Introduction
Sepsis is a broadly defined syndrome, encompassing dozens of diseases. Could sepsis be split into smaller, more biologically homogeneous groups of patients, who might respond similarly to therapy? This could allow a more personalized approach to sepsis care.
Since the 1980s it has been recognized that some patients with sepsis also develop hemophagocytic lymphocytosis (Risdall 1984). For decades this was believed to be extremely rare. However, currently there is increasing recognition that this combination might represent a significant fraction of sepsis patients (Shakoory 2016, Beutel 2011).
What is hemophagocytic lymphohistiocytosis (HLH)?
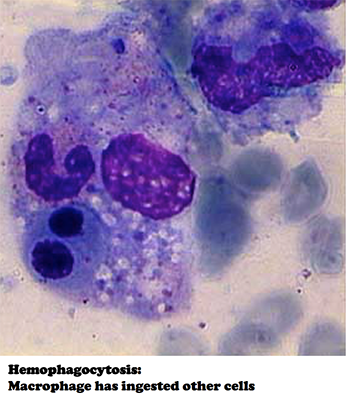 HLH (a.k.a., hemophagocytic syndrome, macrophage activation syndrome) is a clinical syndrome resulting from immunological hyperactivation centered around macrophages (1). It involves a pro-inflammatory cytokine storm with high levels of many cytokines (e.g., IL-1, IL-6, and IL-8). The histological signature of this process is activated macrophages phagocytizing other cells (hemophagocytosis, adjacent image).
HLH (a.k.a., hemophagocytic syndrome, macrophage activation syndrome) is a clinical syndrome resulting from immunological hyperactivation centered around macrophages (1). It involves a pro-inflammatory cytokine storm with high levels of many cytokines (e.g., IL-1, IL-6, and IL-8). The histological signature of this process is activated macrophages phagocytizing other cells (hemophagocytosis, adjacent image).
HLH may be triggered by a variety of factors (e.g., infection, malignancy, autoimmune disease) or it may occur in children with genetic predisposition. Regardless, the features of HLH may include:
- fever
- shock, capillary leak syndrome, ARDS
- cytopenias
- abnormal liver tests
- disseminated intravascular coagulation
- delirium, seizure
- lymphadenopathy, hepatomegaly, splenomegaly
- markedly elevated inflammatory markers (ferritin, CRP, procalcitonin)
- multiorgan failure (including cardiomyopathy), death
What is the relationship between sepsis and HLH?
HLH can cause all of the features of septic shock. Therefore, HLH is traditionally regarded as a “sepsis mimic.” For example, HLH due to rheumatologic disease sometimes masquerades as sepsis.
However, HLH may also be triggered by infection. In this case, the patient has both conditions simultaneously: sepsis-HLH overlap syndrome (SHLHOS)(2). SHLHOS probably represents a subgroup of septic patients, where infection triggers macrophage activation that spirals out of control (Raschke 2011).
Approach to diagnosing SHLHOS?
Diagnosing HLH is challenging, with disagreement even among experts (3). The consensus definition is:
Diagnostic criteria for HLH (at least five)
- Fever
- Splenomegaly
- Cytopenia in at least two cell lines
- Hemoglobin < 9 mg/dL
- Platelets < 100 billion/L
- Neutrophils < 1,000 / microliter
- Hypertriglyceridemia and/or hypofibrinogenemia
- Triglycerides >265 mg/dL
- Fibrinogen < 150 mg/dL
- Hemophagocytosis in bone marrow, spleen, or lymph node biopsy (4)
- Ferritin >500 ng/ml
- Low natural killer-cell activity (5)
- Soluble CD25 (i.e. soluble IL-2 receptor) > 2,400 U/ml
Like may diagnostic criteria, these shouldn't be applied in a rigid fashion. Critically ill patients with HLH may not meet formal diagnostic criteria until they are nearly dead (Ansuini 2013). Diagnosis is ultimately a matter of clinical judgment, with careful consideration of clinical context and competing diagnoses.
