by Neha Dangayach
Case vignette
Our patient, let’s call him Mr. KM is a 35 year old with PMH of hypertension who presented with acute onset of confusion, dysarthria and severe headache. While waiting in the ED triage bay he became suddenly unresponsive. The ED team rapidly assessed him, called a stroke code and intubated him. They found the following on their exam right before intubation:
Vitals: Blood pressure by non-invasive cuff 200/110, HR 100, sinus tachycardia, afebrile
Focused Exam: Pupils anisocoria: Right pupil 4 mm and Left 2 mm and both sluggishly reactive
On painful stimulus, he was extending bilateral upper extremities and was triple flexing bilateral lower extremities. His tone in all extremities was increased. His airway was secured using the EMCrit NeuroCritical Care airway paradigm And he received mannitol 1 gm/kg bolus and a liter of isolyte post-mannitol. He was hyperventilated, head was positioned at 30 degrees and maintained in the midline.
Differentials at this time included: stroke due to emergent large vessel occlusion (ELVO), potentially a basilar clot or vertebral dissection extending to the basilar; subarachnoid hemorrhage (SAH), hypertensive intracerebral hemorrhage (ICH). Post-intubation he was started on a Propofol drip but his blood pressure was not lowered given the concern for ELVO. The ED resident took Nicardipine with her to the CT scanner in case they found a bleed. While the patient was being put on the transport monitor, he was also loaded with Keppra 60 mg/kg intravenously as seizure prophylaxis and to cover for any possible cause of a non-convulsive seizure.
How to do a focused neurological exam in a comatose patient?
In an excellent expert panel report from the European Society of Intensive Care Medicine (ESICM) on the neurological exam in critically ill patients, there are several key suggestions on how to perform focused neurological examinations, how frequently to perform them and how to develop a systematic approach to leveraging such an exam for timely diagnosis and management.

While the following steps aren't all exhaustive, these should be considered as practical steps for doing a focused exam in any patient with suspected coma and customize your exam based on the clinical scenario. The IBCC post on Stupor and Coma describes these steps in much more detail along with the anatomical basis for some of the reflexes etc.
First, make sure that you are able to stop any sedative and analgesic drips safely. If you’re in the ICU, always update the bedside nurse that you’re going to stop sedation to do a wake-up exam. Depending upon the agents being used, cumulative dosing, presence or absence of any underlying hepato-renal dysfunction, you can estimate how long it’ll take for a patient to wake up. For the type of patient who slips into a coma acutely in your ED like Mr. KM; you can jump right into a focused exam. So, once you have waited at least 10-15 minutes and see some signs suggestive of the patient waking up, start your exam with head in the midline, eyes in the midline, uncover the arms and legs and place the arms in the midline.
At every step of this exam, check what response you get and be systematic. Some of these elements of the exam will help you determine an objective score such as GCS (Glasgow Coma Score) or FOUR score.
Score their LOC (Level of Consciousness)
First, call out their name. If there’s no response then grab them by the shoulder (this is the equivalent of deep touch) and if there’s no response give them a painful stimulus. Some examples of painful stimuli include sternal rub, supra-orbital pressure, nail-bed pressure. Observe eyes, face, extremities. The GCS has its limitations but I think it’s utility lies in getting an objective assessment of coma. GCS 8 or less is the equivalent of coma. Coma i.e. lack of awareness and arousal. For each of the responses then note the Eye, Motor, Verbal scores. This establishes your baseline. (For Mr. KM. our GCS is E 1 (no eye opening), M2 (extensor posturing in Upper extremities) V1 (no verbal response)=4 (Figure1)

Figure 1 a. https://www.mdcalc.com/glasgow-coma-scale-score-gcs

Figure 1b. https://www.mdcalc.com/four-full-outline-unresponsiveness-score
Arousal
As part of your assessment for arousal, if they have eye opening then assess whether your patient has a gaze preference, a gaze deviation etc. Do they have face regard i.e. do they look at you. Do they have visual tracking i.e. do their eyes follow you around in the room. After you’ve assessed arousal, then you proceed to assess command following. If they aren't opening their eyes to any stimulus including pain, then make sure you open the eyes and assess for gaze preference, gaze deviation etc.
