What is this page about?
Scott Weingart, MD and Richard Levitan, MD published an article in the Annals of Emergency Medicine entitled Preoxygenation and Prevention of Desaturation during Emergency Airway Management.
This page serves as a repository for supplementary material on the subjects raised in the article.
The article is available for free on the Annals EM Site (pdf)
Updated Recs for Preox of All Patients
Rule of 15's
- All patients get NC @15lpm and NRB at >=15lpm (Flush rate/the higher the better)
- If you cannot achieve Sat of 100, replace NRB with CPAP at up to 15 cmH20
listen to this Wee for more
Flush rate NRB is as good as BVM1
CPAP for Preoxygenation
In a patient with shunt, CPAP is needed for preoxygenation. In my ED, we make this happen with the ventilators installed next to every resuscitation bed.
However, not every ED has ventilators readily available and it might take >15 minutes to have respiratory bring a NIV machine or a vent. In that case, you want to use a BVM with a PEEP valve.

However, this device provides CPAP only when the patient is expiring. In a patient who is not breathing rapidly, most of the cycle will be spent at zero PEEP. Once the patient is apneic, the device won't supply PEEP unless you manually give ventilations–even then the PEEP will only be there immediately following the ventilation. However, if you add a constant source of flow, like a nasal cannula set to 15 lpm then the BVM/PEEP Valve combo will give continuous PEEP regardless of the patients resp rate or even when they become apneic. In the following video, a PEEP valve set to 10 cm H20 provides between 6-8 cm H2) of PEEP throughout the cycle. This same nasal cannula should be on the patient anyway for apenic oxygenation and NO DESAT (Nasal Oxygen During Efforts Securing A Tube) during the intubation procedure.
New CPAP for Preox Articles
(Indian J Anaesth 2015;59(4):216)
Other Articles of Interest on Preoxygenation/Reoxygenation/Preventing Deoxygenation
Dr. Levitan's site for airway videos and courses
The airwaycam site is an amazing source for educational materials and equipment to help you manage ED airways.
If you liked the article and/or this page, you'll probably like the EMCrit Blog and Podcast…
why not check it out at emcrit.org?
Want Additional Information?
Email us on the contact page.
Additional Articles for Version 2.0
More evidence that if the patient starts low, their risk of desat is much greater (Acta Anaesthesiologica Scandinavica Volume 57, Issue 2, pages 199–205, February 2013)
Nicholas Chimes revalidates many of these concepts on his FiO2 Testing Page
Apneic Oxygenation
Here is the evidentiary table published in the Original Article

Great New Review Article (Critical Care and Resus 2014;16(3):233)
New Evidence
ApOx for PanEndoscopy (10.1177/0194599813486248 Otolaryngol Head Neck Surg April 12, 2013 0194599813486248)
Apneic Oxygenation via Nasal Prongs at 10 L/min Prevents Hypoxemia During Elective Tracheal Intubation
Chest. 2013 Oct 1;144(4_MeetingAbstracts):890A. Christodoulou C, Mullen T, Tran T, Rohald P, Hiebert B, Sharma S.
PURPOSE: Hypoxemia during airway management remains an important cause of morbidity and mortality. Oxygenation during intubation via nasal prongs may prevent critical desaturations (Anesthesiology 1988, J Korean Med Sci 1998). We evaluated the effectiveness of oxygen administration via nasal prongs during apneic period following induction of general anesthesia.
METHODS: We conducted a randomized, controlled, double-blind study in patients without significant cardiac or respiratory disease undergoing elective surgery (age 18-65, ASA I-III). Patients randomly received oxygen via nasal prongs at 0, 5, or 10 L/min. Following preoxygenation, general anesthesia was induced. At 90 seconds after induction, nasal prongs were applied and oxygen was delivered according to the experimental group. At 4.5 minutes post-induction the patients were intubated.
RESULTS: The final study population consisted of 41 individuals, with 14 in the 0 L group, 13 in the 5 L group, and 14 in the 10 L group. The mean values are 134 ± 75, 168 ± 138 and 253 ± 146 mmHg respectively. A statistically significant difference was demonstrated between the three treatment protocols (p=0.030), across time (p=0.028), and in the treatment effect across time (p=0.017). Mean PaO2 was higher in the 10 L group (p=0.001) than the 5 L group and 0 L group at 4.5 minutes (p=0.004). CONCLUSIONS: Apneic oxygenation with 10 L/min compared to 5 Lmin via nasal prongs demonstrated delay of desaturation and maintenance of higher PaO2 levels during elective intubation.
