 According to Napoleon, “the moment of greatest vulnerability is the instant immediately after victory.” In airway management, this instant occurs immediately after placement of the endotracheal tube. There is a risk of relaxing and overlooking critical details. Meanwhile, this is often the point when the patient's blood pressure and saturation nadir.
According to Napoleon, “the moment of greatest vulnerability is the instant immediately after victory.” In airway management, this instant occurs immediately after placement of the endotracheal tube. There is a risk of relaxing and overlooking critical details. Meanwhile, this is often the point when the patient's blood pressure and saturation nadir.
Introduction with a rare but recurrent error pattern
Imagine that you are intubating a patient with ARDS. You pre-oxygenate the patient and perform a beautiful intubation on the first attempt. Fantastic! You secure the endotracheal tube at 22cm. Unfortunately, your patient is small, so the tube ends up in the right mainstem bronchus. You can't tell. The ICU is noisy, masking any difference in bilateral breath sounds.
The left lung isn't being ventilated, so the patient starts to desaturate. What is your natural response? You bag a bit harder and faster, trying to recruit some atelectatic lung. Unfortunately, all this does is over-distend the right lung, which pops: pneumothorax. With more bagging, this progresses to a tension pneumothorax. Next: hypotension, and maybe cardiac arrest.
Mainstem intubation usually isn’t this catastrophic. However, in a critically ill patient with fragile lungs, it can be. I’ve seen this error pattern several times. The physicians involved in these cases aren’t bad doctors. Rather, this may result from a systemic flaw in our approach to determining endotracheal tube depth.
Myth #1: The endotracheal tube should be placed at 23cm in men and 21cm in women (23/21 rule)
A widely held belief is that the endotracheal tube (ETT) should be secured at 23cm for men and 21cm for women. This is derived from a study of 83 adults in Cincinnati, USA (Roberts 1995).
Dispelling this myth may be accomplished with a simple thought experiment. Imagine two patients requiring intubation. One patient is a five-foot tall man, the other is a six-foot tall woman. According to the 23/21 rule, the man's ETT should be placed deeper than the woman's ETT. Nonsense.
The strongest determinant of ETT depth is height. In multivariable models including height and gender, gender doesn't add any independent information (Varshney 2011). Thus, the 23/21 rule is a crude approximation based on the fact that men, on average, are taller than women. This rule fails in the following situations:
- Anyone with unusual height.
- Patients who aren't Caucasian. The 23/21 rule was developed in the United States, but has failed validation among more diverse populations. Patients of Asian ethnicity have a higher risk of mainstem intubation when using this rule (Ong 1996).
- Transgender patients.
Myth #2: Auscultation will reliably detect right mainstem intubation.
Auscultation is notoriously inaccurate for determining ETT location. For example, auscultation isn't even reliable enough to confirm that the ETT is in the trachea rather than the esophagus. In one series of esophageal intubation cases, almost half documented auscultation of breath sounds (Salem 2001). For this reason, the current standard is to confirm tracheal placement using end-tidal CO2. Given that auscultation isn't accurate enough to determine whether the ETT is in the trachea vs. the esophagus, it is illogical to expect it to detect mainstem intubation.
Sitzwohl 2010 performed a prospective randomized single-blind trial of 160 patients undergoing preoperative intubation, with exclusion of any patients with lung disease. Bronchoscopy was used to precisely position the ETT within the trachea in half of the patients and within the right mainstem bronchus in the other half. Auscultation had a sensitivity for detection of endobronchial intubation of 17/20 (85%) among experienced anesthesiologists versus 9/20 (45%) among first-year residents.
Among critically ill patients, the sensitivity of auscultation is even lower (40% in Brunel 1989). Patients with severe obstructive lung disease or obesity often have quiet lung sounds. In patients with unilateral pneumonia or pleural effusion, comparing lung sounds is meaningless. In the ER or ICU, auscultation is often performed with disposable stethoscopes under noisy conditions.