Following Commands
Typically, you want to start with axial commands followed by appendicular commands. Axial commands e.g. Open and Close your eyes, Stick your tongue out. Appendicular commands: Eg. Show we two fingers, give me a thumbs up, wiggle your toes.
Practical Tips: For patients who have eyelid apraxia usually seen in patients with non-dominant hemisphere lesions, you’ll have to hold the eyes open to assess arousal. Squeeze my hands, is not a good command since you might get a false positive due to a plamar flexor response
Don’t forget to restart sedation or analgesia as needed. Use the right dose, right agent and analgosedation first and titrate to appropriate goals. In cases of suspected ICP, use both sedation (E.g. Propofol) and analgesia (e.g. Fentanyl) (Ref: PADIS guidelines)
Brainstem Reflexes
At the very least, in addition to pupils check the following: corneal's bilaterally, cough and if no suspected cervical cord injury then check doll's eye reflex or vestibular-ocular reflex. For the corneal's reflex I recommend using a little bit of sterile water or saline or a q-Tip (if readily available) and don't forget to wipe the eyes down after your assessment. When you check for doll's, check where the eyes are in the primary gaze position (is there any deviation, preference etc. ) in addition to presence or absence, also look for any abnormal response, vertical movements, nystagmus etc.
Practical tips: If your patient is easily arousable, then you can skip doll's, corneal's. Before checking for doll's eye, check the position of the eyes in the primary gaze position.
Gaze preference versus forced gaze deviation: Understand the difference between gaze preference (which can be overcome when you elicit a doll's eye response) as opposed to gaze deviation which can't be overcome by doll's. Forced gaze deviation will usually suggestive of a seizure.
Tone, deep tendon reflexes, plantars
I'll typically check for tone i.e. passive resistance to movement in all extremities. I usually don't check deep tendon reflexes in all patients unless I am think it'll provide me with some incremental information. It is worthwhile eliciting the plantars response as an asymmetrical response with an up-going toe on one side or both up-going toes may give you diagnostic clues for lateralized lesions.
How should one develop differentials for coma?
These are the principles I use while developing my differential diagnosis for coma:
Parallel process-is there something structural, electrographic or iatrogenic that can explain this patient’s coma. Or is it a combination of different causes, in which case, what is the primary driver?
So, once ABC is secured, I’ll make sure we get a quick fingerstick and have a team member coordinate a stat scan. The choice of scan will depend on the differentials and how stable the patient and can they tolerate laying flat. For example, for a patient like Mr. KM I want to get the fastest possible scan so we can activate other teams such as neurosurgery, neuroendovascular etc. depending upon what we diagnose on the scans. So, I’ll get a stat CTH/CTA head and neck just like the ED team did. If your center is able to do an MRI brain in a similar time frame as compared to CT, then you could also opt for an MRI/MRA stroke protocol. However for Mr. KM I am worried about his pupillary anisocoria, it’s telling me that he’s going to need an emergent intervention, he probably has raised ICP and I don’t think I want him laying flat in the MRI scanner for even a few additional minutes.
Practical Tips: You can pre-treat your patient’s suspected elevated ICP by giving them a dose of hypertonics (mannitol or a hypertonic saline bolus) before laying them flat for a scan. Make sure your transport team keeps the head of bed up to 30-45 degrees throughout transportation and that you hyperventilate them either using a BVM or the transport ventilator. Don’t wait to get scans based on laboratory results…Parallel process.
Seizure Prophylaxis: In addition to looking for a structural cause, since there will be some delays in getting any patient connected to continuous EEG monitoring, it might be worthwhile loading them with an anti-seizure medication till we have more diagnostic certainty.