CLINICAL IMPLICATIONS: Nasal prongs are available in all of the patient care areas; therefore this simple, benign, inexpensive technique may be useful as a routine addition to airway management.
PMID: 24154362
Must be high-flow to overcome mask leak
Addition of Nasal Cannula Can Either Impair or Enhance Preoxygenation With a Bag Valve Mask: A Randomized Crossover Design Study Comparing Oxygen Flow Rates. Anesth Analg. 2018 Apr;126(4):1214-1218. doi: 10.1213/ANE.0000000000002341.
ApOx and Shunt Physiology
This article lends credence to the point that patients with shunt physiology either preexisting for during apnea will not benefit to same extent (Anesthesiology 1973;39(6):588)
and this one [Anesth Analg 2019;128(6):1154]
Systematic Review (Anesth & Intens Care Volume 45, Issue 1 Apnoeic oxygenation during intubation: a systematic review and meta-analysis)
Nasal Cannula to Augment Face Masks (as Rich and I advocate)
Supplementation of standard pre-oxygenation with nasal prong oxygen or machine oxygen flush during a simulated leak scenario
DOI: 10.1111/anae.12630
The presence of a facemask leak significantly reduces the effectiveness of pre-oxygenation and increases the risk of post-induction hypoxia. We randomly assigned 24 healthy volunteers to a six-period crossover trial with and without a simulated facemask leak. Pre-oxygenation was performed using a standard anaesthesia machine circuit supplemented either by nasal prong oxygen or by anaesthesia machine flush oxygen. Each intervention was completed with both 3-min tidal breathing and 8 deep breath techniques: end-tidal oxygen fraction was used as the measure of pre-oxygenation effectiveness. The presence of a stimulated mask leak significantly reduced the effectiveness of pre-oxygenation regardless of the breathing method used. With a simulated facemask leak introduced, the mean (SD) end-tidal oxygen fraction with the 3-min tidal breath technique was 74.7 (9.3)% compared with 57.5 (6.2%) for the 8 deep breath technique with 3-min tidal breathing and a leak. End-tidal oxygen fractions increased by 11.0% (95% CI 7.8–14.3%) (p < 0.0001) with the addition of nasal prong oxygenation and 16.8% (13.6–20.0%) (p < 0.0001) with machine oxygen flush compared with standard pre-oxygenation. When a leak is present, 3-min tidal breathing with either nasal prong or anaesthesia machine flush oxygenation is an effective pre-oxygenation method, and preferable to the 8 deep breath method.
Can we use ETCO2 Monitoring NC for ApOx?
No
Review of various dual-use NCs
Best Reviews of High-Flow Nasal Cannulae
[cite]23271822[/cite]
High Flow Nasal Cannulae for both Preox and ApOx
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways (doi:10.1111/anae.12923)
and
Use of High-Flow Nasal Cannula Oxygen Therapy to Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate Hypoxemia.
Crit Care Med. 2014 Dec 4.
Miguel-Montanes et al.
CONCLUSIONS:: High-flow nasal cannula oxygen significantly improved preoxygenation and reduced prevalence of severe hypoxemia compared with nonrebreathing bag reservoir facemask. Its use could improve patient safety during intubation.
Will Patients Tolerate 15 lpm by NC?
