Introduction
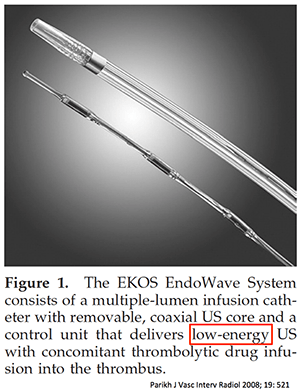
Ultrasound-assisted catheter-directed thrombolysis is increasingly popular for submassive PE. This involves placement of a catheter into one or both pulmonary arteries which infuses alteplase and also vibrates ultrasonically. The combination of localized alteplase and vibrational energy is intended to disrupt the clot. Unfortunately, the actual mechanism of action of this therapy remains unclear.
Ultrasound-assisted catheter-directed thrombolysis works
The only RCT investigating ultrasound-assisted catheter directed thrombolysis (CDT) was ULTIMA, which proved that it reduced pulmonary pressures, compared to heparin which did not. Subsequently eight uncontrolled studies have been published, which paint a reasonably consistent picture (table below)(1). Patients generally received about 25 mg of alteplase, usually via bilateral catheters in both pulmonary arteries. Although some bleeding complications occurred, there were no cases of intracranial or fatal hemorrhage (0/537 patients).
 Mean pulmonary artery pressure (mPAP) decreased by an average of 9 mm. This is significant. For example, pulmonary hypertension is defined as mPAP > 25mm. A normal heart can generate a mPAP up to about 40 mm, beyond which it fails. Therefore, the difference between a normal mPAP (24 mm) and a mPAP causing cardiac arrest (~40mm) may be as little as ~15 mm.
Mean pulmonary artery pressure (mPAP) decreased by an average of 9 mm. This is significant. For example, pulmonary hypertension is defined as mPAP > 25mm. A normal heart can generate a mPAP up to about 40 mm, beyond which it fails. Therefore, the difference between a normal mPAP (24 mm) and a mPAP causing cardiac arrest (~40mm) may be as little as ~15 mm.
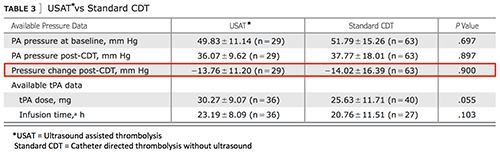
The table below compares average hemodynamic improvements observed with ultrasound-assisted CDT versus improvements observed with systemic thrombolysis (2). Ultrasound-assisted CDT appears to be effective.

Why does ultrasound-assisted CDT work?
Although ultrasound-assisted CDT is a single intervention, it contains roughly three components:
- [1] ultrasonic energy
- [2] effect of local delivery of alteplase
- [3] systemic effect of ~25 mg alteplase (regardless of where it is infused)
The remainder of this post will explore evidence regarding these components.
[#1] Ultrasonic Energy
 Ultrasonic energy augments thrombolysis in laboratory studies, but it doesn't seem to work clinically. This may reflect limitations on the amount of energy which can be delivered without overheating the catheter.
Ultrasonic energy augments thrombolysis in laboratory studies, but it doesn't seem to work clinically. This may reflect limitations on the amount of energy which can be delivered without overheating the catheter.
Engelberger 2014 performed the only RCT available on ultrasound-assisted thrombolysis. These authors studied 48 patients undergoing catheter-based thrombolysis for DVT. All patients underwent placement of an ultrasound-assisted thrombolysis catheter and were treated with a slow infusion of 20 mg alteplase via this catheter. Patients were randomized as to whether or not the ultrasonic energy in the catheter was turned on. Reduction in clot size was identical regardless of whether ultrasonic energy was used (55% vs. 54%).
More recently, the PERFECT registry described 100 patients who underwent catheter-directed thrombolytic infusions for PE. Most patients (64%) were treated using CDT without ultrasound, with the remainder receiving ultrasound as well. There were no differences in the reduction in pulmonary pressures between the two groups:
 [#2] CDT without ultrasound: What is the theoretical rationale?
[#2] CDT without ultrasound: What is the theoretical rationale?