Recheck pupils: Post intubation and after receiving paralytics we know that our patient’s pupils shouldn’t become unreactive, but they will lose motor responses in various skeletal muscles. Immediately post-intubation, before you move the patient for any scans, recheck the pupils and treat raised ICP if the pupils have become unreactive or anisocoria has worsened.
You can utilize quantitative pupillometry and/or optic nerve sheath diameter (ONSD) to assess response to your therapies as you get the patient ready for scans.
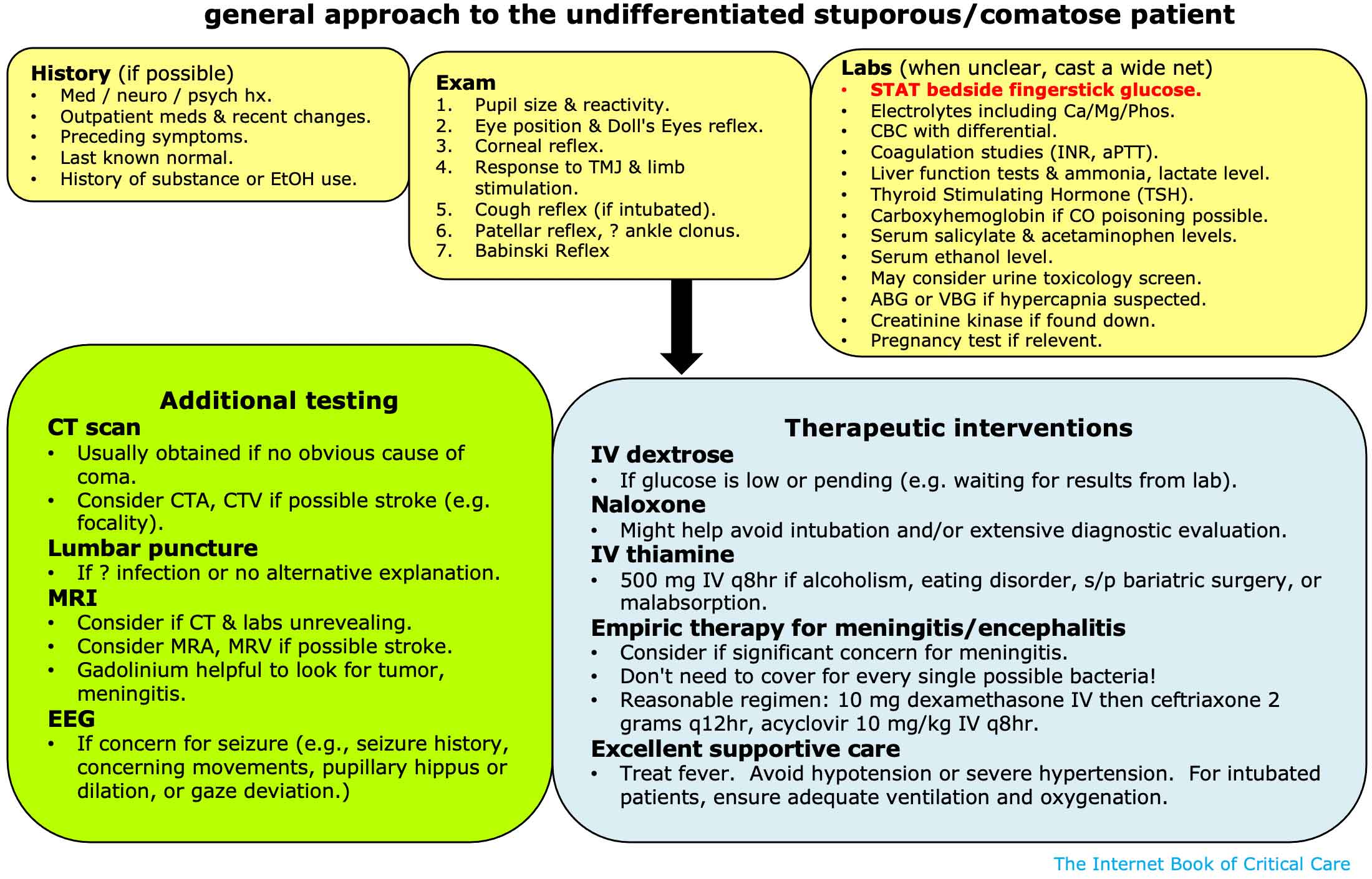
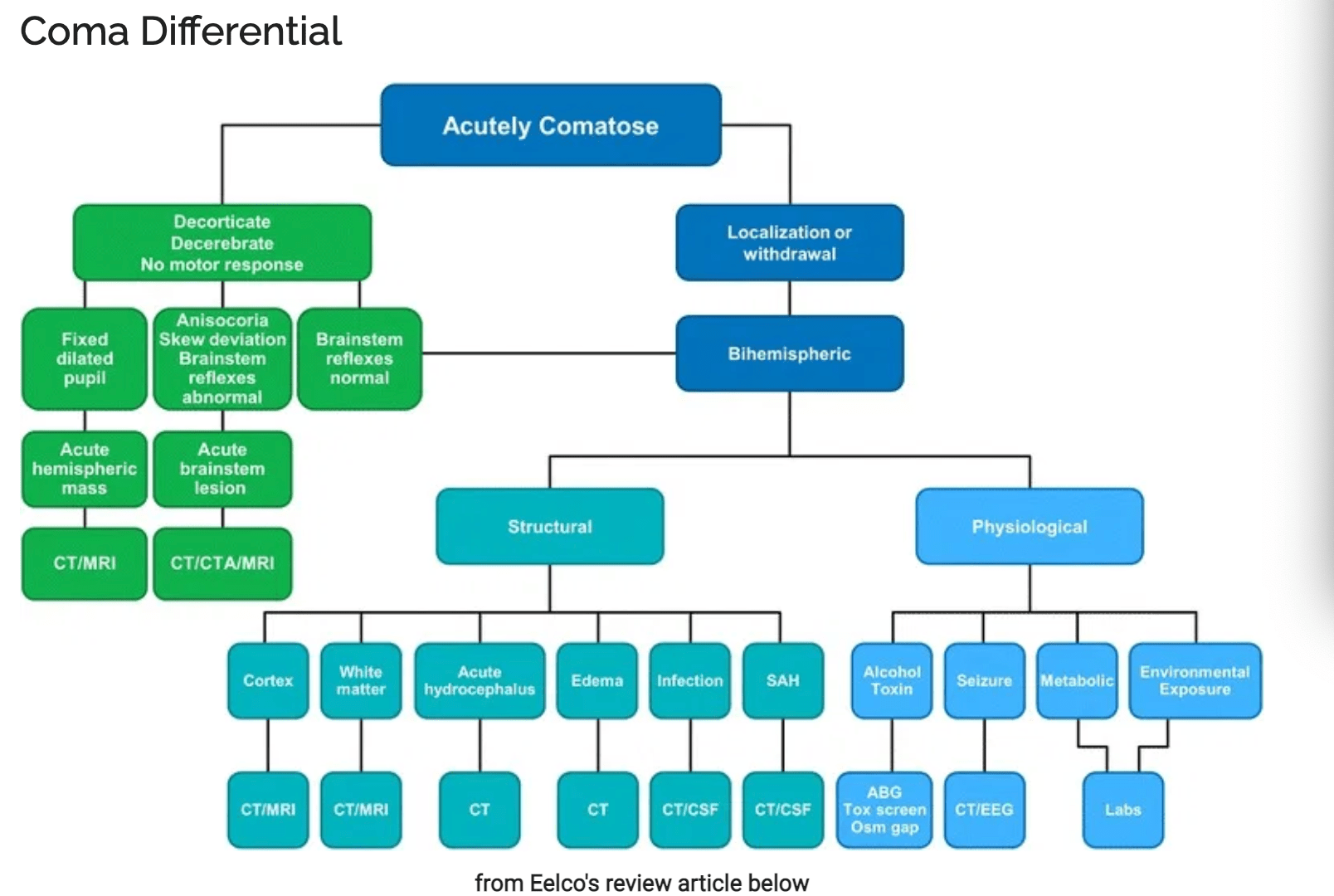
Be systematic: Coma has a lot of different causes and the following figures from the IBCC are great for organizing your differentials and do the initial work-up.
