 We've discussed REBOA before on the EMCrit Podcast with Megan Brenner. We also featured the first prehospital REBOA case. It was an interesting treatment, but an extremely complex one. That has all changed with the new ER REBOA catheter.
We've discussed REBOA before on the EMCrit Podcast with Megan Brenner. We also featured the first prehospital REBOA case. It was an interesting treatment, but an extremely complex one. That has all changed with the new ER REBOA catheter.
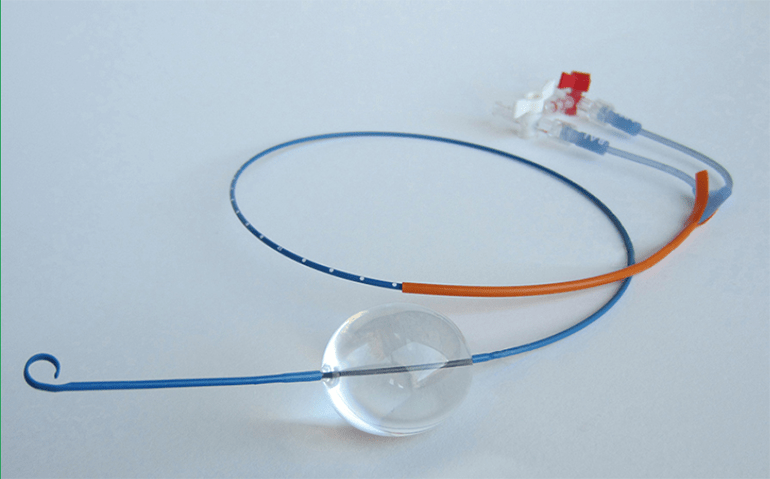
In this podcast, I discuss the new catheter from Prytime and then I interview Dr. Joe DuBose, a trauma and vascular surgeon who performed the first ER REBOA placement that resulted in a survivor.
Conflicts of Interest
Neither Dr. DuBose nor I have any conflicts of interest regarding the ER REBOA catheter or otherwise
Slides from Dr. DuBose's Case
ER REBOA Visual Tour
ER REBOA Placement Video
Steps to Placement of the ER REBOA Catheter
Gain Access to the Common Femoral Artery with a 7-French Introducer
- Just like normal for an arterial line, except make sure you are hitting common femoral and not superficial femoral artery. The point of entry should be 2 cm below inguinal ligament (estimate ligament by anterior superior iliac to pubic tubercle). This may be much higher than you are used to.
- Only some introducers will work:


Attach a Syringe to the Balloon Port of the REBOA Catheter
- Use a 25 or 30 ml syringe, filled with 24 ml of NS
Test the Balloon
- Inflate to test patency
- Make sure to fully deflate the balloon. Apply some extra suction to really shrink it down and then lock the balloon stopcock
Attach Transducer
- Attach a pressure transducer to the arterial line port. Zero the transducer to the phlebostatic access
Measure externally
- Zone 1 is measured with the proximal edge of the balloon at the xiphoid, Zone 3 is measured with the proximal edge of the balloon just above the umbilicus.


Insert the REBOA Catheter
- Use the orange sheath to straighten the p-tip
- Insert the orange sheath 1cm into the valve of the 7-french introducer
- Advance the REBOA catheter a few cm into the introducer
- Pull back on the orange sheath
- Advance the REBOA catheter to the predetermined depth
Inflate the Balloon
- Hold the REBOA catheter to prevent it from pushing out
- Open the Stopcock
- Inflate until resistance goes to moderate or the blood pressure on the arterial line tracing of the REBOA Catheter starts to increase. In general, this corresponds to 12-22 mls depending on the size of the aorta–but this must be individualized to the patient. The actual inflation is far harder than you may think. For me, it is the maximal force I can apply with 1 hand.
- Never instill more than 24 mls. Never more than 24
- Close the stopcock
Secure the Catheter
- If the catheter is not secured externally it will migrate out from aortic pressure, especially in zone I
- It will be an institution dependent choice as to how to secure: tape, sutures, the wings from a 7-french triple lumen, etc.