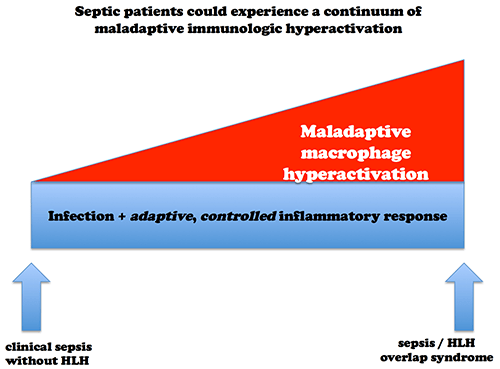
Differentiating between SHLHOS vs. uncomplicated sepsis is challenging, because both disorders cause a similar presentation. Furthermore, SHLHOS may represent a severe form of sepsis, with no clear dividing line between SHLHOS and sepsis (figure above).
SHLHOS may be more common than traditionally thought
Several studies have described a subset of sepsis patients with cytopenias and increased cytokine levels. Fjell 2013 analyzed levels of 39 cytokines among 363 patients with septic shock, with cluster analysis identifying a group of 47 patients with the highest levels of cytokines, greatest mortality, thrombocytopenia, and relative leukopenia (6). Other studies have confirmed a relationship between thrombocytopenia and higher cytokine levels among septic patients (Tsirigotis 2016, Claushuis 2016).
Hemophagocytosis is not often encountered in routine clinical practice (even if a biopsy is performed, hemophagocytosis may be missed)(7). However, autopsy studies suggest that this may be more common than recognized:
- Strauss 2004 found moderate to severe hemophagocytosis within the bone marrow of 35/107 patients who died in the medical ICU. Hemophagocytosis correlated with sepsis, coagulopathy, and hyperbilirubinemia.
- Inai 2014 found hemophagocytosis in bone marrow among 13/18 patients who died from sepsis. Hemophagocytosis correlated with elevated levels inflammatory cytokines involved in HLH (IL-1, IL-6, and IL-8).
- Schaer 2006 found bone marrow infiltration by macrophages and hemophagocytosis to be common among 28 patients who died of sepsis, but not controls who died following trauma.
Four prospective studies have specifically looked for hemophagocytosis in the context of sepsis:
- Francois 1997 and Stephan 1997 both prospectively evaluated bone marrow biopsies among ICU patients with sepsis and unexplained thrombocytopenia (8). Both found hemophagocytosis among ~60% of patients. Francois et al. found that hemophagocytosis correlated with higher levels of ferritin (average 1,822 ng/ml) and the cytokine M-CSF, greater organ dysfunction, and increased mortality.
- Kuwata 2006 evaluated patients presenting with SIRS for hemophagocytosis in their peripheral blood, using a special blood smear technique. Peripheral hemophagocytosis was detected in 40/322 patients, a finding that correlated with increased mortality (53% vs. 6%, p<0.01) and higher levels of cytokines (including IL-1, IL-6, and soluble IL-2 receptor). Although some patients with hemophagocytosis had underlying malignancy, 73% had underlying infection (mostly pneumonia).
- Beutel 2011 prospectively evaluated for SHLHOS among critically ill patients with H1N1 influenza. HLH was detected in 9/25 patients, among whom the mortality rate was markedly increased (8/9).
Overall, epidemiologic data is sparse. Available data suggests that a subset of extremely ill sepsis patients have HLH. In centers with greater awareness of HLH, these cases are detected more often.
Treatment implications of SHLHOS
Pediatric literature
Based on experience gained from children with primary HLH, pediatric intensivists are a decade ahead of adult intensivists with regards to recognizing and treating SHLHOS. Primary HLH is typically treated with a regimen involving dexamethasone, cyclosporine, and etoposide (a chemotherapeutic agent). Some reports have described using etoposide for SHLHOS, but this is associated with high mortality. Current consensus is that etoposide isn’t beneficial for SHLHOS (Giri 2013, Demirkol 2012, Simon 2014).
Carcillo 2015 describes current management strategies for pediatric SHLHOS used at the University of Pittsburgh. In addition to usual sepsis therapies, these authors recommend immunosuppression with a combination of methylprednisolone, IVIG, and anakinra (recombinant IL-1 receptor antagonist). For patients with multi-organ failure, they also use plasma exchange therapy. Other authors have also reported success with steroid and anakinra (Rajasekaran 2014). Unfortunately no high-level evidence is currently available (Demirkol 2014).
