
A recent series of articles suggest that the combination of vancomycin and piperacillin-tazobactam are synergistically nephrotoxic (reviewed by Bryan Hayes here). This is an ongoing topic of debate, pending discussion this week at the Twitter Nephrology Journal Club. It has sparked some interesting articles, including the epic title shown here:
Seriously though, this is an important question: are we hurting our patients with piperacillin-tazobactam? Let's take it one step at a time.
1. Piperacillin-tazobactam increases creatinine levels.
Recent studies have focused on the combination of piperacillin-tazobactam and vancomycin (Maverick and Goose, respectively). However, I doubt that there is anything uniquely nephrotoxic about this exact combination of drugs (1). The real question is whether piperacillin-tazobactam has some weak nephrotoxic properties, which become clinically apparent when combined with vancomycin (a card-carrying nephrotoxin).
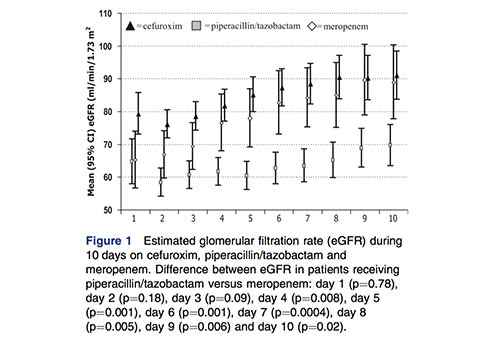
Jensen 2012 might be the best single study to evaluate the effects of piperacillin-tazobactam on renal function. This was a re-analysis of data from a 1200-patient multicenter RCT evaluating the use of procalcitonin. The authors looked carefully at daily creatinine levels while on various antibiotics, and after antibiotic discontinuation. Most patients presented with an acute kidney injury due to sepsis, which improved during the course of treatment. However, patients treated with piperacillin-tazobactam exhibited delayed improvement in their creatinine during antibiotic therapy, compared to patients treated with meropenem (2):
 Following discontinuation of antibiotics, patients in the piperacillin-tazobactam group experienced a rapid improvement in renal function within days. In contrast, patients treated with other antibiotics (including meropenem) had no change in their creatinine after stopping antibiotics:
Following discontinuation of antibiotics, patients in the piperacillin-tazobactam group experienced a rapid improvement in renal function within days. In contrast, patients treated with other antibiotics (including meropenem) had no change in their creatinine after stopping antibiotics:
 Although this is a retrospective study, it is fairly persuasive. Patients in the piperacillin-tazobactam and meropenem groups had similiar baseline renal function. Results were stable upon multivariable re-analysis, arguing against confounding. This result is consistent with most studies which compared vancomycin with or without piperacillin-tazobactam (reviewed here). Overall, it seems that piperacillin-tazobactam increases creatinine levels.
Although this is a retrospective study, it is fairly persuasive. Patients in the piperacillin-tazobactam and meropenem groups had similiar baseline renal function. Results were stable upon multivariable re-analysis, arguing against confounding. This result is consistent with most studies which compared vancomycin with or without piperacillin-tazobactam (reviewed here). Overall, it seems that piperacillin-tazobactam increases creatinine levels.
2. But… piperacillin appears to have nephroprotective effects?
Several animal studies have found that piperacillin exerts nephroprotective effects. Specifically, the addition of piperacillin to nephrotoxic drugs (e.g. amikacin, gentamycin, netilimicin, cisplatin) causes a reduction in renal injury. One study found a similar effect in humans: piperacillin plus amikacin caused less kidney injury than amikacin alone (3).
The mechanism underlying this appears to be as follows: Piperacillin has been shown to competitively inhibit the organic anion transport system, in a fashion similar to probenecid (Komuro 1994, Landersdorfer 2008). Blocking this transporter may reduce the entry of nephrotoxic drugs into the proximal tubules. Lower nephrotoxin concentration in the tubules then shields the kidney from damage (Hayashi 1988, Hayashi 1989).
3. So… piperacillin-tazobactam increases creatinine without hurting the kidneys.
Understanding the effect of piperacillin on the organic anion transport system may allows us to reconcile this seemingly contradictory data:
- Piperacillin-tazobactam may increase serum creatinine due to reduced creatinine secretion via the organic anion transport system. This phenomenon of “pseudo-nephrotoxicity” appears to be a common property of drugs that inhibit this system (e.g. probenecid and trimethoprim; Choudhury 2006)(4).
- However, this elevation in creatinine may not reflect a true reduction in renal function or actual renal damage. In the presence of some nephrotoxins (e.g. aminoglycosides), this might even exert a nephroprotective effect.