Better approach: ETT depth based on patient height.
Dozens of studies have searched for an approach to predict the ideal ETT depth. Prediction based on height seems to be supported by the best evidence (1).
Hunyady et al. 2008: Front teeth-to-carina distance in children undergoing cardiac catheterization.
This study investigated 170 children <19 years old who were intubated in Seattle, Washington. The distance between the front teeth to the carina was obtained by adding the depth of the ETT plus the distance between the ETT and carina (measured on the chest X-ray). A strong correlation was noted between height and the distance between the teeth and carina:
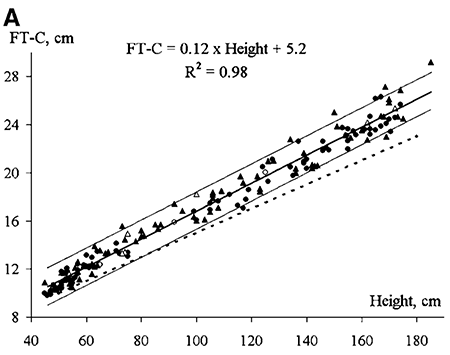 If we want the ETT to be 5 cm above the carina, the following equation could be used (2):
If we want the ETT to be 5 cm above the carina, the following equation could be used (2):
ETT depth = 0.12[height in cm]+0.2
Pak et al. 2010: Assessment of airway length of Korean adults and children for otolaryngology and opthalmic surgery using a fiberoptic bronchoscope.
These authors evaluated 60 adults undergoing elective surgery in Korea (3). After intubation, the distance between the upper incisor and mid-tracheal level was measured using bronchoscopy. The relationship of this distance with patient height is shown here:
 Based on this data, the ideal ETT depth would be given by this equation:
Based on this data, the ideal ETT depth would be given by this equation:
ETT depth = 0.127[height in cm]+0.167
Techanivate et al. 2005: Estimation of the proper length of orotracheal intubation by Chula Formula
ETT depth = 0.1[height in cm] + 4
The Chula formula was developed prior to this study to predict ETT depth (7). These authors prospectively validated the use of this formula among 100 patients in Thailand. Patients were intubated and ETT placed according to the formula. Subsequently, a bronchoscope was used to determine the relationship between the ETT, carina, and vocal cords:
- The distance between the ETT and carina ranged between 1.9-7.5 cm. No patient was at immediate risk of endobronchial intubation (5).
- The upper border of the ETT cuff was always >1.9 cm below the vocal cords, avoiding risk of laryngeal trauma or inadvertent extubation.
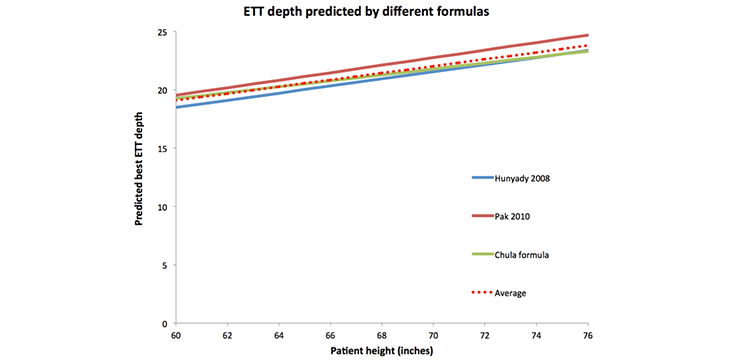
Comparison of various equations
Although these various equations may look different, they actually yield nearly the same results (figure below). For clinical use, I will select the average of all three equations (shown in dotted red below). This is nearly identical to the Chula formula, which has been prospectively validated.
 This isn't anything particularly new. As described in the classic procedure text, Roberts and Hedges:
This isn't anything particularly new. As described in the classic procedure text, Roberts and Hedges:
One can anticipate that tall male patients will often require deeper placement, to 24 or 25 cm, and that short women will often require a shallower placement of 19 or 20 cm –Reardon et al. 2014
Thus, many experts intuitively adjust ETT depth depending on height, over a range of ~19-25 cm. Having a formula may allow this intuitive process to be translated into an objective and reproducible process.
