
🙏Post peer reviewed by Dr. Cederic Pimentel (@CajalButterfly) 🦋🦋🦋
A while ago I put a poll on Twitter:

I really assumed we were all on the same page here. (Yes, I know all the meta-analyses show they have the same efficacy, but…) I thought everyone would agree PLEX is the way to go. I think of this like Starbusts. They are all just flavored corn-syrup, but … we all know – the pink one is best.

(That this box plot exists in the world is incredible, source. Also, I agree red is second best, but then orange? Really? No. Orange is last.)
So, imagine my surprise with these results:

More people would want IVIG! 🤯 Obviously, this led me down a rabbit hole of examining my own biases and going back to the data – a post about what this deep dive revealed:
- Mechanisms of IVIG and PLEX
- IVIG and PLEX in Guillain-Barre Syndrome
- What if Patients aren't Getting Better?
- Complications and Considerations for IVIG and PLEX
Intravenous Immunoglobulin: This is a preparation of polyclonal serum IgG pooled from thousands of blood donors. IgG molecules have the “Fc” portion and the “V-shaped” Fab portion:
🥊 The Fab portion is responsible for neutralization of cytokines, complement and autoantibodies. Thus, this portion halts potent pro-inflammation pathways.
🥊What about the Fc portion though? This portion binds to cellular receptors (RcyF and RcRn). Activation of these receptors trigger immune response. It is hypothesized that by binding to these sites IVIG prevents the binding of the pathologic autoantibodies.
🥊Exactly how this happens is complicated and somewhat still hypothesis, but there’s a nice explanation here (PMID: 25561275)
🥊IVIG was never tested against placebo for GBS. It was compared to PLEX.
Therapeutic Plasma Exchange (PLEX/TPE): A large volume of whole blood is taken from the vein and filtered or centrifuged into various parts. The plasma is discarded. In the States, the approved PLEX machines use centrifugation.
🥊The rest of the blood is replaced back into the circulation usually with 5% albumin or a cystralloid/colloid solution.
🥊This works by removing the pathogenic antibodies in the blood.
🥊There is a concern that once PLEX is stopped the synthesis of auto-antibodies to myelin and peripheral nerves may rebound (PMID: 1898263) although this has not been shown in large studies
🥊PLEX is the OG treatment for GBS. It was proven efficacious in shortening the duration of disability compared to conventional therapy (mainly steroids, which were standard of care at the time) in 1985 in this study
The first major trial of IVIG vs PLEX was published in NEJM by the Dutch GBS Group. The median time to improvement by one grade was 41 days with plasma exchange and 27 days with immune globulin therapy (P = 0.05). Given these results, this larger trial was published in The Lancet in 1997:
379 patients were randomized within 11 countries over 38 centers. Patients had to have an acceptable clinical and CSF profile and had severe disease (at least required assistance to walk).
👉Patients either got 5 rounds of plasma exchange (~50cc/kg exchanges each session, total ~250cc/kg exchanged) – a process which took 8 to 13 days
👉Or got 5 infusions of IVIG (totaling 2g/kg. 0.4g/kg day x 5 days).
👉Or got PLEX followed immediately by IVIG (regardless of degree of improvement to that point)
Randomization:
- The average delay from onset of neuropathy to randomization was about 6.5 days in both groups
- 24% of pts in the PLEX group vs 18.5% in the IVIG group had preceeding enteritis.
- Remember, enteritis (often campylobacter jejuni) is associated with axonal variant of GBS, which has a worse prognosis.
Outcomes:
- There was no statistically significant difference in
- The time to recover walking
- The time to discontinuation of the ventilator
- For mechanical ventilation: the patients in the single treatment arms were on the vent for about a month (26 days vs 29 days).
- PLEX was not universally well tolerated. 14% of pts in the PLEX arm got <75% of their planned doses
🤔In this paper, patients with long delays in starting treatment recovered faster.
This is probably explained by two things:
1️⃣ The patients enrolled late were already starting to get better.
2️⃣ Alternatively, those who had rapidly progressing disease likely came to medical attention more quickly. Rapid progression (discussed as length of prior illness) is associated with prolonged recovery (PMID: 3382169). Graph ⬇️ showing probability of reaching ability to walk independently.

Black dots are short onset of disease; white are long. Dashed lines are those treated with PLEX.
- This happens frequently! Most patients reach their maximal disability at 2 weeks and then reach a plateau phase (PMID: 31541214). Many times, patients continue to have progressive weakness through the treatment. (I warn patients/families of this possibility).
- Mulitple studies have demonstrated that about 40% of patients treated with standard IVIG and plasma exchange do not improve in the first 4 weeks (studies summarized here: PMID: 27837102)
- Progression despite treatment does not mean that treatment has failed. (There likely would have been more significant progression without treatment!)
- But still, when patients aren't getting better, it is hard not feel antsy. What about switching treatments? What about both? What about more of the same? A look at the options:
Question 1: Can I use both treatments– PLEX and then IVIG?
In the Lancet study there was a group that got PLEX followed by IVIG.

