
So…
I spent the afternoon wading through the proposed CMS sepsis measure. Anyone who has any experience with national quality measures understands just how painful a way this is to waste a few hours. Here is the issue:
You and I have a pretty clean definition of Severe Sepsis and Septic Shock:
- A suspected infection
- with >=2 of the SIRS criteria
- along with a Lactate >=4 mmol/L or hypotension (SBP<90, MAP<65) after initial fluid resuscitation
This was the definition used in the EGDT Trial [PMID 11794169], the ProCESS Trial [PMID 24635773], the Arise Trial [PMID 25272316], and the ProMISE Trial [PMID 25776532]. It is not perfect, but at least we are all on the same page.
In a patient meeting the above definition, we are all pretty clear that if the goals of care are curative, we should pursue aggressive sepsis treatment. You can debate endlessly exactly what that care should be, but I think we all agree that we should be focusing our efforts on this group.
But of course, this is just a bit too clean cut for the world of quality.
SSC Guidelines
The fun started in 2012 with the revision of the Surviving Sepsis Campaign Guidelines [PMID 23353941].
Somehow this table managed to find its way into the guidelines:
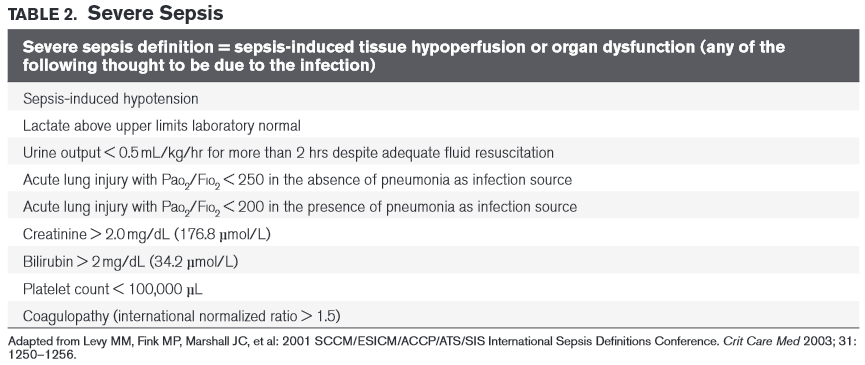
You can see at the bottom of the table, that these new criteria for Severe Sepsis are seemingly derived from this 2003 paper [PMID 12682500]. I still can't find where in the paper (which is actually a consensus document from a conference held in 2001), precisely where these variables emerged from–I imagine they were from some of the illness severity scoring systems, but who knows? But put that aside for a second, even if you give credence to these variables, note that in the table's heading it states …THOUGHT TO BE DUE TO THE INFECTION. This will become important in just a bit.
National Quality Forum
The NQF has been pushing for Measure 0500 (this link will take you to a version downloaded on 6/8/15) for a while now. We worked hard to get this one quashed just prior to the publication of ProCESS, as putting forth a new measure demanding CVP and ScvO2 seemed a bit silly at the time, but I digress. The NQF document has some new and fun definitions for severe sepsis:
SEVERE SEPSIS:
- Severe sepsis is defined as a suspected source of clinical infection, 2 or more manifestations of systemic infection (SIRS criteria) and
the presence of sepsis-induced organ dysfunction. - SIRS criteria include: Temperature >38.3 C or <36.0 C, Heart rate >90 beats per minute, Respiration > 20 breaths/min, White blood
cell count >12,000 or <4000/mm3, or >10% bandemia. - Organ dysfunction variables include:
- (SBP)<90 mm Hg or mean arterial pressure <70 mm Hg or a SBP decrease >40 mm Hg or <2 SD
below normal for age or known baseline - Creatinine > 2.0 mg/dl (176.8 mmol/L) or Urine Output < 0.5 ml/kg/hour for > 2 hours,
- Bilirubin > 2 mg/dl (34.2 mmol/L),
- Platelet count < 100,000,
- Coagulopathy (INR >1.5 or aPTT >60 secs),
- Lactate > 2 mmol/L (18.0 mg/dl).
- (SBP)<90 mm Hg or mean arterial pressure <70 mm Hg or a SBP decrease >40 mm Hg or <2 SD
SEPTIC SHOCK:
- Septic shock requires the presence of severe sepsis as above AND as sepsis-induced hypoperfusion persisting despite adequate fluid resuscitation OR lactate > 4 mmol/L.
- Sepsis induced tissue hypoperfusion is present with (SBP)<90 mm Hg or mean arterial pressure <70 mm Hg or a SBP decrease >40 mm Hg or <2 SD below normal for age or known baseline.