Andy Brainard shows that of course they will: (Brainard A et al. A Randomized Trial on Subject Tolerance and the Adverse Effects Associated With Higher- vs Lower-Flow Oxygen Through a Standard Nasal Cannula. Ann Emerg Med 2014. PMID: 25458980)
Prehospital ApOx
NIPPV for Sedation
Reuben Strayer's NIPPV for Procedural Sedation Case Series [cite source='pubmed']25455053[/cite]
Probably not a Clever Move to use Nasal Trumpets
Anaesth Intensive Care 2015 Mar;43(2):244-8
=======================================================
Here is a bit of follow-up on prior EMCrit discussions and some new stuff for Janu-Airway
Updated Recs on Preox in Non-Shunted Patients
Original Article: Weingart & Levitan on Preoxygenation
Evidence [cite source='pubmed']24931923[/cite]
Will Patients Tolerate 15 lpm by NC? Andy Brainard shows that of course they will: [cite source='pubmed']25458980[/cite]
Bodily, JB et al. Incidence and duration of continuously measured oxygen desaturation during emergency department intubation. Ann Emerg Med. 2016 Mar;67(3):389-95. PMID: 26164643
Reiterated the 93% risk of desaturation, 1/3 of ED intubations had desat < 90%
And 1st Attempt is CRITICAL
The Rule of 15's
Every patient gets a NC @15 lpm
Try adding a Non-Rebreather Mask at 15 lpm
If that doesn't get the Sat to >= 95%, change to BVM on 15 lpm with a PEEP valve set to up to 15 cm H20 Water
Hi-Flow Nasal Cannulae for Apneic Oxygenation
- Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways [cite source='pubmed']25388828[/cite]
- Use of High-Flow Nasal Cannula Oxygen Therapy to Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate Hypoxemia. [cite source='pubmed']25479117[/cite]
- Josh Farkas has a great post on sole use of high-flow NC
- Best Review of High-Flow Nasal Cannulae [cite source='pubmed']23271822[/cite]
Why BVM Recruitment is a Failure
I got a G+ post from Frederic:

These are a fantastic set of questions! I briefly address them in a Grand Rounds talk I give (LaMW: Ox Kills), but even in that talk I don't give this topic the time it deserves. So hence this wee…
How do alveoli open and close?

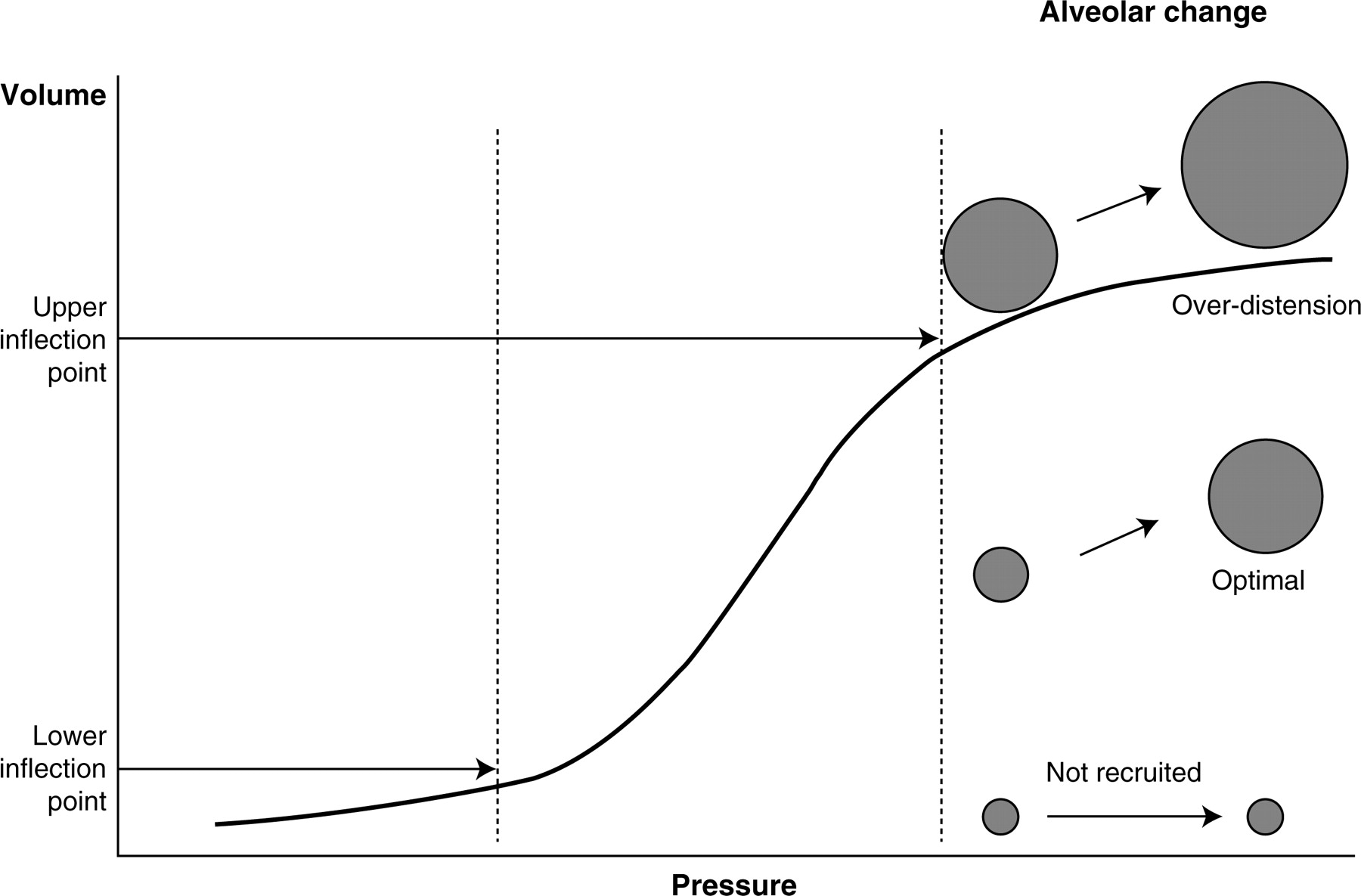
Watch this video from Dr. Slutsky:
and this one
George Kovacs and Nick Sowers recorded these two cadaver videos with their AIME Crew:
Atelectrauma
Atelectrauma is bad!
Does BVM Vent Lead to Aspiration
Avoid Derecruitment with Tube Clamping
Articles of Interest
- Reuben Strayer's NIPPV for Procedural Sedation Case Series3
- Sydney HEMS on Prehospital ApOx [cite source='pubmed']25536868[/cite]
More on the Head-Up Intubation Position
VAPOX and Vent-as-Bag
