 Introduction with a clinical question
Introduction with a clinical question

A young woman is transferred to the ICU from an outside hospital due to severely depressed mental status, thought due to intoxication. You evaluate her intracranial pressure using ocular ultrasonography. Evaluation of the optic disc diameter in both eyes and in both orientations yields four measurements: 5.5 mm and 6.0 mm (left eye) and 5.7 mm and 5.9 mm (right eye). A representative image is below. Does this patient have intracranial pressure (ICP) elevation? Or is this examination indeterminate?
 The problem
The problem
The most widely used and validated method of evaluating ICP elevation is measuring the optic nerve sheath diameter 3 mm behind the eye. This may be interpreted roughly as follows:
- <5 mm is normal
- 5-6 mm is a grey zone
- >6 mm is abnormal, suggesting ICP elevation
This is a fast and easy examination which can yield useful information. The following 5-minute video by Jacob Avila contains everything you need to know:
The problem is that a lot of patients fall into the ~5-6 mm grey zone. It would be useful to have additional features to help sort out these patients.
Papilledema
Papilledema refers to edema of the retinal disc caused by elevated ICP. This was traditionally diagnosed with an ophthalmoscope, as shown in this unrealistically crisp image:

Ophthalmoscopy is arduous and rarely performed in critical care practice. Fortunately, papilledema may also be detected using ocular ultrasonography (figure below). This is convenient, because papilledema can be observed using the same view used to determine optic nerve sheath diameter. Thus, looking for papilledema doesn't actually take any additional time, it just requires being slightly more observant.