Of course, it remains possible that piperacillin-tazobactam is nephrotoxic (e.g. perhaps in rare cases involving acute tubulointerstitial nephritis). Nonetheless, currently there isn't clear evidence that piperacillin-tazobactam commonly exhibits true nephrotoxicity.
4. Hypothesis testing: does piperacillin-tazobactam increase the need for dialysis?
Before finishing up, let's test the concept that piperacillin-tazobactam causes pseudo-nephrotoxicity (elevated in creatinine without genuine renal injury). If this were true, one would expect that piperacillin-tazobactam wouldn't increase the need for dialysis.
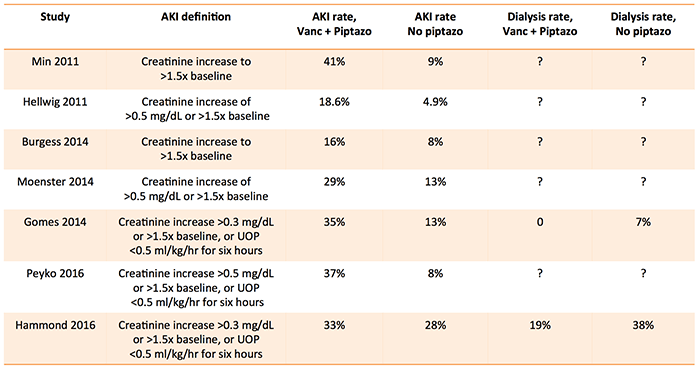 The table above shows recent studies investigating the nephrotoxicity of vancomycin combined with piperacillin-tazobactam (5). Patients treated with piperacillin-tazobactam had higher rates of AKI, but lower rates of requiring dialysis. This dissociation between “AKI” rates and dialysis requirement supports the concept that piperacillin-tazobactam causes an artifactual increase in creatinine only.
The table above shows recent studies investigating the nephrotoxicity of vancomycin combined with piperacillin-tazobactam (5). Patients treated with piperacillin-tazobactam had higher rates of AKI, but lower rates of requiring dialysis. This dissociation between “AKI” rates and dialysis requirement supports the concept that piperacillin-tazobactam causes an artifactual increase in creatinine only.

- Piperacillin-tazobactam may increase serum creatinine due to a reduction in tubular creatinine secretion, caused by inhibition of the organic anion transporter. This causes “pseudo-nephrotoxicity” – increase serum creatinine, without impaired renal function or true renal injury.
- In recent studies, piperacillin-tazobactam is associated with an increased creatinine, but also a trend toward less dialysis. Thus, elevations in creatinine due to piperacillin-tazobactam might not be clinically relevant.
- Current evidence does not support a change in practice due to concerns regarding nephrotoxicity. For now, I will keep on sending in Maverick.
 Stay tuned for more discussion about this topic in a few days at the Nephrology Journal Club. As always, the purpose of this blog isn't necessarily to be right 100% of the time, but rather to explore controversial ideas and stimulate interesting debate.
Stay tuned for more discussion about this topic in a few days at the Nephrology Journal Club. As always, the purpose of this blog isn't necessarily to be right 100% of the time, but rather to explore controversial ideas and stimulate interesting debate.
Related:
- Piperacillin/Tazobactam and risk of acute kidney injury with vancomycin (Bryan Hayes, ALiEM)
- Do CT scans cause contrast nephropathy? (Pulmcrit) This post illustrates how incredibly difficult it can be to determine if something is nephrotoxic.
Notes
- For example, it's hard to think of two drugs which combined are nephrotoxic, but on their own are not nephrotoxic. Most commonly, synergistic nephrotoxicity is due to the combination of two drugs which both have at least some nephrotoxicity on their own.
- Since piperacillin-tazobactam and meropenem were used in a similar fashion for broad-spectrum antibiotic coverage, this is probably the most appropriate comparison. In contrast, patients treated with cefuroxime appeared to be less sick at baseline, which confounds direct comparison.
- Unfortunately this study is in Japanese (Kusafuka 1992). The abstract sounds good, but that's about as far as I can get.
- This explains the rapid fall in serum creatinine observed by Jensen 2012 after piperacillin-tazobactam was stopped (in contrast, when a drug that causes true kidney injury is stopped, it might take the kidneys a bit longer to recover).
- If you don't understand this table, or have questions about these studies, please see the excellent post by Bryan Hayes here.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Thank you, this is very interesting!
Great post, the secretion of SCr via the anion transport system in the proximal tubules and its competitive inhibitors is well known in the Nephrology world and I find this concept of Pseudo-Nephrotoxicity very interesting and becoming more relevant as we diagnose AKI’s. Medicine is in a desperate need for better renal markers. Thanks.
So does it need dose adjustment in aki? For tazosin