Over the years, CDT without ultrasound has been attempted in a variety of diseases (e.g. MI, stroke). This has intuitive appeal, but little theoretical justification in PE.
Targeting pulmonary emboli is easier said than done
CDT makes the most sense for MI or CVA, where there is often a single thrombus causing a single culprit lesion. Alternatively, patients with severe PE typically have multiple lesions distributed throughout the pulmonary circulation. This raises a question of how it is possible to provide “directed” therapy to numerous target lesions.
~85% of patients in recent trials of CDT have had catheters placed into both pulmonary arteries to treat bilateral emboli. However, because the lungs receive 100% of the circulation, the average drug concentration in the lungs will be identical regardless of whether drug is infused peripherally or via bilateral pulmonary artery catheters.
 CDT might improve therapy if placing the catheter next to a prominent clot increases the local concentration of alteplase. However, blood flow through an occluded pulmonary arterial system is fast and turbulent, so the alteplase doesn't stay still. Studies in dogs have demonstrated that thrombolytic released adjacent to a clot is rapidly whisked away, sometimes winding up in the contralateral lung (Schmitz-Rode 1998).
CDT might improve therapy if placing the catheter next to a prominent clot increases the local concentration of alteplase. However, blood flow through an occluded pulmonary arterial system is fast and turbulent, so the alteplase doesn't stay still. Studies in dogs have demonstrated that thrombolytic released adjacent to a clot is rapidly whisked away, sometimes winding up in the contralateral lung (Schmitz-Rode 1998).
Flow studies explain why thrombolytic agents administered via a catheter positioned adjacent to the embolus may have no more effect than systemically administered agents. –Schmitz-Rode 1998
Current techniques try to solve this problem by attempting to embed the catheter within the clot and infuse thrombolytic directly into the clot. However, these catheters have multiple side-ports, so thrombolytic may preferentially flow through unobstructed side-ports lying outside of the clot.
Catheter-directed thrombolysis ignores the significance of recirculating thrombolytic
CDT focuses on maximizing the first-pass effect of alteplase. This could make sense when performing CDT in a coronary artery, because the alteplase is diluted substantially prior to recirculation.
PE is different. For a patient receiving alteplase infusions into both pulmonary arteries, the average drug concentration in the lungs is equal to the subsequent systemic drug concentration. After flowing through the lungs, alteplase is sent to the systemic circulation and then it immediately returns to the lungs. All alteplase molecules remaining in circulation will keep circulating through the lungs over and over.
Re-circulating alteplase may play a greater role than the first-pass effect. The half-life of alteplase in the blood is ~4 minutes. Meanwhile, the time required for alteplase to pass through systemic circulation and return to the lungs may be roughly one minute (3). If alteplase re-circulates through the lungs every minute and levels fall with a half-life of 4 minutes, then the effect of recirculation may be estimated:
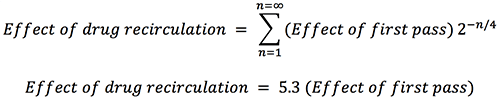 This is a crude estimate, but it illustrates how recirculating alteplase could have a dominant effect on thrombolysis. If recirculation were more important than the first-pass effect, then the site of infusion would be irrelevant.
This is a crude estimate, but it illustrates how recirculating alteplase could have a dominant effect on thrombolysis. If recirculation were more important than the first-pass effect, then the site of infusion would be irrelevant.
[#2] CDT without ultrasound: Clinical evidence
![]() This isn't the first time there's been excitement about CDT for PE. There was interest in CDT in the 1970s-1980s, with several uncontrolled studies showing it to be effective. Eventually, an RCT was performed in 1988 comparing CDT to an equal dose of alteplase via peripheral vein. Alteplase was equally effective regardless of where it was infused (Verstraete 1988). This study debunked CDT, which remained unpopular until the invention of ultrasound-assisted CDT. Newer catheters may be more effective than catheters used in the 1980s, but this has yet to be tested in an RCT.
