

CONTENTS
- Rapid Reference 🚀
- Is CAUTI real?
- Diagnostic criteria for CAUTI
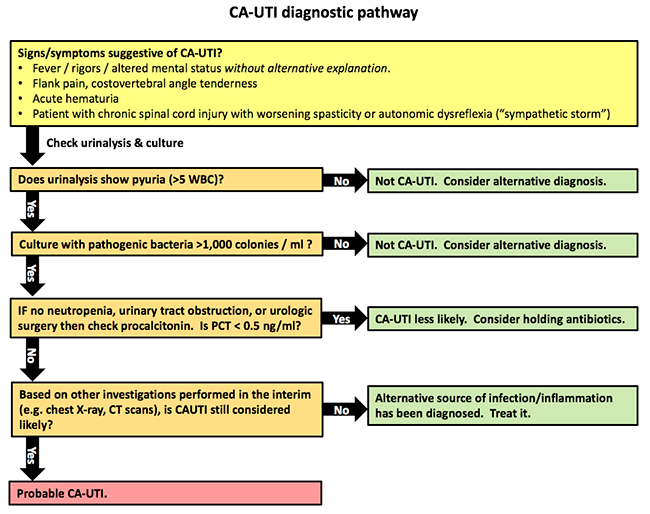
- Diagnosis of CAUTI
- Treatment of CAUTI
- Prevention
- Podcast
- Questions & discussion
- Pitfalls
some general principles
- Urinary tract infections may be divided into infections limited to the bladder and urethra (cystitis) and infections which ascend to involve the kidneys (pyelonephritis).
- Cystitis may cause local symptoms (e.g., frequency, dysuria), but rarely causes systemic symptoms (e.g., fever, septic shock).
- Pyelonephritis is a common cause of bacteremia and septic shock.
- Over time, most patients with a urinary catheter will develop bacterial colonization of their bladders. This is also commonly seen in normal elderly people as well, even without having urinary catheters (asymptomatic bacteriuria).
- This colonization is generally noninvasive and limited to the bladder, rather than ascending to the kidneys (unless there is obstruction, urologic surgery, or neutropenia). The Foley catheter itself plus ongoing urine flow tends to prevent invasive infection. However, some patients may develop invasive infection after the Foley catheter is removed, if there is subsequent urinary stasis and reflux into the kidneys.
- Catheter associated-urinary tract infection (CAUTI) is generally over-diagnosed, because the urine is easily cultured and often yields bacteria. In reality, these bacteria are usually not causing disease.
- Finding bacteria in the urine is easy; the challenging issue is determining whether they are causing disease.
is CAUTI even real?
- CAUTI probably does exist, but it is vastly less common than usually believed.
- One study prospectively evaluated 1,034 hospitalized patients with new Foley catheters and no alternative focus of infection. 89 patients (9%) developed >1,000 bacteria/ml in their urine. However, comparing patients who developed bacteriuria versus those who did not, there was no difference in the frequency of urgency, dysuria, fever, or leukocytosis! Thus, the vast majority of patients who develop bacteriuria have asymptomatic bacteriuria.(10724054)
- There is a notable absence of evidence that either of the following statements is valid:
- CAUTI commonly causes symptoms (or necessarily exists, among patients with a functional Foley catheter).
- Treatment of bacteriuria in hospitalized patients with an indwelling Foley catheter is beneficial.
The Infectious Disease Society of America (IDSA) definition of CAUTI requires all of the following components: (20175247)
- (1) Culture growth of at least 1,000 colony-forming units per ml of a uropathological bacteria.
- Note: candiduria doesn't qualify for the diagnosis of CAUTI. (29910547)
- (2) Symptoms or signs of a urinary tract infection (e.g., fever, costovertebral angle tenderness, hypotension).
- (3) No alternative explanation of these symptoms, despite adequate evaluation.
- (4) Patient is catheterized or has had a urinary catheter removed within <48 hours.
key points regarding the definition of CAUTI
- CAUTI is a definition of exclusion.
- Positive urinary culture by itself does not indicate CAUTI (and most often such patients won't have a CAUTI).
symptoms of CAUTI can be tricky
- Fever or mental status changes:
- Overall, for patients in the ICU, CAUTI is rarely a cause of these symptoms.(23878765)
- Evaluation for CAUTI may be reasonable if there are no alternative explanations. However, don't assume that the combination of a fever and positive urinalysis means that there is a CAUTI.
- Bladder irritation (e.g., frequency, dysuria, urgency)
- For a patient with a urinary catheter, these are nonspecific (because they can be caused by direct irritation from the catheter).
- For a patient whose catheter has been removed, these symptoms should be considered as potential symptoms of infection.
bladder ultrasonography
- This might be the single most important investigation to perform in a patient with possible CAUTI.
- (1) The finding of a distended bladder indicates dysfunction of the Foley catheter. This indicates a real risk of cystitis, pyelonephritis, septic shock, and obstructive renal failure. Urinary obstruction is an emergent problem which requires immediate attention (e.g., flushing or replacement of the foley catheter).
- (2) A non-distended bladder indicates normal function of the Foley catheter. In the context of a patient without neutropenia, this makes invasive bacterial infection distinctly unlikely.
urinalysis
- Bacterial culture
- Over time, most urinary catheters will become colonized with bacteria (asymptomatic bacteriuria). This occurs at a rate of 3-10% per day, so nearly all patients catheterized for a month will have bacteriuria. (30241712)
- The presence of bacteria doesn't necessarily indicate CAUTI.
- >1,000 bacteria/ml is recommended as a level that may be considered positive by the Infectious Disease Society of America guideline. However, most patients with CAUTI will have >100,000 bacteria/ml (and this higher cutoff is used by the Centers for Disease Control definition of CAUTI).
- Over time, most urinary catheters will become colonized with bacteria (asymptomatic bacteriuria). This occurs at a rate of 3-10% per day, so nearly all patients catheterized for a month will have bacteriuria. (30241712)
- Pyuria (>10 WBC/uL)
- The presence of pyuria is nonspecific: this can be caused by CAUTI or by sterile irritation of the bladder by the urinary catheter.
- The absence of pyuria argues against a diagnosis of CAUTI (unless the patient is neutropenic).