Ventilator-assisted preoxygenation: Protocol for combining non-invasive ventilation and apnoeic oxygenation using a portable ventilator
Steven Grant DOI: 10.1111/1742-6723.12524
Head Up is the Way to Go
Khandelwal N, Khorsand S, Mitchell SH, Joffe AM. Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Anesthesia and analgesia. 122(4):1101-7. 2016. PMID: 26866753
also see Semler RCT for opposing view
Brindley's PREPARE Article
Sakles Editorial
from AEM4
Nasal Cannula fixed BVM Leak and improved standard NRM
from Hayes-Bradley56
Nick Chrimes Airway Adjunct Sheet


This ‘poor-man’ NIPPV method (high flow NP+BVM) requires 2 Oxygen sources?
George
Clarification: This ‘poor-man’ NIPPV method (high flow Nasal Prongs+BVM/PEEP valve) requires 2 Oxygen sources?
George
This may be a silly question but is o2 flowing through the bvm when the bag is not being squeezed?
nope, nothing comes out of the bag unless you squeeze
Hi, I think that might be wrong. O2 flows through the one way valve constantly- this can be felt and heard when checking the BVM.
When the patient inspires the flutter valve will open further and they will draw in O2 from the bag and reservoir, providing there is a good seal.
Nope, a majority of bags are manufactured with valves that put the oxygen out the back unless the front duckbill is open.
In the breathing patient, which is the more effective oxygen delivery method:
1. Commercial CPAP device (Flow-safe, Boussingnac)
2. BVM with PEEP
I assume the combination BVM/PEEP with Nasal Prongs is better than above but requires 2 sources of O2.
George
Best would be commercial cpap with nasal cannula; which also requires 2 sources O2
Is this actually Bi-Pap?
nope, cpap
Why use CPAP and not BiPAP? Does it matter?
Thanks!
BiPAP brings nothing to preox but does push you closer to opening the esophageal sphincter and therefore causing gastric insufflation
It was nice to be able to cite (after the fact) anaesthetic literature (via your article) to an anaesthetist who tried to tell me that nasal cannula oxygenation would not be helpful during a high risk RSI.
🙂
Scott,
Just clarification, but if we’re using an LTV1200 for CPAP during PreOx, it would be easier to continue using the vent during ApOx? If in a situation where you have NIV capabilities, one could leave the mask on, and just switch to A/C to use the vent while patient is apneic, right?
Lee, Sorry I missed this comment originally. You still need the nasal cannula for even vented apneic ox as the vent will not pick up the small O2 utilization as a breath. But a vent set to PEEP or a very low RR with a NC underneath would work wonderfully.
