
Today I get to talk Status Epilepticus with Tom Bleck.
Tom Bleck is a neurointensivist from Rush Medical College in Chicago, where he is a professor of neurological sciences, neurosurgery, medicine, and anesthesiology. Dr. Bleck is board certified in internal medicine, with subspecialty certification in critical care medicine; neurology, with subspecialty certification in vascular neurology; clinical neurophysiology; and neurocritical care. He was the founding president of the Neurocritical Care Society.
Here are the questions we discussed:
Initial Treatment
RAMPART [21967361] showed us that 10 mg IM Midazolam was at least as good as 4 mg IV Lorazepam
If we have an IV, why are we not using IV midazolam over IV Lorazepam?
When is Status Refractory?
- “Status should be considered refractory after the failure of the first agent that should have worked”
- “If you fail lorazepam, you should move to general anesthesia”
- “The longer you seize, the tougher it will be to break”
When should you say that the seizure is unlikely to end? At 5 minutes, you have an 80% or greater chance that you will continue seizing
See Josh Farkas' view on the rapid sequence termination
So if they fail lorazepam (midazolam?), we should consider intubation and general anesthesia.
Which Paralytic?
Sux vs. Roc
Which agent is best for General Anesthesia?
High Dose Midazolam (Neurology 2014;82:359)
– loading dose: 0.2 mg/kg
– maintenance: 0.1 - 2.0 mg/kg/hr
Propofol
may be bad (Prasad A et al Epilepsia 2001;?42:380-386)
Conventional AEDs
Which one and when?
- Fosphenytoin
- Valproic Acid
- Levetiracetam (Keppra)
- Lacosamide
Dr. Bleck recommends one of the latter two. Levetiracetam at a dose of 1 gm, may repeat 1-2 times or Lacosamide 200-300 mg.
Still Refractory
- Ketamine for Status [cite source='pubmed']23758557[/cite] and this article. Reasonable Starting Dose 3-5 mg/kg.
- Hypothermia
- Inhaled General Anesthesia-AnaConDa with Iso or Desflurane
- This Review Article Discusses Super-Refractory Status Management
EEGs
When should a patient get continuous EEGs?
What if you don't have access
EEG Interpretation for Dummies
- EEG should be the opposite of your EKG (Vfib is good)
- Reactive is better than non-reactive
What if we can't get one?
NitWitticism: Being in burst suppression will prevent you from seizing. Pts can seize through burst. May need to be made flatline EEG.
Etiology
Consider Autoimmune Encephalitis, especially Anti-NMDA Encephalitis (Neurology 2015 vol. 85 no. 18 1604-1613)
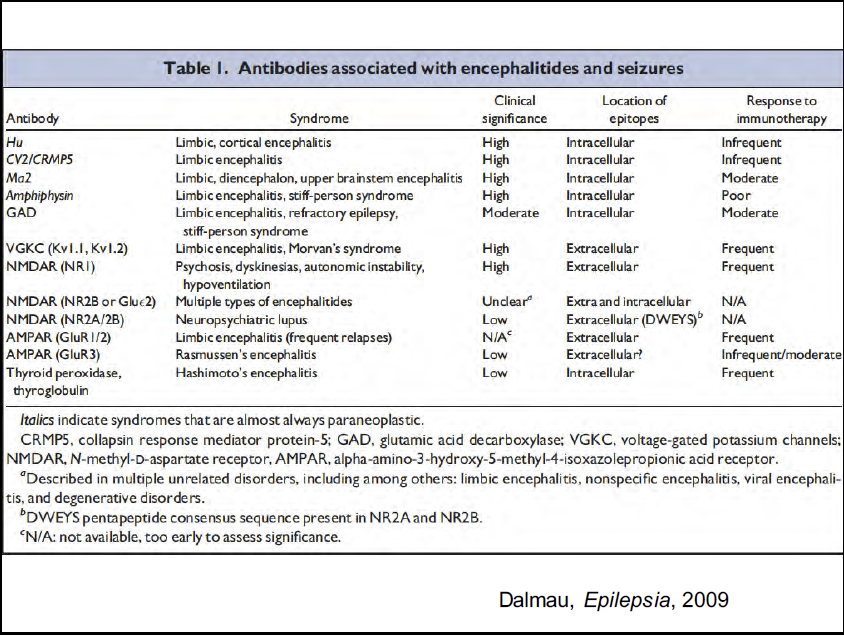{kind=link}
Consider Tox
- INH
- Tricyclics
- Theophylline
- Cocaine
- Alcohol/Benzo withdrawal
- Organophosphates
More from Tom on Status
- Rossetti and Bleck in ICM
- Tom Bleck's Slides from SMACC on SE
- Tom's Lecture on Free Emerg Med Talks
- Medscape Article
Articles and Guidelines of Interest
- Neurocritical Care Society Guidelines
Additional New Information
More on EMCrit
Status Epilepticus(Opens in a new browser tab)
The Status on Status(Opens in a new browser tab)
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Hi Scott,
With regard to muscle relaxants would the use of sugammadex to reverse the rocuronium after intubation be an option in these cases if you want to avoid suxamethonium?