procalcitonin
- The role of procalcitonin in UTI requires further research. However, it does appear that procalcitonin >0.5 is sensitive for the detection of urinary tract infection with bacteremia.(27979420, 25944771)
- For patients in whom the clinical suspicion is low for CAUTI (e.g., no neutropenia, obstruction, or urologic surgery), a procalcitonin <0.5 ng/ml may support the decision to withhold antibiotics.

when to start antibiotics?
- It is unclear exactly when antibiotics should be started during the diagnostic evaluation for CAUTI.
- For patients with clinical signs of septic shock or neutropenic fever, antibiotic initiation should not be delayed.
- For patients with an isolated fever, antibiotics should generally be withheld pending additional investigation (fever isn't an indication for antibiotics!).
selection of antibiotics
- Epidemiological studies of CAUTI show that most infections are caused by gram-negative bacilli (~20% overall due to Pseudomonas), with occasional infections due to Staphylococcus aureus or Enterococcus species.
- How broad does initial coverage need to be?
- This is unclear.
- If the patient is stable (e.g., febrile but not shocked), then it's not mission-critical to cover all possible organisms initially. For example, it's probably unnecessary to cover enterococcus in most patients (given that enterococcus is uncommon and not a very virulent organism anyway).
- Potential empiric regimens?
- Piperacillin-tazobactam is a reasonable initial agent for sicker patients, given coverage of Pseudomonas and Enterococcus.
- Ceftazidime might be a reasonable cephalosporin choice (with a goal of covering pseudomonas, while accepting sub-par gram-positive coverage).
- Aztreonam could be a logical choice and a somewhat elegant choice as well (good gram-negative coverage, without affecting gram-positive flora).
- Culture and sensitivity information should almost always be available within 48-72 hours. This should allow for narrowing and focusing of antibiotic therapy.
duration of antibiotics
- Recommendations range from 3-14 days. With ongoing trends towards shorter antibiotics courses in the ICU, 3-7 days is probably reasonable for most patients.
changing the Foley catheter
- This should be done upon initiation of antibiotics.
- Foley catheters will develop a biofilm, which harbors bacteria and is difficult for antibiotics to penetrate. This is the same biofilm phenomenon which explains why an infected central line should be removed.
avoid or limit Foley catheter placement
- Review the need for a Foley catheter daily (similarly to ongoing review for a central line).
alternatives to bladder catheterization?
- These include a condom catheter for men or an external female collection device for women (e.g., PureWick).
- Although intuitively these devices might seem safer, they are not supported by robust data among ICU patients. Especially for women, these devices should not be assumed to be superior to a Foley catheter.