Putting this data into clinical practice
Implementing this equation is easy. The following table shows the ETT depth and target tidal volume, depending on height and gender (4):
 For a non-emergent intubation, the ETT depth and target tidal volume may be determined before intubation and written down (e.g. on a whiteboard in the patient’s room). This will enforce correct ETT position and tidal volumes in the post-intubation period (a busy period where there is a risk of overlooking these details). I scotch taped an airway checklist to my parking card, to prevent it from getting lost:
For a non-emergent intubation, the ETT depth and target tidal volume may be determined before intubation and written down (e.g. on a whiteboard in the patient’s room). This will enforce correct ETT position and tidal volumes in the post-intubation period (a busy period where there is a risk of overlooking these details). I scotch taped an airway checklist to my parking card, to prevent it from getting lost:
Alternative strategies for determining ETT depth.
Like anything in airway management, there are a dizzying number of different approaches. Here are two leading examples.
#1: Direct visualization of ETT depth
 Most ETTs have a black depth marker a few centimeters above the cuff. During intubation, alignment of this with the vocal cords may be used to place the ETT at the correct depth.
Most ETTs have a black depth marker a few centimeters above the cuff. During intubation, alignment of this with the vocal cords may be used to place the ETT at the correct depth.
I haven’t had great results with this technique for a few reasons:
- It relies on the ability to visualize the vocal cords (i.e. Grade I or II view).
- Although this technique is simple, it must be performed during a time then the operator will be rushed, distracted, and adrenergically charged. This is a setup for error.
#2: Balloting the ETT cuff
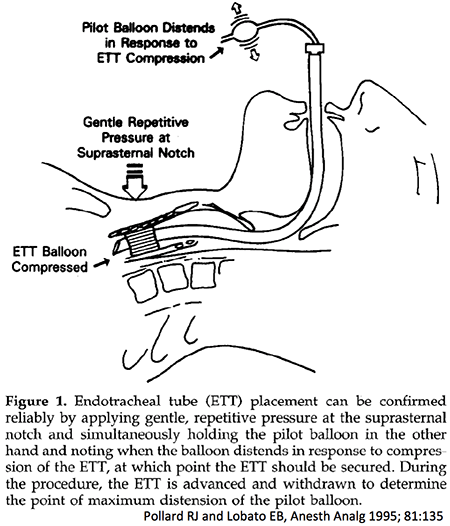 Balloting the ETT cuff refers to exerting gentle bouncing pressure over the suprasternal notch while palpating the ETT pilot balloon. If the ETT is in a good position, pressure variation over the suprasternal notch should be transmitted to the ETT cuff, and thence transmitted further to the pilot balloon (where it may be palpated). If the ETT isn’t easily balloted, this may be used to adjust tube position (e.g. advance or withdraw the ETT until ballottement improves).
Balloting the ETT cuff refers to exerting gentle bouncing pressure over the suprasternal notch while palpating the ETT pilot balloon. If the ETT is in a good position, pressure variation over the suprasternal notch should be transmitted to the ETT cuff, and thence transmitted further to the pilot balloon (where it may be palpated). If the ETT isn’t easily balloted, this may be used to adjust tube position (e.g. advance or withdraw the ETT until ballottement improves).
Unfortunately, inability to ballot the ETT has only a 26% specificity for indicating incorrect ETT placement (Ledrick 2008). Thus, in some cases (e.g. morbid obesity), this technique may incorrectly suggest that the ETT is misplaced. This could lead to repositioning of a correctly positioned ETT, running the risk of actually causing ETT misplacement (6).