This video from Sinai EM Ultrasound shows papilledema in cine:
This video from MGH Ultrasound compares normal vs. papilledema in a less dramatic example:
Diagnostic performance?
- Lochner 2016 performed a prospective multicenter study comparing 21 patients with known intracranial hypertension versus age-matched controls. Ultrasonographic papilledema was present bilaterally in 20/21 (95%) of patients with intracranial hypertension, but was absent bilaterally in all 21 control patients. Papilledema out-performed optic nerve sheath diameter (which had 93% sensitivity and 67% specificity, using a cutoff of 5.9 mm).
- Carter 2014 found ultrasonography to be 90% sensitive for papilledema in a retrospective chart-review series of 87 patients.
- Teismann 2013 found that optic disc height on ultrasonography correlated well with optical coherence tomography among 14 patients evaluated in an ophthalmology clinic (r = 0.84; figure below). One strength of this study is that sonography was performed by emergency physicians, rather than ultrasound technicians.
- Bauerle 2011 performed a prospective study involving 10 patients diagnosed with idiopathic intracranial hypertension and 25 patients with neurologic disorders not associated with intracranial hypertension. Ultrasonographic papilledema was present bilaterally in 9/10 patients and absent in 25/25 control patients. Papilledema out-performed optic nerve sheath diameter (which had 90% sensitivity but only 84% specificity using a cutoff value of 5.8 mm).
 The above studies aren’t perfectly translatable into acute-care medicine, because they were done in outpatient clinics. In particular, they fail to evaluate the performance of ultrasonographic papilledema for acute elevation in intracranial pressure (which may be lower, because papilledema can take some time to develop). Nonetheless, they demonstrate the concept that ultrasonography can detect papilledema.
The above studies aren’t perfectly translatable into acute-care medicine, because they were done in outpatient clinics. In particular, they fail to evaluate the performance of ultrasonographic papilledema for acute elevation in intracranial pressure (which may be lower, because papilledema can take some time to develop). Nonetheless, they demonstrate the concept that ultrasonography can detect papilledema.
Some authors have measured the degree of optic nerve elevation. However, there is disagreement about the optimal cutoff for this distance. Thus, a qualitative approach is probably best at this point. Ongoing experience and review of video clips at monthly educational conferences will establish an appreciation for what is normal vs. abnormal (1).
Papilledema… or pseudopapilledema?
Pseudopapilledema refers to anything causing optic nerve edema other than ICP elevation. These include the following:
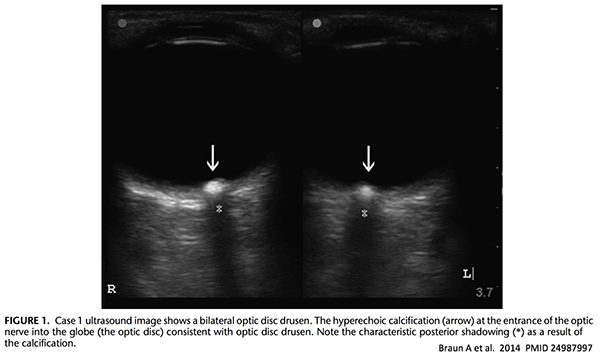
- Optic Disc Drusen: these are essentially bits of calcium within the optic disc. This may be diagnosed on ultrasonography because it creates a very bright signal which casts a clean shadow (similar to gallstones; image below). Drusen may cause mild visual symptoms, but it's essentially a benign finding.
- Inflammation (generally due to optic neuritis, sarcoidosis, syphilis, or lupus). This is often unilateral, which may help differentiate it from papilledema (which is usually bilateral).
 Integration of optic nerve sheath diameter and papilledema
Integration of optic nerve sheath diameter and papilledema
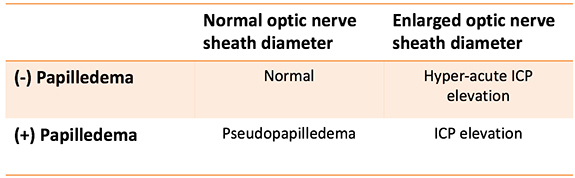
In theory, papilledema and optic nerve sheath diameter could be integrated in a 2×2 table as shown here:
 However, the optic nerve sheath diameter is often not definitively normal or abnormal, which makes this more complex. Overall, optic nerve sheath diameter is supported by the most robust evidence (Shevlin 2015). This leads to the following two-tiered algorithm to determine if the ICP is elevated:
However, the optic nerve sheath diameter is often not definitively normal or abnormal, which makes this more complex. Overall, optic nerve sheath diameter is supported by the most robust evidence (Shevlin 2015). This leads to the following two-tiered algorithm to determine if the ICP is elevated:
 Pretest probability also matters. Within the critical care arena, this test will be applied to patients with significant alteration of consciousness. Among such patients:
Pretest probability also matters. Within the critical care arena, this test will be applied to patients with significant alteration of consciousness. Among such patients:
- There is an above-average rate of ICP elevation.
- There is a relatively low rate of pseudopapilledema.
Thus, the above algorithm might be expected to work reasonably well among critically ill patients. Alternatively, if this algorithm were applied to patients in an ophthalmology clinic, it might misdiagnose some patients with pseudopapilledema as having ICP elevation.
Clinical utility of ICP estimation?
Although this should be obvious, a note of caution is needed here. A normal optic nerve by no means excludes life-threatening brain pathology. If you feel that the patient needs further investigation (e.g. CT, MRI, LP), a normal optic nerve ultrasound shouldn't dissuade you from pursuing that evaluation.
 What, then, is the point of estimating the ICP at all? ICP estimation is merely one more piece of information to be integrated with clinical context. It's not the be-all or end-all, but it may help point us in the right direction. For example, it can be helpful in deciding whether to initiate osmotherapy in a patient with suspected intracranial hypertension who is awaiting neuroimaging.
What, then, is the point of estimating the ICP at all? ICP estimation is merely one more piece of information to be integrated with clinical context. It's not the be-all or end-all, but it may help point us in the right direction. For example, it can be helpful in deciding whether to initiate osmotherapy in a patient with suspected intracranial hypertension who is awaiting neuroimaging.
Returning to the original clinical question
 Recall our case of a patient with optic nerve disc diameter on the higher end of the grey zone (running between 5.5-6 mm). This patient was noted to have ultrasonographic papilledema bilaterally. The combination of a top-normal optic nerve disc diameter and papilledema was highly suggestive of elevated intracranial pressure. Further investigation including CT and MRI scanning ultimately did reveal cerebral edema due to viral encephalitis.
Recall our case of a patient with optic nerve disc diameter on the higher end of the grey zone (running between 5.5-6 mm). This patient was noted to have ultrasonographic papilledema bilaterally. The combination of a top-normal optic nerve disc diameter and papilledema was highly suggestive of elevated intracranial pressure. Further investigation including CT and MRI scanning ultimately did reveal cerebral edema due to viral encephalitis.