Practical tips-I will usually get vascular imaging depending upon the clinical context. I do think that if you’re going to scan a patient whether it’s a CT or MRI, it’s important to pause and think whether you want vessel imaging for any of your differentials or not. You don’t want to keep sending a critically ill patient back to the scanner for additional imaging and ensure that you can activate the endovascular suite in a timely fashion because as always, Time is Brain!
Engage timely help: At every step of the way ask yourself, can I narrow my differential down and which other team do I need to engage. For Mr. KM on the non-contrast CTH we see high grade SAH, he has global cerebral edema and severe hydrocephalus. His CTA shows a fusiform left posterior inferior cerebellar artery (PICA) aneurysm. And as soon the ED resident sees the non-contrast CTH, she asks the radiology tech to pause and starts the nicardipine drip for SBP goal 100-140 mm Hg and cycles the blood pressure cuff q5 minutes till the blood pressure is within range. While the radiology tech is running the CTA, the stroke resident notifies the neurosurgery and Neuroendovascular teams on call regarding the need for emergent EVD and for activating the endovascular suite. The ED resident notifies the Neurocritical Care team about the need for an ICU bed. Mr. Kim’s right pupil isn’t reacting after he comes out of CT and the ED resident institutes all ICP precautions and gives a 250 cc bolus of 3% via the peripheral iv line.
This kind of parallel processing leads to excellent teamwork and prepares our teams and patients for success.
Mr. KM was rapidly taken up to the Neuro-ICU for an EVD placement. His pupils returned but he remained in a coma. He underwent an angiogram and coiling of his aneurysm. The placement of his EVD was confirmed via a dynamic CTH performed in the endovascular suite saving him another trip to the CT scanner. Post coiling his EVD was lowered to 10 cm above head level from 20 cm but he didn't wake up on post bleed day 0 (the first day of symptom onset