Follow us on iTunes
The Podcast Episode
Want to Download the Episode?
Right Click Here and Choose Save-As
To keep this page small and fast, questions & discussion about this post can be found on another page here.

- Urinalysis should not be checked simply due to cloudy or odorous urine (Class A recommendation from Infectious Diseases Society of America). This probably represents colonization of the Foley bag, not invasive infection.
- Be careful about blaming fever and sepsis on CAUTI. CAUTI is a rare cause of severe illness, so it's probable that something else is going on (e.g., ventilator-associated pneumonia or line infection). Prematurely anchoring on the diagnosis of CAUTI could cause another focus of infection to be overlooked.
- Lower urinary tract symptoms (e.g., frequency, dysuria) may be due to irritation of the bladder by the catheter itself, rendering them nonspecific and unhelpful.
Guide to emoji hyperlinks 
 = Link to online calculator.
= Link to online calculator. = Link to Medscape monograph about a drug.
= Link to Medscape monograph about a drug. = Link to IBCC section about a drug.
= Link to IBCC section about a drug. = Link to IBCC section covering that topic.
= Link to IBCC section covering that topic. = Link to FOAMed site with related information.
= Link to FOAMed site with related information. = Link to supplemental media.
= Link to supplemental media.
References
- 10724054 Tambyah PA, Maki DG. Catheter-associated urinary tract infection is rarely symptomatic: a prospective study of 1,497 catheterized patients. Arch Intern Med. 2000;160(5):678-682. doi:10.1001/archinte.160.5.678 [PubMed]
- 20175247 Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(5):625-663. doi:10.1086/650482 [PubMed]
- 23878765 Cunha BA. Clinical approach to fever in the neurosurgical intensive care unit: Focus on drug fever. Surg Neurol Int. 2013;4(Suppl 5):S318-S322. Published 2013 May 6. doi:10.4103/2152-7806.111432 [PubMed]
- 24479059 Al Montasir A, Al Mustaque A. Purple urine bag syndrome. J Family Med Prim Care. 2013;2(1):104-105. doi:10.4103/2249-4863.109970 [PubMed]
- 25944771 Julián-Jiménez A, Gutiérrez-Martín P, Lizcano-Lizcano A, López-Guerrero MA, Barroso-Manso Á, Heredero-Gálvez E. Usefulness of procalcitonin and C-reactive protein for predicting bacteremia in urinary tract infections in the emergency department. Actas Urol Esp. 2015;39(8):502-510. doi:10.1016/j.acuro.2015.03.003 [PubMed]
- 27979420 Yan ST, Sun LC, Jia HB, Gao W, Yang JP, Zhang GQ. Procalcitonin levels in bloodstream infections caused by different sources and species of bacteria. Am J Emerg Med. 2017;35(4):579-583. doi:10.1016/j.ajem.2016.12.017 [PubMed]
- 29910547 Saran S, Rao NS, Azim A. Diagnosing Catheter-associated Urinary Tract Infection in Critically Ill Patients: Do the Guidelines Help?. Indian J Crit Care Med. 2018;22(5):357-360. doi:10.4103/ijccm.IJCCM_434_17 [PubMed]
- 30241712 Shuman EK, Chenoweth CE. Urinary Catheter-Associated Infections. Infect Dis Clin North Am. 2018;32(4):885-897. doi:10.1016/j.idc.2018.07.002 [PubMed]

{kind=link}