So what can we say about this little bit of delight. Well, they have re-dubbed severe sepsis to be something very different than we are used to or have read in any of the major sepsis studies. They seem to have conveniently left out the, “thought to be due to infection” that was in the SSC table 2. I am sure they will say, “we have the line sepsis-induced in there,” but unfortunately the measure itself doesn't list your clinical feelings anywhere as an exclusion–so that would be bunk. I am still fairly desperate to know the evidence for this new definition, but I haven't found it yet. Pretty unacceptable to hold every hospital in the US accountable to an arbitrary definition that has not been tested in large-scale trials.
Then we have a reimagining of septic shock. Somehow, septic shock now includes a lactate >4. The lactate >=4 was supposed to be the severe sepsis that went into the phrase that EGDT built: Severe Sepsis and Septic Shock. I'm not sure whose idea it was to conflate these two, but it is a bad idea. And where the hell does MAP<70 factor into this, every other shred of sepsis evidence uses a MAP<65.
Now what would they have you do in these patients?
A. measure lactate level
B. obtain blood cultures prior to antibiotics
C. administer broad spectrum antibiotics
D. administer 30 ml/kg crystalloid for hypotension or lactate = 4 mmol/L
E. apply vasopressors (for hypotension that does not respond to initial fluid resuscitation to maintain a mean arterial pressure >=65)
F. in the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was = 4 mmol/L, reassess
volume status and tissue perfusion and document findings.*
* To meet the requirements, a focused exam† by a licensed independent practitioner (LIP) or any 2 other items are required:
• Measure CVP
• Measure ScvO2
• Bedside cardiovascular ultrasound
• Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge
• Focused exam† including vital signs, cardiopulmonary, capillary refill, pulse and skin findings.
G. remeasure lactate if initial lactate is elevated
A is good–I'm with them there.
B is problematic. Yes, when possible get the blood cultures first, but the Surviving Sepsis Campaign actually addressed this issue in the wording of their recommendation:
We recommend obtaining appropriate cultures before anti-microbial therapy is initiated if such cultures do not cause significant delay (> 45 minutes) in the start of antimicrobial(s) administration (grade 1C).
- Kumar did a retrospective study over a sig. chunk of time that showed early antibiotics were associated with decreased mortality in patients with septic SHOCK. (Crit Care Med. 2006 Jun;34(6):1589-96.)
- Puskarich et al showed the same thing, again in septic SHOCK. Delay for patients not in shock did not seem to have an effect on mortality (Crit Care Med 2011;39:2066)
- Gaieski showed time from EGDT Criteria to antibioitcs was associated with mortality. This was the only one that showed Lactate>=4 also had an association and they didn't actually subset this group out. (Crit Care Med 2010; 38:1045–1053)
- de Groot showed early antibiotics didn’t matter unless the pt was in SHOCK [Crit Care 2015;19:194]
So the only real evidence (albeit not great evidence) is for patients who have septic SHOCK. And when I say shock, I mean shock the way everyone else in the world thinks of it as opposed to NQF–that is hypotension after initial fluids. Though the evidence isn't there, I think giving antibiotics within 3 hours for the Lactate>=4 group makes sense as well. It was done in the 3 recent big sepsis trials for those folks. But there is NO evidence for the NQF-redefined severe sepsis group, this portion of the measure should be rewritten to only include the EGDT criteria patients.
D of course should only list the 30 ml/kg bolus for patients who meet the EDGT definition as well.
E seems fine unless you have a 20 year-old, 50 kg female whose baseline BP may very well be a MAP of 60, but why should we let individualized medicine get in the way of quality measures
F is just plain silly. A desperate grab to keep big-brother ownership of what ProCESS, ARISE, and ProMISE demonstrated to be a purely clinical game.
and then G which seems fine, though we could quibble.
So in conclusion for NQF, go back to some real evidence based definitions of severe sepsis and septic shock, keep A, alter B, C&D get fixed with the repaired definition, E is fine, strike F, and keep G.
which brings us to… CMS
===
Antibiotic Delays and Feasibility of a 1-Hour-From-Triage Antibiotic Requirement: Analysis of an Emergency Department Sepsis Quality Improvement Database. Ann Emerg Med. 2019 Sep 24. pii: S0196-0644(19)30593-1. doi: 10.1016/j.annemergmed.2019.07.
CMS Measure
And now we tie the pain to the money.
We have the proposed SEPSIS BUNDLE PROJECT (SEP) v 5.0a, which I believe will go into effect in October 2015. From this document comes yet another definition of severe sepsis:
In order to establish the presence of severe sepsis, there are three criteria, all three of which must be met within 6 hours of each other.