or the first day for SAH patients). Since his exam didn't improve he was connected to continuous EEG monitoring. No seizures were identified on his EEG and his Keppra was continued for seizure prophylaxis for 7 days as per institutional protocol. He woke up and started following simple commands on post bleed 2 as his hydrocephalus continued to improve.

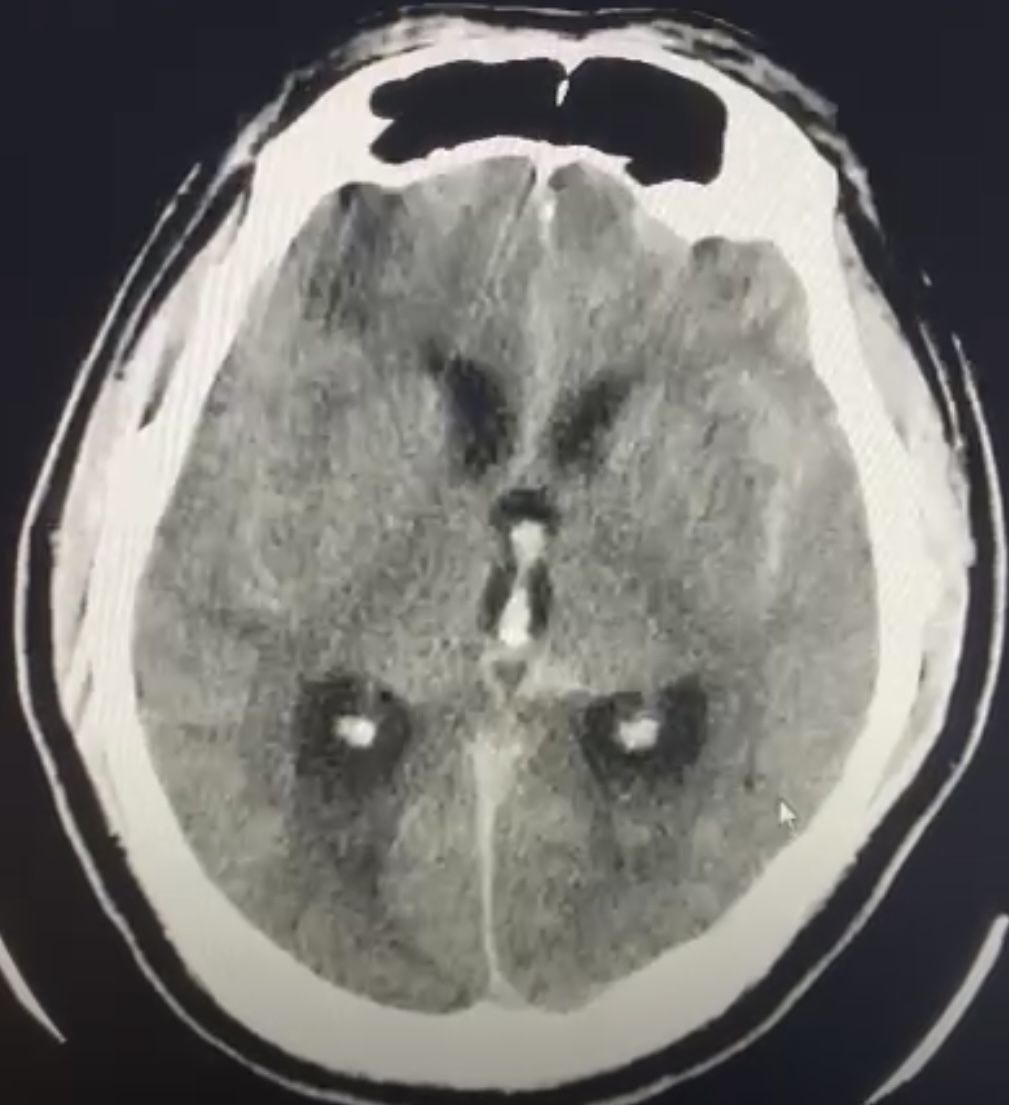
Figure 2. Non-contrast CTH showing thick subarachnoid hemorrhage, global cerebral edema and hydrocephalus.
Additional Emcrit Resources

Another awesome neuroemcrit post, and what an amazing ER resident you have (brings Cardene with her to the scanner!) ..in reference to this part of the post
“he was also loaded with Keppra 60 mg/kg intravenously as seizure prophylaxis and to cover for any possible cause of a non-convulsive seizure.”
do you typically use status dosing as prophylaxis ? is that dosing carried out for the full seven days when EEG is negative ?
Thank you so much Marisa. Indeed we have some fantastic ER residents 🙂 Regarding Seizure prophylaxis dosing, I’ll usually use 1000 mg Q12h iv for average size adults and lower for eg. 500-750 mg Q12h for older, frail individuals with lower BMIs. In patients I suspect convulsive or non-convulsive status or when it’s unclear but my clinical suspicion is high, I’ll load (like in this case). Once convulsive or non-convulsive seizures are ruled out, I’ll switch to prophylactic dosing if indicated. Our institutional consensus for seizure prophylaxis: 1) Post craniotomy patients 7 days 2) SAH patients 7 days 3) TBI… Read more »
Excellent post by a first-class educator! Look forward to more neurocrit pearls from Dr Dangayach in the future.
Thank you David! If you have any recommendations for topics send them over. Yes, will be writing a post soon tackling important questions raised by SKIP and DEVT 🙂
Excellent post. How are you monitoring for vasospasm in a comatose patient such as this and what’s your protocol when you suspect it is present?
[…] Critical Care – Coma tips, Airway paradigm, Post-it […]