
The Society of Critical Care Medicine published over 1,800 abstracts to go along with their latest conference. I sifted through them to come up with my favorite 20. Kudos to all the authors on creating diverse and thoughtful work – the future of critical care is indeed bright!
The abstracts are divided into six groups: cardiology, hematology, pulmonology, nephrology, neurology, and miscellaneous. No matter what your interests are, there's probably something here for you.
cardiology
can we just shut off the vaso?
Vasopressin has a relatively long half-life compared to other vasopressors, making it a bit harder to titrate rapidly. This has led some protocols to mandate very gradual weaning. These authors demonstrated that simply shutting off the vasopressin was safe. This finding is consistent with the concept that as patients improve, their “relative vasopressin deficiency” may resolve – so they just don’t need vasopressin any more.

metoprolol vs. diltiazem for atrial fibrillation in the ICU
Diltiazem versus metoprolol for atrial fibrillation is an age-old debate. Shockingly little evidence exists regarding this, especially for treating ICU patients. Diltiazem seems a bit preferable in emergency medicine and cardiology cohorts, but ICU patients may be different.
This retrospective quasi-experimental study suggested that metoprolol might work better in the ICU. This could make sense, since patients in the ICU are often suffering from secondary AF due to elevated sympathetic tone. The number of patients in the study isn't reported, so the statistical significance of the findings is unclear.

midodrine to accelerate liberation from vasopressors
Oral midodrine to accelerate weaning off vasopressors: Is this cheating, or is it a legitimate strategy for reducing length of stay and promoting earlier rehabilitation? A few abstracts supported the use of midodrine: here is one from a trauma ICU and another from a medical ICU.


hematology
over-diagnosis and over-treatment of heparin-induced thrombocytopenia continues to cause harm
Over-diagnosis and over-treatment of HIT is a persistent problem. This retrospective survey shows over-diagnosis of HIT leading to iatrogenic hemorrhage. I suspect similar results could be found in most hospitals.
The authors attribute this largely to the under-utilization of the 4T score. However, even if patients with low-risk 4T scores had been excluded, this cohort of patients still would have experienced substantial iatrogenic harm due to overenthusiastic use of anticoagulants (among patients with intermediate or high-risk 4T score, only 9/91 actually had HIT). This substantiates the concept that all patients with intermediate 4T scores don't automatically require immediate anticoagulation (but rather, this can be personalized, based on a risk/benefit calculation). More on this in the IBCC chapter on thrombocytopenia.

weight-based enoxaparin for DVT prophylaxis
Dosing of enoxaparin for morbidly obese patients remains controversial. It’s unlikely that we will have a massive, robust RCT on this anytime soon. Thus, smaller studies with pharmacological endpoints make sense.
Weight-based dosing seems logical, since this is how we dose enoxaparin for other indications. Most studies on weight-based enoxaparin prophylaxis have used a dose of 0.5 mg/kg daily. This study uses twice that dose (0.5 mg/kg BID) – and yet still was very successful at achieving target anti-Xa levels. This raises a question of whether daily enoxaparin may be leaving patients subtherapeutic for periods of time. At the very least, this new data should be reassuring that using a dose of 0.5 mg/kg daily (or 0.25 mg/kg BID) is unlikely to cause bleeding in patients with intact renal function.

pulmonary
blindness as a complication of prone ventilation
Complex interventions can lead to unexpected iatrogenic complications. This case report describes a patient who developed blindness due to ischemic optic neuropathy, during prone ventilation. To make this even scarier, the case comes from the University of Colorado – a center with extensive expertise in prone ventilation. So, if this could happen in Colorado, it could happen anywhere.
I continue to doubt whether the PROSEVA trial on prone ventilation could be replicated outside of France (particularly in the United States).1 Especially in the context of a recent review on mortality endpoints in critical care, the results from PROSEVA seem a bit too good to be true.2
When proning, avoid putting any pressure on the eyeballs. It seems like a compartment syndrome physiology may be going on here – so any external pressure might exacerbate matters.

is obesity supine death syndrome a thing?
There is definitely a cohort of patients with severe morbid obesity who do poorly in a supine position. The physiology here is pretty simple: a reverse Trendelenburg or seated position prevents the abdominal compartment from compressing the thorax. When lying flat, abdominal weight compresses the diaphragm, leading to atelectasis and diaphragmatic fatigue. The classic clinical history is someone who can't lie down due to dyspnea (often sleeping in a seated position). If these patients are forced to lie flat (e.g. postoperatively or in an ambulance), disaster can ensue. When recognized promptly, this syndrome is reversible with repositioning and BiPAP.

nephrology
point-of-care potassium measurement often overlooks hemolysis
We're all used to seeing falsely elevated potassium levels due to hemolysis. Most of the time, these labs are sent to a central laboratory which evaluates for hemolysis. Thus, the high potassium levels will be flagged as “hemolyzed” – and we know not to over-react. Point-of-care meters can't detect hemolysis, so there is the potential to return falsely elevated potassium levels without any warning that they are hemolyzed. This may be a fairly common problem (40% in this series!), so be careful. Before treating for hyperkalemia, look at the EKG and consider repeating the lab.

additional vancomycin is bad for patients with vancomycin-induced acute kidney injury
How should one manage vancomycin-induced nephrotoxicity? This can create a bit of a vicious cycle, whereby renal dysfunction causes retention of vancomycin, leading to higher vancomycin levels and further renal dysfunction. I've encountered a couple patients who retained so much vancomycin that they required dialysis to remove it.
This retrospective study compared management of vancomycin-related acute kidney injury by dose-reducing vancomycin versus transitioning to linezolid. Not surprisingly, transition to linezolid correlated with faster resolution of the renal injury. (Although perhaps a more interesting question might be: why use vancomycin at all for MRSA pneumonia? Some advantages of linezolid over vancomycin are explored in the IBCC here.)