Advantages of a height-based strategy compared to these techniques
Many strategies may be successful. There is no direct evidence that any strategy is superior to any other strategy. However, a height-based strategy has some advantages:
- A height-based strategy requires almost no operator effort following intubation. In contrast, ballottement or visualization of the tube marker require active effort after or during laryngoscopy, respectively. Such efforts may distract attention from other peri-intubation events (e.g. blood pressure swings, etc.).
- Ballottement or visualization of the ETT marker requires a certain amount of skill. In contrast, a height-based ETT depth algorithm can be uniformly implemented without any learning curve.
- Use of a height-based strategy encourages the use of safe tidal volumes, because both ETT depth and tidal volume may be determined simultaneously.

- Although ETT depth is generally overlooked, it can be important. Inadvertent endobronchial intubation exposes the patient to a risk of hypoxemia, atelectasis, and pneumothorax.
- Our usual strategy for determining ETT depth is error-prone:
- (a) Traditionally it has been taught that ETT depth should be 23 cm in men and 21 cm in women. This rule may be dangerous in people of unusual height or non-Caucasian ethnicity.
- (b) Chest auscultation is insensitive for detecting endobronchial intubation.
- ETT depth may be predicted based on the patient’s height. This has been validated among both men and women, across different ethnicities, and among both adults and taller children.
- A height-based algorithm can easily be implemented by attaching a table to determine ETT depth and tidal volume to your airway checklist (example below). This table may simultaneously improve two aspects of post-intubation safety.
Related
- RSI Checklist (EMCrit)
Notes
- Newer studies are discussed in this blog, but there are some older studies which came to nearly identical conclusions (Eagle 1992, Morgan 1982).
- This 5 cm figure is a bit fuzzy. Different sources make different recommendations about how far above the carina the ETT should be (e.g. 3-5 cm, 3-6 cm, 5-7 cm). 5 cm seems to be in the middle of these (somewhat discordant) recommendations.
- They also studied children, but for the purposes of this blog I’m only focusing on their findings with regards to adults.
- This is my airway checklist. I make no claim that this is the best airway checklist, but rather that it works within my context. For example, some things are so engrained in my practice that I've left them off the checklist. For more on airway checklists see: RSI Checklist.
- In one patient the distance from the carina was <2cm, which is potentially dangerous (if the patient was to flex their neck, the tube could advance further). However, in all cases the ETT position was safe enough for a short period of ventilation, until the chest x-ray was obtained.
- I know some anesthesiologists who swear by this technique. I have no doubt that this works extremely well in the hands of someone with substantial experience with it. However, in terms of creating a uniform approach to airway management which is highly reproducible and failure-resistant, this technique doesn't seem like the best approach.
- Interestingly, other investigators have also proposed that the exact formula should be used for infants below three months of age. This may speak to the universality of these relationships.
Image credits: Napoleon
{kind=link}

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
why not just throw the ultrasound on the left chest to make sure there is lung slide?
why not do both?
Ultrasound is great, especially if there is question of right mainstem intubation (although performance isn’t perfect: https://www.ncbi.nlm.nih.gov/pubmed/16495415; https://www.ncbi.nlm.nih.gov/pubmed/26950708). Also ultrasound doesn’t exclude incipient right mainstem intubation (e.g. the ETT is a few milimeters from the right mainstem, may slip into it if the patient is moved, but not quite there yet). My main reason for not using an ultrasound-based algorithm is that most of the time I don’t have an ultrasound in the room when intubating. (You could argue that I should, but the current reality is that most intubations occur without an ultrasound). So a height-based algorithm is easier… Read more »
Hi Dr, good information. When I worked in a SEA country where most population short built, I put ETT at depth of 18 sometimes and good position confirmed later with xray. In fact I never gone beyond 22cm. My mind did not agree to follow standard rule of 21 to 23.
Hi Dr Josh, how if we measure length from Manubroihm Sterni to incisors externally to estimate correct depth of ETT.
What if you are intubating for complete left lung collapse .
In this situation ultrasound and auscultation are totally not helpful.
As mentioned the problems will come from exposing the right lung to more pressures.