Definitely, Alice. Although I would think a lot of places don’t have this stocked and it’s still somewhat expensive. HIgh dose opioid would also facilitate good airway conditions if (as is typical) high sympathetic burst and CV healthy. 4micr/kg of remi one option together with propofol (itself good for aw tone relaxation) usually facilitate good aw and has fast onset. But nothing beats NMBs for good fast control, especially if aspiration a risk.
Best regards, Mads, gasman, DK.
Agree with both of you. One other non-studied option is a slug of prop and a slug of ketamine. I can’t imagine you would have too many folks you couldn’t intubate. And have the sux or roc drawn up in reserve.
Another review article
http://brain.oxfordjournals.org/content/134/10/2802
Hi Scott, u got some amazing stuff here and I applaud and thank you for it.
My question stemming from old swedish traditions: No room for thiopental in genereal anaestheisa anymore?
Tom mentioned it briefly, but it doesn’t exist in the US
Hi Scott,
Thank you for hosting such a quality discussion. From a paramedic point of view I think more can be done prehospital for these patients. Early treatment may prevent seizures from becoming self sustaining and as you discussed no pre hospital treatment was associated with increased rates of intubation. Probably not anaesthesia but certainly the administration of agents like Keppra I think is achievable by paramedics.
Do you treat convulsant status epilepticus differently to non convulsant status epilepticus?
Very interesting podcast and also relevant to prehospital providers. If you are caring for a patient who has seizures or developers them, why not intranasal Midazolam? It would be absorbed quicker than waiting for an IV or IM use.
do the study and then we will : )
SCOTT!!!! thanks so much for doing this podcast. OMG I am so glad you put this together with such a wonderful expert on the subject. This was so on point. You also asked him one of the most important questions in my opinion. What to do if you do not have cont, EEG ability. This scenario plagues me to no end. Using the appropriate drugs is second nature for me in the ICU. Dr. Bleck’s perspective is a great listen. My biggest hurdle from a logistics side in the these patients is getting the cont EEG. Of the 20 hospitals… Read more »
Hey Scott,
Great show, some fantastic information in that action packed 25 minutes! The one comment I would add is that when progressing to general anesthesia for status (especially in adults without a know seizure disorder history) we should probably also be considering 5 grams of pyridoxine as well. This would be especially important at practice sites that encounter large populations of HIV-positive patients, immigrants, prisoners, or IVDU. The incidence of TB amongst these populations remains much higher than the general population and encountering INH induced status should be on the clinician’s radar.
Willie
added a tox section to the shownotes, great point
Scott, This podcast was a huge treat! Bleck is an icon in NCC and one of founders of the field. Great interview! I’d like to throw out one other option for induction during RSI for the RSE patient: 0.2 mg/kg of MDZ. This would not only be your induction drug, but it would be your initial MDZ load for your cIV gtt. As you mentioned in the podcast, hypotension is a possibility, and should be mitigated/ anticipated. Also, a few words on KET and RSE. I fear that your listeners may get the idea that RSE is being treated with… Read more »
yep! absolutely crucial that ketamine is not given as a substitute to GABAergic meds. Thanks for the refs, Chris!
Hi Scott!
Thanks for this superb podcast!
Just a few quick questions… For General Anesthesia, you have mentioned the maintenance dose for Midazolam is upto 2mg/kg/hr..
(1) Now isn’t that too high a dose?
(2)Do we, after reaching a limit, add another agent so as not to go this far with Midaz?
(3)If so, what do we use?
Thanks
there is no dose too high until hypotension intervenes or the pt’s eeg is flatline. if you need a ref, go to the NCS guidelines linked above. If you still have seizure activity, I think I would move to the super-refractory therapies listed above.
Great podcast- I would still rather use roc than suxs so I’m curious about this approach. I can’t seem to find the post now but Reuben Strayer suggested a while back that you can still use Roc in status but you could do a finger tourniquet on a seizing extremity before you pushed the roc to cut off blood flow temporarily. This should allow you to tell if the patient was still seizing after the roc since the roc won’t make it into that finger. I imagine you could also try to use a manual BP cuff on the forearm… Read more »
i think this is a convoluted solution to a non-existent problem for a patient without sux contraindications. For those who have contraindications; you can give it a shot. Problem is you have no confirmation of whether you have successfully left the arm’s receptors unaffected vs. the pt’s arm is actually paralyzed and they are still seizing.
Hey Scott, nice podcast. Anecdotally have used ketamine IV in patients with SE while slower drugs infusing (e.g phenytoin) and have avoided a GA. Also recently started using valproate as 2nd line, over 5min.
With all do respect to the speaker. When I absolutely positively want someone to stop seizing now!. I reach for the Phenobarbital. In Thirty years of practice it has rarely failed me. Why is phenobarbital a bad thing. It is cheap and I have found it effective…Further in seizures related to GABA receptor down regulation it works on the alpha, beta and gamma subunits.
could Status epileptics be focal? if yes should it be treated the same as generalized tonic colonic SE?
thanks.. if i decided to intubate with midazolam,, is it still necessary to add fentanyl for example.. ?? then should i continue fentanyl infusion?