- Documentation of a suspected source of clinical infection. There may be reference to “possible infection from xx”, “suspect infection from xx”, or similar reference in progress notes, consult notes, or similar physician/APN/PA documentation
- Two or more manifestations of systemic infection according to the Systemic Inflammatory Response Syndrome (SIRS) criteria
- Organ dysfunction,evidenced by any one of the following:
- Systolic blood pressure (SBP) < 90, or mean arterial pressure < 65, or a systolic blood pressure decrease of more than 40 mmHg from the last previously recorded SBP considered normal for that specific patient
- Creatinine > 2.0, or urine output < 0.5 mL/kg/hour for 2 hours
- Bilirubin > 2 mg/dL (34.2 mmol/L)
- Platelet count < 100,000
- INR > 1.5 or aPTT > 60 sec
- Lactate > 2 mmol/L (18.0 mg/dL)
When determining organ dysfunction, any single blood pressure or mean arterial pressure reading in the first hour after presentation that is abnormal, as described above, will satisfy the criteria for organ dysfunction.
So if a patient at any point has a single drop in BP or a lactate of 2.1 or an INR of 1.6 they are now severe sepsis in this imaginary evidence-free world. Note, now even the sepsis-induced has disappeared. So patients with a baseline Cr of >2 = you are screwed on the measure, sucker.
Looks pretty similar to the NQF measure right? That's b/c it is the same docs shepherding both of them.
What would they have you do with the patients that meet this definition?
Received within three hours of presentation of severe sepsis:
• Initial lactate level measurement
• Broad spectrum or other antibiotics administered
• Blood cultures drawn prior to antibiotics
AND received within six hours of presentation of severe sepsis:
• Repeat lactate level measurement only if initial lactate level is elevated
AND ONLY if Septic Shock present:
Received within three hours of presentation of septic shock:
• Resuscitation with 30 ml/kg crystalloid fluids
AND ONLY IF hypotension persists after fluid administration, received within six hours of presentation of septic shock:
• Vasopressors
AND ONLY if hypotension persists after fluid administration or initial lactate >= 4 mmol/L, received within six hours of presentation of septic shock:
• Repeat volume status and tissue perfusion assessment consisting of either
A focused exam including:
- Vital signs, AND
- Cardiopulmonary exam, AND
- Capillary refill evaluation, AND
- Peripheral pulse evaluation, AND
- Skin examination
OR
Any two of the following four:
- Central venous pressure measurement
- Central venous oxygen measurement
- Bedside Cardiovascular Ultrasound
- Passive Leg Raise or Fluid Challenge
So in order to understand this we need to know how they are defining septic shock:
a. There must be documentation of severe sepsis present.
AND
b. Tissue hypoperfusion persists in the hour after crystalloid fluid administration, evidenced by either
• systolic blood pressure (SBP) < 90, or
• mean arterial pressure < 65 or
• a decrease in systolic blood pressure by > 40 mmHg from the last previously recorded SBP considered normal for that specific patient
OR
• Lactate level is >= 4 mmol/L
Back to a mixed up vision of septic shock.
So how do we fix the CMS measure?
Simple:
- Keep the Lactate
- Change the ABX within 3 hours to their new definition of Septic Shock (i.e. the old definition/EGDT definition of Severe Sepsis and Septic Shock), and not their new vision of severe sepsis
- Eliminate the Blood Culture rule
- Keep the 30 ml/kg of fluid for the septic shock patients (by their definition) unless clinicians document why they felt the pt should not get this volume
- Keep the vasopressors
- Eliminate the focused exam silliness
Alternatively, everything could be fixed by defining the denominator as patients with persistent hypotension after fluids or Lactate>=4
Why Should You Care?
If the CMS measure goes through as currently written, we are hosed. Since all of this data will be collected retrospectively, there will be hundreds of patients deemed severe sepsis that you never even thought were sick.
And we are not even bringing up the Time Zero ridiculousness that this is all based on.
So why are we complicit?
Because these government organizations do not come up with this stuff themselves. Behind every silly CMS reg you are subjected to, there is, somewhere, a group of doctors that made it happen. Just as medical malpractice would not exist without a host of plaintiff witnesses, these measures would not exist without us.
Yeah!