Get an Xray when time allows
Go to Definitive Management
- When deflating the balloon for removal, it will require active suction to cause deflation. Make sure the number of mls recorded as being used for inflation are removed. If the catheter catches on the introducer sheath during removal, reinsert a few cm. Gently inflate with a few mls and then remove all saline again and maintain suction while locking the stopcock.
- The introducer sheath removal likely will not need cutdown or arterial repair. However, patients are still at risk for vascular trauma or vasospasm.
- Schedule neurovascular checks and consider angiographic imaging.
Even More Stuff
- In a delightful bit of synchronicity, my main man Rob Orman, published a REBOA podcast yesterday with Zaf
- Zaf's REBOA Review Article
- Deb Stein on REBOA from SmaccCHICAGO
- History of REBOA (J Trauma Acute Care Surg 79(4-supp 1):S236
- REBOA Case Series
- Trauma Registry Study (Journal of Trauma and Acute Care Surgery:October 2015 – Volume 79 – Issue 4 – p 523–532)
- Ultrasound Wire Confirmation (Journal of Trauma and Acute Care Surgery October 2015 – Volume 79 – Issue 4 – p 549–554)
- Ultrasonography technique for Zone III (J Trauma Acute Care Surg 2016;80: 89)
- Resuscitative endovascular balloon occlusion of the aorta for uncontrolled haemorrahgic shock as an adjunct to haemostatic procedures in the acute care setting
- A cadaver study indicates mid-sternum may be a better landmark (Journal of Trauma and Acute Care Surgery:
September 2016 – Volume 81 – Issue 3 – p 453–457)
- A micro-bubble ultrasound contrast agent may further augment the ultrasound visualization (DOI: 10.1097/TA.0000000000000863)
- First study of ER-REBOA in combat. placed by non-surgeons (PMID: 28285473)
Additional New Information
More on EMCrit
REBOA for Non-Traumatic (Medical) Cardiac Arrest
EMCrit Guest Post – The good, the bad, and the ugly of the Joint Statement on REBOA by Zaffer Qasim
EMCrit Podcast 133 – The First Prehospital REBOA
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Thanks for the mention Scott! I had a couple of thoughts your readers might find of interest based on my practice: 1. Accessing the artery – I think definitely using ultrasound is the way to go primarily, as identifying and accessing the common femoral is critical to minimize the risk of vascular injury. Blind puncture is often done too low as you mention into the superficial femoral especially in larger patients we may encounter. Additionally, I think even with this catheter there is still value in placing a standard arterial line first, and putting it in early in someone you… Read more »
Other than the Reanimateconference, any local BEST conferences for ecmo/reboa training?
Any thoughts on a east coast conference teaching such procedures like at Stony Brook?
–Torres
An emergency medicine physician who teaches simulation and airway.
We were thinking of coming out East, but logistically it will never happen. Just too much stuff and too perfect a location in San Diego.
If you want just REBOA, Shock Trauma has their BEST Course.
Congrates for a great case by DuBose et al. They did a great work. The REBOA and other endo/hybrid methods are spreading fast. We have in Europe the EVTM workshops, trauma workshops (using also ER REBOA wich was great to use in models and animals!) and next year, Feb 2017, the first EndoVascular and Hybrid Trauma and bleeding Management (EVTM round tables). For more details, http://www.jevtm.com under sympsoium. We hope that in this meeting we can discuss the ER REBOA and other methods for bleeding control. We would like to congratulate the company for comming up with this catheter- this… Read more »
If manual pressure is impractical, or clotting is likely to be impaired, removal lesions of up to 8 Fr can be closed with an Angio-Seal closure system – as is the standard in interventional cardiology.
Cheers!
Patrick
Germany
[…] Here is Joes previous interview by Scott Weingart on EMCrit […]