- Although papilledema is traditionally considered a finding on opthalmoscopy, it can also be easily observed with point-of-care ultrasonography.
- Sonographic papilledema appears to have good performance for detection of ICP elevation.
- Papilledema can be observed with the same ultrasound views that are used to measure optic nerve sheath diameter, so looking for papilledema requires no additional work.
- Ultrasonographic papilledema may be combined with measurement of the optic nerve sheath diameter to evaluate for elevated intracranial pressure.
Related
- Papilledema and the Crescent sign – Sinai EM Ultrasound
- Optic Nerve Sheath ultrasound for detecting increased ICP – EMCrit
- Optic Nerve Sheath Diameter evaluation – 5 minute sono by Jacob Avila
- Optic nerve sheath diameter: window to the soul? Broome Docs
- Ultrasound for optic nerve sheath diameter – Stephen Alerhand on emDocs
Notes
- Shout-out to Peter Weimersheimer (@VTEMSONO) for creating a monthly EM-ICU ultrasound review conference at UVM. Thanks for organizing this, it's a fantastic conference.
Image credits: gulls on fence,
{kind=link}

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Very interesting! thanks Josh. I have occasionally observed papilloedema on US and been unsure how to integrate it into the clinical picture. This really helps
As always – we must use POCUS in the context of the clinical picture and help guide decision-making rather than rely on it as a binary answer.
Great work
ok, Josh. i have to share this with you and the “team”. i had a long weekend working nights fri-sunday and then monday swing shift, so the last thing i wanted to do on october 10 was read your podcast. (did reward myself monday night with an episode of “24” with sutherland, but tues did this pulmcrit., and did all the links, including the one that scott linked to mass. general. then , on my day shift yesterday: 35 year old female, above avg weight, c/o headaches, dizzy, nausea, progressively worse times 1 year, visual blurring. she said she had… Read more »
Great stuff, thanks for the feedback.
Yeah, transducing pressure from a LP can be a bit tricky. I think in some situations folks may not give it enough time to equilibrate, or the needle may slip out slightly.
“Ophthalmoscopy is arduous and rarely performed in critical care practice.”
For real?! The reason people say this is that it is poorly taught and rarely practiced. It is a phenomenally useful and generally very easy examination to perform to look for papilloedema. I do it all the time.
We need to get out of this defeatist mindset. As a notable contemporary commentator on world events might say: Sad!
I’m just trying to be realistic here. In the US, intensivists very rarely use fundoscopy and aren’t good at it. We could debate whether that is good/bad till we’re blue in the face, but it is reality and unlikely to change in the immediate future.
Fair enough. Look, you’re broadcasting this to the real world and I understand that, but we should be encouraging trainees to learn this skill. It’s extremely useful and genuinely pretty easy if taught well. I am a UK-trained GP, now one of Casey Parker’s colleagues in the ED at Broome Hospital. Occasionally our CT scanner doesn’t work and there isn’t another one for 700 miles.
Sorry. I only put in who I am and where I work when I saw your last post said ‘What’s your job?’ I thought you were asking me the question, but I see it’s in all the posts!
Hello Dr. Farkas, I am writing out of IM residency based in the community hospital in south Brooklyn. US technology her is not a realm of IM department. We are often short staffed and run codes and procedures by ourselves. So being a first year resident I am always afraid of emergency situations on the floor, that is why I read Emcrit and Dr. Malik diligently. Thank you for this particular episode. Over 65 year old female was admitted to GMF after one episode of vomiting and LOC. The was no fever, no cough, but mild WBC. The working diagnosis… Read more »
that’s fantastic, tremendous work!! really glad that you found it useful.
I work in the ED and recently saw a pt with a h/o IIH which had been in remission for several years and the pt had subsequently lost 100+ pounds. She presented with headache and visual symptoms which she described as different and less severe than prior IIH presentation. I wondered how ocular US could have changed our work up. If you were confident in your US and found nerve sheath diameter < 5 and no Papilledema, could you get away with not LP’ing this patient?
Thanks for your thoughts!
Very easy to understand – sharing it with my residents to watch before I do a teaching session for the ocular ultrasound.Thank you