Scott, excellent, … great tips regarding oxygenation, thank you. A word re the use of NIV during the apneic period. The LTV 1200 that Lee is using does provide a continuous bias flow of O2 at 10 lpm and will maintain CPAP (as long as the conserve O2 feature is “off”) whether the patient is spontaneouly breathing or apneic. The addition of NC may not add any advantage as the ventilator will maintain constant CPAP by adding gas flow at whatever FiO2 is set on the ventilator. NIV devices that I am familiar with all behave this way.
Thanks for the information. Where I trained (Australia and UK) we have always prexoygenated with BVM. The cited superiority of high flow NRM over BVM actually refers to an abstract on the internet and the article written by Dr Weingart (1) does state without reference that standard flow meters are capable of achieving very high flows in the order of 30-60 l/min if dialled right up. The data presented in the reference (abstract form on net) shows NRM achieving 77-89% at 30-60l/min respectively (and not greater than 90% as stated). Iis there any data to support these higher flow rates… Read more »
Today I had the opportunity to visit our biomedical equipment division. I tested a standard (15l/min) flow meter with a Fluke VT mobile gas flow analyzer. The calibrated flows on the wall flow meter were accurate. When the valve was fully opened past 15 l/min it only generates a maximum 19l/min flow.
May be the flow meters are different pressures in the USA ( I work in Australia). But the flow meters I checked would not produce the required flow rates to achieve FiO2 > 90% with NRB mask alone.
Is there a benefit to using the nonrebreather on its own at 30-60 lpm as opposed to using the nonrebreather at 15 lpm plus the use of nasal cannula to the max? I’ve been reading Dr. Levitan’s NO DESAT material, which recommends nonrebreather plus nasal cannula…
thanks!
The NRB should ALWAYS be put up as high as your flowmeter will allow. NC adds little to this, but there is no reason not to put it on at 15 lpm right at the start if you have enough flowmeters. When using oxygen tank (limited to 15 lpm) with the NRB, there is prob. an advantage to NC in addition. Dr. Levitan was my co-author on the paper recommending always try to get 30-40 lpm with NRB.
I have read your articles referenced above including the joint article with Levitan and they were excellent. question re Pre-Ox: – While the patient is spontaneously breathing before you push your drugs? What is the advantage of using the NRB mask over the BVM with good seal? If the patient is taking adequate breaths surely the NRB is delivering higher FiO2 unless you have flow valves that open up to 30L-60L per min where they may be equivalent? So essentially I’m trying to figure out when NRB mask is going to be better than NRB with good seal (not just… Read more »
most BVMs provide only room air to spont. breathing pts as the exhalation valve is where they are exchanging gas. even in the rare, more expensive bags that have a 1-way valve on exhalation, you need to maintain perfect seal for high fio2.
NRB provides nothing in apnea and we remove it.
thanks Scott -1 follow up questions to help me get my head around this and 2 others: 1. So because BVM’s exhalation port does not have 1 way valve then during spontaneous breathing entrain a mixture of room air through this port and 100% 02 from the bag through the inspiratory port (that opens through the negative pressure of the spontaneous breath. With the NRB you are also getting a mixture of entrained air from room air (through the holes on the mask) and 100% O2 through the reservoir. So why then does the NRB provide the patient much better… Read more »
1. Only room air, nipple on insp doesn’t open
2. Not necessary unless deformed anatomy
3. No
But it depends on the BVM type, no?
Grauman S, Johansson J, Drevhammar T. Large variations of oxygen delivery in self-inflating resuscitation bags used for preoxygenation – a mechanical simulation. Scand J Trauma Resusc Emerg Med. 2021 Jul 19;29(1):98. doi: 10.1186/s13049-021-00885-3. PMID: 34281616; PMCID: PMC8290536.
what depends on BVM type
I mean if you use a BVM device with a exhalation port 1 way valve (or with a peep valve attached) and you maintain a good seal, the patient will get a high Fi02 from the BVM breathing himself (not squeezing it al all)
yes–that is the entire point made here
Scott, when using the NRB for PreOx prior to intubation, can you substantially improve your Fi02 by taping the expiration ports that are NOT covered with 1 way valve. I understand these ports without valves are there to prevent suffocation in the event your oxygen runs out. However if you are only using this NRB temporarily for 3 minutes with you continuously attending the patient prior to intubation to improve FiO2 the benefits would probably outweigh the risks.