Adult literature: anakinra
A large multi-center RCT found that anakinra caused a 3% reduction in mortality from septic shock, but this difference was statistically insignificant (Opal 1997). Shakoory 2016 later re-analyzed the study, focusing on a group of patients with hepatobiliary dysfunction and disseminated intravascular coagulation (surrogate markers for SHLHOS). Among 763 patients in the original study, 43 patients met these criteria. Within this patient subset, anakinra had a substantial survival benefit (65% vs. 35%, p=0.0006; figure below). Given its post-hoc design, this study is only hypothesis-generating. Nonetheless, the ability to isolate a high-mortality group of patients who benefit from immunomodulation is promising.

Steroid in adult SHLHOS?
Consider the following:
- Steroid appears to have the most benefit among the sickest patients with septic shock.
- SHLHOS defines a subgroup of the septic shock patients with high mortality.
- SHLHOS patients have a truly dysregulated, hyperactive inflammatory response, which in theory could respond to steroid.
- Steroid is an accepted therapy for HLH and pediatric SHLHOS.
SHLHOS might identify a subset of septic patients who benefit from steroid. Identifying such patients could facilitate steroid therapy in a timely and rational fashion. This might make more biological sense than the traditional approach to steroid therapy (waiting until patients develop refractory shock and then trying to rescue them with steroid).
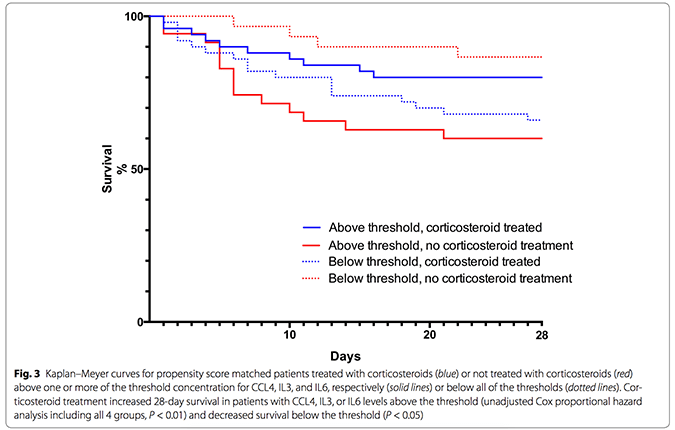
A recent propensity-matching study compared septic patients with similar clinical characteristics who did or didn't receive steroid (Bentzer 2016). Patients with higher levels of several cytokines appeared to obtain a mortality benefit from steroid (9). Among cytokines with the strongest linkage to benefit from steroid, several have been implicated in macrophage activation (e.g. IL6, macrophage inflammatory protein 1-beta, CD40 ligand, granulocyte colony stimulating factor).
Perhaps the most provocative finding in Bentzer 2016 was that steroid appeared to improve mortality among patients with high cytokine levels, but simultaneously worsened mortality among patients with low cytokine levels (figure below). Among the entire population, steroid had a neutral effect. Thus, when the entire population is studied as a whole it appears that steroid is doing nothing, but in fact steroid may be helping some patients while hurting others (9).
A more biologically meaningful definition than “sepsis”?
According to SEPSIS-3.0, “Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection.” This is a nice conceptual definition, but the associated clinical criteria fail to identify which patients truly have a dysregulated host response. For example, clinical criteria for sepsis could be met either by:
- (a) previously healthy person with maladaptive, dysregulated immune response to illness causing shock
- (b) chronically ill person without physiologic reserves, who develops shock due to an infection with an appropriate, well-regulated immune response
This distinction matters. Sepsis has been a graveyard for immunomodulatory therapies. Decades of failure could reflect using therapies indiscriminately, among heterogeneous patients with widely varying levels of immune activation.
SHLHOS may represent a subset of patients with sepsis who have very high mortality and are truly suffering from dysregulated immune hyperactivity. Identifying these patients might allow us to select those who would benefit most from immunomodulation.