Hello Josh, good article! I have to be agree with you. There are many errors specially when there is no expertise. There are some details that I like to know your thoughts. 1. Some formula for ett depth calc for pediatrics are based on age or weight, not “height”. Like you said height is variable among person. 2. The other thing is patient’s body position. If the ett is placed too deep, and the patient is in trendelenburg there is higher risk for endobronchial intubation. Or vice versa ett placed too superficial and the patient’s neck is extended there us… Read more »
This smacks of more numbers to forget during a stressful situation. Esp w SaO2 lag w peripheral oximetry after successful intubation, its cognitively important to visualize the ETT passing through the cords. For me this means slowing down as the tube enters the cords, watching the balloon pass – 1-2 cm past the cords, and then briefly pausing to take that mental picture of a successful intubation for the inevitable angst when SaO2 transiently continues to drop in a sick patient. Tube may be a cm or so higher then desired, but can always be advanced after confirmatory imaging.
I’ve tried this, and I’ve tried to teach my fellows it. It’s not as easy as it sounds, and frankly I was unable to achieve consistent results with this when applying it with different fellows and residents. Especially with regards to improving institution-wide quality, direct visualization has many limitations: (1) Only works if you have an excellent view of the cords and maintain this view throughout the procedure. (2) Technique has to be taught to every trainee, this makes it difficult to implement across the board in any consistent fashion. (3) Increases task-complexity of intubation & distracts the operator after… Read more »
I may have totally missed this, but is the ETT depth from the lip, teeth, or other location?
Distance is measured from the upper front teeth (not the molars).
Interesting article. Thanks Josh for putting light on the issue with right stem intubation. Good as it is to have this formula to get an idea of a reasonable depth, I still have to agree with Peter W; See the tube pass the cords, stop by the black marker (which is there in all ETT brands I´ve used). Most patients are grade II, especially if you have access to VL at least as a backup, so rt stem intub is very seldom an issue for adults (peds more relevant) in my experience. In the few patients where one is super… Read more »
With regards to the drawbacks of direct visualization, see my comment above to Peter’s thoughts. You sound like an expert who has essentially internalized a height calculation. I think that this is very common, and probably the way most expert intubators determine ETT depth. The formula is essentially doing the same thing, just in a more reproducible fashion and without the need for so much experience. The advantage of the formula is that anyone could pick it up and use it, and presumably achieve the same results as an expert. There are certainly many ways to do this and probably… Read more »
I can certainly see the point in uniform routines and specifically in a big shop with a big throughput of, particularly junior, doctors. Obviously to get a good view, incl cuff/marker passing the cords, should be part of every intubator’s training and skill set. But I do appreciate that where I work Anaesthetists are the only one´s intubating anywhere and that obviously makes for a difference compared to where you have a greater mix in background and experience of the intubators. I still think it´s really difficult to estimate height of patients in a bed apart form a rough short,… Read more »
Great post, and great checklist! You should put EtCO2 on the checklist as well, important to prepare that
Hi Josh,
I revisited this post after listening to a lecture from an ENT attending discussing endotracheal tube diameter selection in the ICU. He mentioned using patient height not only to select ETT depth but also diameter. In that very tall people should get large diameter tubes, and shorter patients the smaller diameter tubes. Does this jive with your practice as well?
Excellent previous points! Provided you can get grade 2B view (or better) and intubate with a GlideScope or equivalent; I generally just leave the blade in the mouth after a successful intubation and watch the ETT cuff on the screen inflate just distal to the cords. I hold little weight to auscultation and rely on an ETCO2 (preferably with a waveform) until I get confirmation with CXR or US (with a reliable operator).
Excellent previous points! Provided you can get grade 2B view (or better) and intubate with a GlideScope or equivalent; I generally just leave the blade in the mouth after a successful intubation and watch the ETT cuff on the screen inflate just distal to the cords. I hold little weight to auscultation and rely on an ETCO2 (preferably with a waveform) until I get confirmation with CXR or US (with a reliable operator).