Addendum
- SEP-1 One-Pager for Updates/Revisions
- sepsis core, no benefit except expense
- Great paper looking at simulated misses on real patients and whether they would have any impact
- Paper on the costs and benefits of these quality metrics (high cost low benefit)
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Hi Scott, I am a Nurse Practitioner in the ER, but have long background in EMS and ER nursing…worked in corporate quality for exactly as long as I could stand it…worked on Primary care side with CMS measures and understand the reasons for leaving out important stuff…They leave out what is not easily measurable data, whether or not it is vital…How can they measure “suspected infection” when they get most of their flagged cases from insurance claims data…ICD codes. They can collect lab data, diagnosis and procedure codes, but they cannot quantify and collect clinical judgement. It is a flaw… Read more »
Absolutely!!!
CMS and NQF both have public stakeholder comment periods. Your/our input is essential.
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/MMS/CallforPublicComment.html
tee hee hee hee hee hee
In some obscure corner of the detailed core measure explanation it appears that the CMS definition of a balanced crystalloid is either LR or NS. Our providers are moving steadily toward fluid resuscitation using balanced crystalloid solutions like Normosol-R. Does anyone know if there is a caveat for use of any isotonic crystalloid? Or are they really going to penalize us for using these better products?
I can’t imagine that being a problem, but that will up to your coders
Metabolic Theory of Septic Shock
Please do a search for the above
This is an incredibly important and depressing post. What has our world come to!
Cochran review Early vs late antibiotics in severe sepsis pre-Itu admission.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007081.pub2/full
No RCTs found
Something similar developing in the UK, will likely become a performance indicator, driven by the “sepsis trust”. It’s the policy management of severe sepsis in my hospital. Not sure how well validated the bundle is outside of my hospital. I’m told it has been repeated in other hospitals, but I have not found any published data. Some aspects of the bundle make sense. Some do not. The argument for early antibiotics is extrapolation from septic shock. Cochran could not find any RCTs in severe sepsis.
http://m.emj.bmj.com/content/28/6/507
Scot Nice review of the current Sepsis measure. Hospitals will be/ are struggling with this measure. To answer your request to be more participatory I have included the following lnk from CMS. Remember this is a huge volume IQR call but they do have opportunity to ask and more importantly submit questions. I would suggest any one who has some thoughts on this topic to attend and submit questions and concerns. You may register for the webinar at the following link: https://cc.readytalk.com/r/wzscq465sz0&eom. This IQR webinar, titled “Early Management Bundle, Severe Sepsis/Septic Shock” will be presented and will provide the basis,… Read more »
the docs running this webinar are the complicit docs
Excellent post! This is the most eloquent breakdown of this terrible Core Measure I’ve seen. Thank you! The irony, of course (as with most stupid CMS measures) is that this will increase costs in the long run (without benefiting care), when we start treating CHF/COPD exacerbation’s, pancreatitis, PE’s, SBO’s, and AKI’s like they are all sepsis (last time I checked, there is more than one kind of shock). Kindey failure…here’s some Zosyn and Vanc! Pulmonary edema with elevated WBC…here’s 2 L of fluids! Frail elderly patient who is normotensive w/ MAP of 70..here’s a line in your neck! This is… Read more »
yes!
The worst part is, if we give all the antibiotics so that we don’t fail the measure, which we are ALL already pressured to do…along comes the next measure!! Somebody is already typing somewhere… Numerator: Number of patients presenting with sepsis who are found to be resistant to any antibiotic given during any previous admission…:) http://www.qualityforum.org/News_And_Resources/Press_Releases/2015/NQF_Statement_on_the_White_House_Effort_to_Combat_Antibiotic_Resistance.aspx Seriously though, I have seen a few comments in here saying you can make a difference through public comment period…but the rule is listed as “finalized” and the meeting that is posted above is not for the purpose of commenting, it is for the… Read more »
nowhere in this discussion is there a discussion about bacteria unless you include “we all like antibiotics for bacterial infection” the problem with the sepsis debacle is that none of it is focused on microbiology or the early pathologic identification of the microbe causing the infection in real time. this recent paper hit a great nail on the head of our numbskulls when it decried the lack of a pathologic diagnosis in emergency department. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4307726/ the answer my fine friends as told by Semmelweis, Koch, Lister, Pasteur et al is to be found in the laboratory and not on the… Read more »
Absolutely right Dr.Weingart.. There has been tremendous public health value derived in the efforts of delivering enhanced sepsis awarenes in the ER, EMS, and on the wards and the need for early fluids and antibiotics. For example I recently sent a e coli urosepsis case to the ER and they managed the case like we would have in the ICU. Within a few hours he received 4 liters of NS. His HR fell from 130 to 96. His Lactate fell from 2.2 to 1.5 and by the next day his creat. had fallen from 2 to 1.5. The bringing of… Read more »