What are you thoughts? Have you tried this?
I can’t recommend this b/c of safety concerns, but yes it increases FiO2. You can just steal a gasket off another mask as well.
Have you had much experience with the Mapleson C devices for preoxgenation. Apparently quite good but needs some additional training to use in respect to setting the oxygen flow rate and the bag not being self inflating. Also useful for manual ventilation, can provide PEEP and can allow you to feel the compliance of lungs. Also makes it easy to provide gently manually supported spontaneous breaths as can feel when patient inspires. Compared with BVM and NRB seems like the only device that can easily be used in ED for BOTH spontaneously breathing Preox AND manually ventilating Reox. I wonder… Read more »
Only seen pictures. I’d still prefer BVM with a PEEP valve which along with a nasal cannula provides preox, reox, and apox with 100% fiO2 and self-inflation of the bag.
sure. Though since you’ve opened my eyes to this BVM issue, I do wonder though if the BVM even with PEEP valve is really giving the patient 100% Fi02 if there are even small leaks around the mask. I haven’t yet tested with the PEEP valve but do have some BVM’s with a one way valve on the expiratory port (they must be affordable here as my dept has a bunch of disposable ones) and I wonder whether the patient is getting much ventilation with spont breaths given how much effort is required to open the inspiratory valve – tried… Read more »
Obviously as you describe nasal cannula assist during ApOx.
However during the PreOx phase, if you use a NRB with O2 flow turned up to max above 15L/min 02, does the addition of Nasal Cannula even at 3-5L/min increase your FiO2 significantly? The semi awake patient may only tolerate those type flows from Nasal Cannula before pushing sedation so wondered if this is improving FiO2 by creating an O2 reservoir in the pharyx (at the end of expiration just before inspiration). Do you know of any research demonstrating an increase in FiO2 with such a NRB + Nasal Cannula combo?
I personally don’t believe ti does anything over a maxed out (40lpm) NRB. Rich does believe it adds to fiO2. No research that I know of.
I understand the PAP, but when you demonstrated the BVM/PEEP with the NC, you had a change in pressure. You were showing a pressure of approx. 5 cm/H2O on inspiration and 10 cm/H2O on expiration. So why would this not be considered BiPAP? This would be very handy in EMS where access to BiPAP is limited due to equipment cost.
I presume it is CPAP where due to your equipment you are not getting less than ideal pressure provided in inspiration i.e the inspiratory pressure is less than the expiratory pressure instead of being the same. Effectively it is PEEP with a little of pressure during inspiration as well (provided by adding the continuous oxygen flow via the nasal cannula).
BIPAP would have a greater inspiratory pressure than expiratory pressure i.e the 10 and 5 would be the other way round.
Ok, I understand, now. Thank you.
A question from a basic level provider (asking for educational reasons).
Is the use of a peep valve for re-oxygenation (or BVM ventilation if the pt is hypoxemic on high FiO2) still safe in PTS with a head injury w/ suspected increased ICP?
I’m not a neuro guy (and am not an als/ccp provider) so I don’t know if the possible negative effects PEEP has on the CPP (CPP=MAP-ICP) outweigh the need to oxygenate the pt.
Scott,
I’ve been using pre-oxygenation via NC since I heard you talk about it – but I keep running into a “Style-point” roadblock – the RT’s always want to argue about the flow rate on the NC, saying it “can’t deliver above 5L…” I tried to explain the difference between apneic oxygenation and the actively breathing person to no avail. Are there any quick explanations you could offer? Maybe an in-service is indicated.
here you go Chest. 2013 Oct 1;144(4_MeetingAbstracts):890A. Apneic Oxygenation via Nasal Prongs at 10 L/min Prevents Hypoxemia During Elective Tracheal Intubation. Christodoulou C, Mullen T, Tran T, Rohald P, Hiebert B, Sharma S. Abstract SESSION TITLE: Ventilatory Strategies in Severe Hypoxemia SESSION TYPE: Original Investigation Slide PRESENTED ON: Wednesday, October 30, 2013 at 07:30 AM – 09:00 AM PURPOSE: Hypoxemia during airway management remains an important cause of morbidity and mortality. Oxygenation during intubation via nasal prongs may prevent critical desaturations (Anesthesiology 1988, J Korean Med Sci 1998). We evaluated the effectiveness of oxygen administration via nasal prongs during apneic… Read more »
Scott,
When you see the O2% bumping up from say, 90% range all the way up to 100% just by adding 5cm/h20 of CPAP (obviously maxed at 100 % FIO2).. do you go up to 10 on CPAP- or all the way up to 15 on CPAP, since we want to optimize Pao2, and 100% could mean Pao2 of 90 or… 400?
