesium do you have there in USA? Here in Brazil the apresentation usually avaiable is 10 mL of MgSO4 50%. How would you make your solution to give the 1g/hour infusion? Is there a ideal concentration of the solution? Thanks!!!
40 mg/ml of MgSO4 in water is probably the most common concentration that I’ve seen here in the U.S. It’s usually packaged as 40 grams in a liter, 4 grams in 100 ml, and less commonly (from my encounters), 20 grams in 500 ml.
Very important topic!! I would like to known how IV magnesium is supplied in the USA? Here in Brazil the apresentation usually avaiable is 10 mL of MgSO4 50%? How would you make your solution to give the 1g/hour infusion? Is there a ideal concentration? Thanks!!!