Sorry that was the wrong link. Here is the link which tells the almost unbelievable history of 25 years of pathological, dead end, Sepsis Science. Read this and you will understand why the clinical docs are beginning to push back. Read this again if you read it in the past. You will note that all that it predicted when it was written, has come true. Remember the hope for all those randomized trials. PROCESS, ARISE, PROMISE. If the linked article was right …. they never had a chance. Of course, in the end, that was exactly the case. It is… Read more »
There are a variety of incorrectly positioned assumptions in this critique. The most prominent is that any of the 4 trials on septic shock somehow included a definition of severe sepsis. This is simple false. The trials defined shock and were silent ion the definition of severe sepsis. The next faulty assumption is that “Somehow, septic shock now includes a lactate >4. The lactate >=4 was supposed to be the severe sepsis that went into the phrase that EGDT built: Severe Sepsis and Septic Shock.” This is again simply a misstatement of the facts. Lactate >= 4 is a part… Read more »
This is a illustrative example of the collision of medical threshold science (also called thresold decision making) which originated in the 1970s and 80s with concepts of ROC and the work of Paulker, et al. and the clinicians who have learned to their sorrow the personalized consequences of utilitarian, “one size fits all” threshold rules based medicine for complex heterogenous dynamic group of phenotypes of severe infection which we call sepsis. The application of threshold based rules (as one might for ACS or acute carotid occlusion) to the broad range of sepsis phenotypes with no known time of onset is… Read more »
Lawrence, this is an elegant theory and the letter you cite explains much of it well, but it’s a prescription to nowhere. Just as much as threshold science has been used to built this monster, threshold science is being used to deconstruct it. Is there another science we should be applying? And how do we know it has better results or is a better fit? Essentially it comes down to this: never has a public health campaign endured more head-on and sideways at tacks and criticism as the Surviving Sepsis Campaign. Often these criticisms come as critiques of our methods,… Read more »
Sean I support the SSC and never argued that it was not a good idea. I am not sure that the entire claimed reduction in death is supported by solid science given the fluidity of the criteria defined denominator over the past decade, However, the culture in the ER relavant timely intervention has been greatly improved by SSC. A major achievement in the interest of public health My problem is with the present science of sepsis. In particular, the collection, analysis and reliance uoon preselected gilded thresholds. These are data fragments upon which scientists and clinicians have anchored. This has… Read more »
I have been asked to explain my comments in simpler terms. Let me summarize. The acheivements of SSC thought leaders rank with other great medical leaders. We are thankful for their brilliance, hard work. and dedication to public heath. However now, in 2025, it is important to understand that: “There are no thresholds of sepsis, thats a 1980s myth. There are only the dynamic relational patterns of the different phenotypes of sepsis.” ER docs are faced with these complex patterns while regulators are listening to those well meaning thought leaders who, for 25 years have been convinced they could define… Read more »
One might ask why are we, as clinical sepsis researchers, so desperate that we resort to SOME in an intellectual challenge to the sepsis dogma? To explain how our problems mirror those of the ER physcian, here is the pivotal statement from Scott in this blog. “I am still fairly desperate to know the evidence for this new definition, but I haven’t found it yet. Pretty unacceptable to hold every hospital in the US accountable to an arbitrary definition that has not been tested in large-scale trials.” That is what sepsis researchers working outside the dogma have faced for over… Read more »
Thank you for sharing the story Sherrie! It kind of weaves in so much well with our storyline and suite of cloud based Sepsis solutions and software that primarily assist nurses and physicians in the sepsis care process. As a nurse you are aware of the time delays that do happen unintentionally, in the care process. Added to it is the gaps i the care transition process when nurses and physicians change their shifts and handover care to the next set of care providers, In all this chaos, hospitals fails to adhere to the sepsis bundle protocols mandated by the… Read more »
Great discussion and comments. However, my issue with all of this is more unsophisticated… Where the statement exists above “after crystaloid fluid administration”, does that mean after a 30 ml/kg fluid bolus, or some “reasonable amount of fluid”? ..and does CMS clarify how rapidly this fluid bolus should go in? That is very difficult for me to clarify, as I’m involved peripherally with our hospital’s attempt to make sense of all of this. In addition, the IS department is trying to build a module in Epic to help with the abstract recording times. They have similar questions regarding the fluid… Read more »
How much fluid is too much for these patients? Say young, showing early signs of DIC, renal failure, and with a mild trop elevation? Recent contextual invasive strep A exposure.
Many thanks from Canada,
who are the people on the committee? someone with a website that has a large following of healthcare providers (for example Scott Weingart) should start a web petition to remove the inane parts of the guidelines. that’s about the only way docs in the trenches will have a voice.