This isn't the first time there's been excitement about CDT for PE. There was interest in CDT in the 1970s-1980s, with several uncontrolled studies showing it to be effective. Eventually, an RCT was performed in 1988 comparing CDT to an equal dose of alteplase via peripheral vein. Alteplase was equally effective regardless of where it was infused (Verstraete 1988). This study debunked CDT, which remained unpopular until the invention of ultrasound-assisted CDT. Newer catheters may be more effective than catheters used in the 1980s, but this has yet to be tested in an RCT.
Gaba 2014: Thrombolysis via a Swan-Ganz catheter
This study is strange but interesting. It describes 19 patients with submassive PE treated with alteplase infused at 0.5-1 mg/hr via a Swan-Ganz catheter. In 17/19 cases the pulmonary emboli were located bilaterally, but alteplase was infused unilaterally into one pulmonary artery. Patients underwent daily pulmonary angiography, with continuation of thrombolysis until pulmonary artery pressures and symptoms resolved. If angiography showed clearance of clot on the same side as the pulmonary artery catheter but residual clot on the contralateral side, then the catheter was re-positioned onto the other side.
Success was achieved in 18/19 cases, with complete or near complete clot dissolution (the remaining patient died from an intracranial hemorrhage (4)). Catheter repositioning to the contralateral lung was performed only in four cases. This study proves that infusing alteplase unilaterally can achieve resolution of bilateral pulmonary emboli, suggesting that CDT isn't a precisely targeted therapy.
[#3] Systemic effect of ~25mg alteplase
Patients treated with ultrasound-assisted CDT usually receive ~25 mg alteplase (“quarter-dose”). This may have a greater systemic effect than is commonly appreciated. For example, four case reports describe success using slow infusions of peripheral 25 mg alteplase in PE patients at high risk of hemorrhage (5). Boone 2011 published a series of four patients who developed intra-operative pulmonary emboli which responded to tiny doses of alteplase (0.5-4 mg).
Aykan 2014 reported the effect of 25 mg alteplase administered peripherally over six hours to 27 patients with massive PE. This was a high-risk patient group, most of whom were over seventy years old. However the results were favorable, with no major hemorrhage or in-hospital mortality. Alteplase caused an impressive 23 mm drop in the pulmonary artery systolic pressure (from 57 +/- 8 mm to 34 +/- 3 mm)(6).
Additional data about the systemic efficacy of slow quarter-dose thrombolysis comes from patients with thrombosed prosthetic heart valves. Prosthetic valve thrombosis is similar to PE because it occurs in a central location, which receives 100% of the cardiac output. Slow peripheral infusion of 25 mg alteplase has been shown to be effective (Ozkan 2013).
Conclusion: Why does ultrasound-assisted CDT work?
 Understanding why ultrasound-assisted CDT works seems like peeling away layers of an onion, with each layer bringing us closer to the truth. The outer-most layer is ultrasonic energy, which isn't supported by the only RCT testing it. The next layer is CDT without ultrasound, which likewise was ineffective in the only RCT testing it. Its theoretical basis is also questionable. Ultimately, we are only left with the systemic effects of quarter-dose alteplase, which has proven efficacy and probably is the main mechanism behind all of these therapies.
Understanding why ultrasound-assisted CDT works seems like peeling away layers of an onion, with each layer bringing us closer to the truth. The outer-most layer is ultrasonic energy, which isn't supported by the only RCT testing it. The next layer is CDT without ultrasound, which likewise was ineffective in the only RCT testing it. Its theoretical basis is also questionable. Ultimately, we are only left with the systemic effects of quarter-dose alteplase, which has proven efficacy and probably is the main mechanism behind all of these therapies.
Mechanism of action matters. For example, the PERFECT study concluded that ultrasonic energy was expensive and nonbeneficial, so CDT without ultrasound should be used. If CDT without ultrasound were also unnecessary, this would imply that similar benefits could be obtained with a slow peripheral infusion of quarter-dose alteplase. Administering alteplase peripherally could allow thrombolysis to be started sooner, achieved noninvasively, and be widely utilized in any hospital.
Stay tuned, this is the first of a two-part series on submassive PE.