In this group, the number of median vent days was 18 days (vs 26 or 29 in the single therapy arm), which seems like a meaningful difference, but it did not reach statistical significance. We may at some point determine a subgroup that does benefit from this treatment strategy, but currently, that hasn't been answered. But, we do know there are risks and costs associated with each treatment. For now, PLEX followed by IVIG does not have a significant benefit.
Question 2: What about more of the same?
- Similarly, more is not better. In this trial of trial of IVIG + a second round of IVIG, a second round of IVIG was associated with a signal of harm.
Question 3: PLEX after IVIG – what about that?
- There is less trial data here, but the way that PLEX works, you’d be removing the treatment you just paid to give. A retrospective study found no association between PLEX after IVIG and improved short-term outcomes of patients with Guillain-Barré syndrome, but there was an association with an increase in cost and duration of hospitalization (PMID 21386771)
From the largest trial, there is not overwhelmingly convincing evidence that even in critical illness one is better than the other, but:
- The side effect profiles are different.
- There is a difference in cost
- There is difference in the ease of administration
Side Effects and Dosing Considerations:

1: PMID 31300488 // 2: the spiral of angioedema // 3. PMID 31300488 // 4. PMID: 32445106// 5. PMID: 29443413 // 6. PMID: 27630072

1: PMID: 16391392 // 2. PMID: 15186194
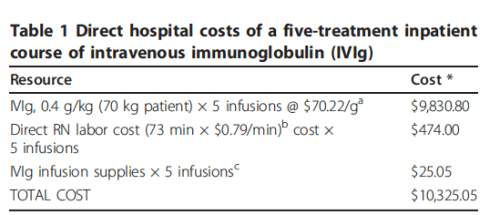
Cost:
It’s really hard to find exact costs and to take into account insurance reimbursement etc.
But one study did look into 💸 about 10 years ago. PMID: 21575219

Ease of administration:
This came up a lot in the poll discussion. IVIG does not require a vascular access catheter and does not require involvement from the blood bank. I can certainly understand when a patient is floor-status that getting central access can be a challenge. Several people commented that it just takes too long to set up.
I hear that. Two thoughts —
🎉PLEX can be done peripherally. In fact, in the major trial of Myasthenia Treatment (IVIG vs PLEX), PLEX was done through peripheral access with very few adverse events (PMID: 23322564)
🎉Is Time Nerve (PMID 27837102)? Unclear. In the early trials demonstrating efficiency, PLEX just had to be started within 72 hours of enrollment (PMID 3382168) and was shown to be most effective in treating patient if started within 7 days of onset of symptoms (PMID: 4022342). So, sooner treatment does seem better. However, in GBS what we term “rapid reversal” is over weeks instead of the usual months. Since the goal of either IVIG or PLEX is to shorten the duration of disability over months, I’m not sure that hours or maybe even a day of treatment delay to set up the treatment makes a difference in promoting the long-term recovery. There is no hard evidence in this respect. Personally, I feel ok about getting the catheter in on day 1 and starting PLEX day 2.
Summary:
✅ IVIG ⚔️ PLEX gets you the same outcome. The patient may get worse during the treatment and that does not mean the treatment has failed. Choose one treatment, stick with it unless complications, and counsel the patient that recovery really takes weeks to months.
-
- Note: You can calculate your patients risk of inability to walk independently at 4 and 26 weeks using the mEGOS score.
✅ PLEX and IVIG have different side effects. Know what to watch out for!
[I still like PLEX better, I just now realize that that preference isn’t evidenced based.🤷🏻♀️]

- NeuroEMCrit – 31 #NeuroPostItPearls - August 22, 2022
- NeuroEMCrit – IVIG 🆚 PLEX - May 3, 2022
- NeuroEMCrit – Does Vent Over-Breathing Always Disqualify Brain Death Testing? - December 27, 2021
Really enjoying the neuro focused blogs, it’s definitely a weak point of mine! I recall reading somewhere that bulbar symptoms were an indication for PLEX given that it may work faster (doesn’t seem to be true from the above studies). Any truth/thoughts on this?
Thanks Ryan! I dont know of any literature that supports that for GBS, BUT there is evidence that PLEX works faster than IVIG in patients with Myasthenia Gravis crisis. These patients often present with bulbar symptoms, and may have rapid enough improvement that you may be able to get by with just NIV with rapid induction of immunosuppression (and if they can control secretions). So, I personally always choose PLEX for patients in myasthenia crisis in hopes that we can turn things around quickly enough to avoid intubation. couple references: PMID: 8352670, PMC4514693, PMID: 10025801
Interesting, thanks Casey!
Hi, is there an audio podcast for this post?
Casey and I will be doing GBS and MG podcast soon
IVIG is not a preferred agent in ESRD/CKD patients. Risk of overload. I think that’s very important to remember in considering these two agents. And essentially the only thing I really put thought into… do I want volume or not?
Nice topic! Agree – PLEX is the way to go. Cheaper overall for the treatment duration. Also worth noting that the first session of PLEX removes majority of immunoglobulins. If time is nerves – well, you get the idea. If memory serves correctly, for MG, PLEX is slightly better. With careful placement of HD cath, we can minimize risk of infections.
Thank you so much for this review. It’s a topic which brings me feelings. My main concern on this topic is that in my country, IVIG and PLEX next to each other is a common practice, which I think causes harm without benefit, as far I know (and, in theory, PLEX after IVIG makes very little sense, as you said). But even regarding the 1st line treatment, I have concerns. I confess I didn’t know IVIG was that expensive and that you could make PLEX through a peripheral catheter. Even though, I also think that’s not a common practice in… Read more »