Nah. The yield from raising PaO2 is virtually nil. All the gain is from maximal saturation of Hb, maximal recruitment of alveoli, and maximal denitrogenation.
Hey Scott, It seems as though whether Pa02 truly directly feeds the hemoglobin saturation directly, or if it’s just a marker of optimization of the things you speak about (alveolar recruitment, de-nitrogenation, etc.), higher PaO2 levels appear to correlate with and are associated with a longer safe-apenic period. This was a small study but just an example: http://www.ncbi.nlm.nih.gov/pubmed/8564655 Therefore, it seems additional increases in CPAP(PEEP), (in pts refractory to 100% supplemental O2) may be a valuable method of increasing the safe apenic period, by increasing PaO2 to higher levels despite a pulse ox of 100% at a given lower level… Read more »
Dear Scott, In trying to wrap my head around the concept of bag-valve mask ventilation and PEEP, I ask if you could please just follow my logic and way of thinking and see where I may be losing any concept, or where my logic may be going stray… I mentally break down the entire cycle into 3 parts: 1. Inspiration 2. Expiration 3. *the period between breathes 1. Inspiration- When the patient takes a breath, I would assist his/her ventilation by gently squeezing the bag with a tight seal, and therefore supplying PEEP during inspiration. 2. Expiration- During expiration, by… Read more »
Flow is everything. Normal insp flow is approx 40 l\m, coming out of a Flow meter one can achieve upwards of over 100 l\m with the knob turned OPEN, clearly meeting or EXCEEDING normal insp flow to achieve 100% 02 DELIEVERED prior to intubation via a MASK, the use of a nasal cannula at 15 l/m during intubation would then AUGMENT any 02 HgB saturation gain with this mask. To me this is the QUICKEST and SIMPLEST way to achieve the GOALS of no or minimal desaturations and buy some extra TIME for intubation and avoid the possibility of aspiration… Read more »
A NC at 10 Lpm will provide only 1 cmH20 of cpap. This is why Nasal High Flow Cpap works so well. If you are giving the patient 60 Lpm, they are getting 6 cmH20 of Cpap. I use NHF all the time where I work at for many issues and it’s a standard practice to have a patient on 60-to-50 Lpm and 100%-to-35% of Fi02.
J.Toto, BS, RRT, EMT-P
Dr. Weingart,
At my ED, the RTs pre oxygenate using an anesthesia bag mask, not a self inflating bag mask. Is there literature looking at the actual FiO2 delivery (or end tital O2 achieved) using anesthesia bag mask vs nonrebreather mask? I cannot find any actual data on this.
Thanks for all your great work
Mike Miescier
Pediatric EM physician
Salt Lake City, UT
super cool pod, scott
Hey Scott
I saw that you linked our AJEM study that NC doesn’t increase NIV mask leak- our followup study showed that NC at 15 LPM doesn’t significantly affect pre-ox with NIV. Although I just saw the other study showing that NC flow rate matters when using it underneath BVM- not a surprise to be honest.
https://www.ncbi.nlm.nih.gov/m/pubmed/30037519/?i=2&from=end%20tidal%20oxygen%20saturation
just linked to your new one as well–great work
Hi, dr. Scott, I know that this is an old article and I have been using things that you wrote here with great results. But I have never tried a CPAP for pre-Ox before. If I recall it right, I think I read in the comment section where you advise to use CPAP concurrently with NC 15 lpm? I don’t really get it. What is the purpose of the NC here? Why not just set the FiO2 to 100% in the CPAP machine? Thanks
Can you explain how placing nasal cannula flow rates force the duckbill valve open to create this PEEP? The duckbill is an inspiratory flow valve, no? Is the BVM providing any passive airflow/oxygenation? As in, if I intubated a patient and just placed a BVM and set the flow to 15Lpm, will any of that flow get to the patient for apneic oxygenation? Thank you!