Related links
- Choosing your poison: thrombolysis vs. heparin
- Resus: The crashing PE patient
- Other stuff
- EKG patterns of PE that mimic MI (PulmCrit)
- What is the evidence behind the IVC filter? (PulmCrit)
References
- References for this table: ULTIMA, SEATTLE II, PERFECT, Engelhardt 2011, Kennedy 2013, Dumantepe 2014, McCabe 2015, Engelberger 2015, Bagla 2015.
- It is difficult to make direct comparisons between different studies, because the effectiveness of any intervention will vary between populations (e.g. depending on the initial severity of pulmonary hypertension, time delay to therapy). Other variables limiting comparability include different time-points selected and different methods used to determine pulmonary artery pressures. References for this table: Meyer 1992, Meneveau 1997, Meneveau 1998, Tebbe 1999, Becattini 2010, Wang 2010, Sharifi 2013, Sharifi 2014
- Estimated based on ~4 liters blood volume divided by ~4 liters/minute cardiac output.
- The episode of intracranial hemorrhage occurred in a patient who had received relatively little alteplase, had normal fibrinogen levels (386-486 mg/dL), but had uncontrolled PTT values on a heparin infusion (with elevation of PTT > 200s). The authors attributed this intracranial hemorrhage to supra-therapeutic heparin infusion, rather than a consequence of alteplase infusion. This is consistent with my experience and interpretation of the literature, specifically that alteplase alone is fairly safe but the combination of alteplase with titrated heparin infusions can be dangerous.
- References are: Yildiz 2013, Biteker 2010, Sen 2014, and Aykan 2014.
- Unfortunately this study currently is only available in abstract format: Aykan AC et al. Low dose prolonged infusion of tissue type plasminogen activator therapy in massive pulmonary embolism. European Heart J 2014; 35(Suppl 1): 69.
- The PEITHO trial is often held up as an example of the bleeding risks of thrombolysis. However, it must be noted that patients in this trial were simultaneously treated with full-dose tenecteplase and loading boluses of heparin. This is probably inadvisable under any circumstance. The PEITHO trial is discussed further here.
Image credits: Opening image: Inception (Warner Brothers). White water rapids: en.wikipedia.org/wiki/Whitewater.

- PulmCrit Wee: Rational selection of infusion rate based on loading dose - June 25, 2024
- PulmCrit: PPIs are safe and effective for GI prophylaxis… the end. - June 18, 2024
- PulmCrit: Bilevel Sequence Intubation (BSI) – The new standard - June 17, 2024
Ok, so we may be getting somewhere. If you can give a dose of thrombolytic that causes near zero number of “serious” bleeding complications and still significantly decreases the mPAP in the all-too familiar “sub-massive” PE cases you may gradually bring some of the “First Do No Harm” camp to the other side. It was always difficult for me to justify giving a thrombolytic in a relatively hemodynamic patient, especially when I can always decide to lyse someone later if there is evidence of decompensation. The next hurdle is going to be getting people to give alteplase and potentially NOT… Read more »
Thanks. The heparin bit is very tricky. There isn’t evidence that heparin helps acutely, but at the same time there isn’t much evidence that it’s safe not to give heparin either. For patients who are getting full-dose or half-dose alteplase (i.e., 50-100 mg alteplase over 2 hours), my preference is to avoid heparin for ~12 hours (and to avoid heparin boluses for at least 24 hours). This isn’t based on hard clinical evidence. These alteplase doses cause substantial changes to the coagulation system which favor hemorrhage (e.g. fibrin degradation product coagulopathy), so I think it’s reasonable to hold heparin for… Read more »
Thanks so much for the great breakdown of the research. I’ve seen/heard some data on 50mg vs 100mg, but hadn’t seen the 25mg low dose study before. Very interesting stuff. We typically would hold heparin until 12 hours post lytic in our institution, but it definitely seems unnecessary (if infusing the lytic for 24 hrs) to be infusing heparin concurrently.
Thanks again!
Don’t discount the reimbursement part of the equation. My understanding is that placement of bilateral EKOS catheters is fairly lucrative (roughly the equivalent of me seeing 4-5 critically ill patients). It will be interesting to see if insurance companies drop the reimbursement some and if that has any effect on its “increasing popularity”.