- Hemophagocytic lymphohistiocytosis (HLH) is a syndrome resulting from immunologic hyperactivation centering on macrophages. It may be caused by infection, cancer, or rheumatologic disease.
- Clinically, HLH causes fever, shock, capillary leak, thrombocytopenia, delirium, disseminated intravascular coagulation, and multiorgan failure.
- Patients with HLH due to infection have a combination of sepsis and HLH (sepsis-HLH overlap syndrome, SHLHOS). SHLHOS represents a subset of sepsis patients with intense immunologic hyperactivation and high mortality.
- Ideal treatment for SHLHOS might be a combination of therapies for sepsis (e.g. antibiotics, supportive care) as well as immunosupressive therapies for HLH (e.g. steroid, possibly anakinra).
Related posts
- HLH… the white whale of hematology (Maryland CC project)
- Top ten problems with SEPSIS-3.0
- Sepsis stuff:
Notes
- Technically macrophage activation syndrome (MAS) is intended to refer only to HLH which is triggered by rheumatologic diseases. However, sometimes this term is used in a more general fashion to refer to HLH.
- Some authors have referred to this as “sepsis / hemophagocytic lymphohistiocytosis / macrophage activation overlap syndrome” or “hyperferritinemic sepsis-related multiple organ dysfunction syndrome / macrophage activation syndrome / secondary hemophagocytic lymphohistiocytosis.” SHLHOS is used here for the sake of brevity. Indeed, there is little agreement regarding the nomenclature used to describe these patients. As lamented by Carcillo 2015 “when hyperferritinemic sepsis as associated with five of eight criteria reflective of hyperinflammation … it might be called multiple organ dysfunction syndrome (MODS) by intensivists, macrophage activation syndrome (MAS) by rheumatologists, and hemophagocytic lymphohistiocytosis (HLH) by oncologists.”
- To illustrate just how subjective and murky this diagnosis can be, Riviere 2014 performed a retrospective case series of 162 patients with possible HLH. As part of the study, three experts independently reviewed the patients' charts. Experts only agreed on the diagnosis of HLH in 57% of cases. In many cases, even after the three experts discussed the case and invited a fourth expert to adjudicate, they were still unable to reach agreement about the diagnosis.
- Of course, most patients with sepsis won't receive a tissue biopsy. To complicate matters further, the diagnosis of hemophagocytosis is tricky and may be missed if the hematopathologist isn't looking for it.
- Generally neither NK cell activity nor sIL-2 receptor levels are obtainable rapidly enough to affect clinical decision making in the ICU.
- Although these patients tended to have a normal WBC count, this is arguably “inappropriately” low given the high severity of their sepsis syndrome. Compared to other clusters of patients, these 47 patients had lower WBC counts despite being sicker.
- Rates of hemophagocytosis observed on biopsy vary, and seem to be quite high within research studies. High rates observed in research studies are probably a reflection that these studies typically utilize specific immunohistochemical statins that highlight macrophages, while looking specifically for hemophagocytosis. Additionally, different studies use conflicting criteria to define hemophagocytosis.
- Note that these are selected populations. First, only patients sick enough to require ICU admission were studied. Second, Francois 1997 included only about half of patients with sepsis and thrombocytopenia because it excluded any patient with known hematologic disease, prior chemotherapy, major bleeding and/or prior transfusion of any blood component, disseminated intravascular coagulopathy, or prior administration of heparin.
- Please note that since this is a propensity-matching study, it cannot prove causality. This study is included here for hypothesis generation only.
Image credits: Image of hemophagocytosis from wikipedia. Cytokine storm image from Tisoncik JR et al. 2012.
{kind=link}

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Really interesting topic, The one patient with HLH I diagnosed had a ferritin of 35,000, but I wonder how many we might be missing. Also, I think you really hit the nail on the head on our dogmatic reliance of RCTs that we use to provide care to ALL patients. So many positive results that don’t apply to everyone, and negative results where the intervention definitely does work in some subgroups.
Very cool analysis of an entity i am ashamed to say that i am newly learning about.
very good, Josh
thank you
super illustrative review and description, excellent as always, Josh. thank you.
tom
Do you think that sHLH is is main pathophysiology in COVID-19 ? could immunosuppressive therapy have some role in the treatment