I don’t understand what “Mean pulmonary artery systolic pressure (mPASP)”. In my book a pulsed pressure can be systolic, dialostic or mean, but not ‘mean’ and ‘systolic’ at the same time…
“For example, pulmonary hypertension is defined as mPASP > 25mm.” Again, mPAP would make this phrase correct, but a ‘mean systolic’ as expressed by mPASP doesn’t exist…
Agree. I meant to write “mean pulmonary artery pressure” rather than “mean pulmonary artery systolic pressure.” I have corrected it above. Thanks for pointing this out.
Thank you for this interesting article. The obvious fact that there is a 100 % passage thrue the lungs of any drug you give intravenously came to me first when I read some article about the low dose trombolysis for PE. That is kind of embarrassing. For me there is always the question if a trombus in the lung is always receptible for trombolysis, that means if it is not already some kind of a ”stable” old clot. I´ve met some patient with at least submassive PE that had symptoms for weeks. Do they have symtoms because of any new… Read more »
I think there is a reasonable amount of evidence that lysing patients with submissive PE improves functional outcomes. The best single study in this regard is TOPCOAT (discussed here: https://emcrit.org/pulmcrit/submassive-pe-are-we-treating-it-backwards/). There are also a number of observational/correlational studies which show that: (1) lysis causes persistent reductions in pulmonary pressures compared to heparin, and (2) patients with persistent pulmonary hypertension are more likely to have exercise limitation/reduced quality of life. A patient presenting with submassive PE has a one-time oppertunity for pharmacologic lysis. If lysis isn’t performed and the patient progresses onward to develop chronic thromboembolic pulmonary HTN, then the only… Read more »
Josh,
What is your feeling on the safest route for a patient who syncopized from their saddle and smashed their nasal bone. Def. submassive, occ. drops in BP. Head CT normal. Options are systemic lytics, IA lytics, angiojet, angiovac, surg embo, just heparin. What would you do based on your research of complications.
Tough situation. The first thing to realize is that any course of action is going to involve a risk of mortality or severe morbidity (ie ICH). We can try to minimize this as much as possible, but it’s probably impossible to drive this risk below a certain level (perhaps 5% in this patient). This reminds me of a case at Genius General involving a patient with submassive PE who syncopized and hit their head, without fracture but with a sizable goose-egg. Due to concern about the risk of intracranial hemorrhage the patient was treated with heparin. The patient went on… Read more »
Why catheter directed and not just thru a PIV?
Josh, Thanks for another outstanding review. I’m wondering your thoughts about the new ACCP VTE guidelines, which take a pretty dubious stance regarding thrombolysis for anything but massive PE, and whether they will influence your practice. Clearly there’s sound physiologic rationale; having a lower PA pressure seems better than having a higher one. Similar logic with lower versus higher clot burden. Our group remains concerned about the lack of data demonstrating improvement in any patient-centered outcome (as you mentioned, Kline’s TOPCOAT study comes closest, but it’s a bit concerning that it was terminated early) and signals of harm from the… Read more »
Thanks, Nick. I feel that the ACCP guidelines are oversimplified and insufficiently aggressive. For example: – All thrombolytics aren’t created equal. There may be a significant difference betwen full-dose tenecteplase boluses with therapeutic heparin (as in PEITHO) versus 50 mg alteplase without heparin. – I usually don’t prefer the wait-and-lyse approach (i.e. admit for observation and lyse if the patient deteriorates). Patients may deteriorate and arrest rapidly, before lysis is possible. Also, patients may arrest after >24 hours observation and transfer to the floor (have seen this). The best solution may be to find a pro-active, safe, and controlled way… Read more »
I just saw this trial come up and thought of this post. Can’t wait to see the results when it comes out.
“Peripheral Low Dose Thrombolysis Versus Catheter Acoustic Directed Thrombolysis for Submassive PE”
EKOS vs Peripheral IV 2mg/hr
https://clinicaltrials.gov/ct2/show/NCT03581877
Have you seen any other interesting papers about peripheral tPA in PE, or has your practice changed much recently?
oh boy oh boy oh boy oh boy oh boy
Have been waiting for this study for years.
Kudos in advance to the authors, let’s pray that it doesn’t get stopped prematurely.