hyponatremia due to vasopressin in the neuro ICU
Physiologically, vasopressin infusion should cause free water retention and carry a risk of hyponatremia. Large RCTs haven't consistently reported this, but I've seen it. This abstract reports cases of patients who developed hyponatremia on vasopressin infusions, with rapid improvement when the infusion was discontinued. This isn't RCT-level data, but it's fairly convincing.

is hypertonic saline nephrotoxic?
This is a single-center, double-blind trial comparing hypertonic sodium chloride versus hypertonic sodium acetate in a neuro ICU. Both solutions had similar effects on the intracranial pressure. However, the sodium acetate led to lower rates of acute kidney injury and lower levels of renal biomarkers. This is a thought-provoking study, suggesting that we should consider not only the tonicity of hypertonic solutions in the neuro ICU, but also their chloride content.

neurology
fentanyl shortages… improve patient care?
This is a multi-center quasi-experimental study evaluating the consequences of a fentanyl shortage. Due to the shortage, fentanyl infusions were restricted – resulting in an 84% reduction in average opioid doses. However, there was no change in the patients' pain levels! This supports the concept that fentanyl infusions are often left running at excessive rates, causing exposure to unnecessarily high opioid doses (more on the evil of fentanyl infusions here).

lorazepam shortage also… improves patient care!
Continuing with the theme of fortuitous drug shortages… a lorazepam shortage forced practitioners at the University of Massachusetts to transition to a new protocol for alcohol withdrawal involving midazolam and phenobarbital. The new protocol worked better, with a considerably lower rate of intubations. When the lorazepam shortage ended, they decided to keep using the new protocol!

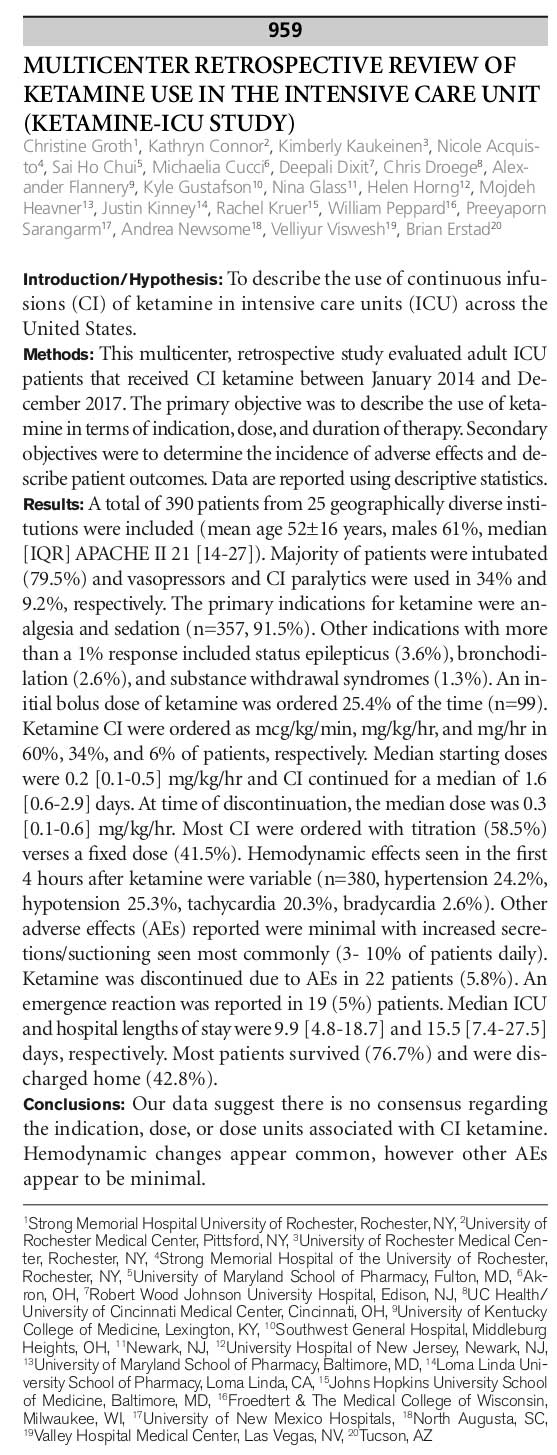
ketamine infusions for the win (KETAMINE-ICU study)
This is a retrospective study describing the use of ketamine infusions in 390 patients within 25 institutions. Ketamine use correlated with improvements in achieving target levels of pain and sedation, without signals of increased delirium. This is a retrospective study which should ideally be confirmed by prospective RCTs, but it's consistent with an emerging body of evidence. Ketamine infusions may offer patients improvements in analgesia as well as less depression – important patient-centered outcomes.

Here is another abstract from the same study, this one focusing on adverse events. In most cases pain-dose ketamine infusions were used, but some patients received higher doses for other indications (e.g. seizure or bronchodilation). Overall, ketamine seems to have been well tolerated:
ketamine as a second-line antiepileptic for status epilepticus
Ketamine has enormous potential as a second-line agent after benzodiazepines (based on its hemodynamic stability, ability to be given as a rapid bolus, wide availability, and lack of respiratory suppression). This has been demonstrated in children, but adult data is lacking.1 Kudos to these authors for a courageous and potentially game-changing study. Further data is obviously required, but this is extremely promising.

phenobarbital for alcohol withdrawal in the neuro ICU
Management of alcohol withdrawal in patients with acute neurologic injuries is extremely challenging. These patients may be at increased risk of over-sedation (due to low neurologic reserve function). Also, there is often confusion about which symptoms are due to withdrawal versus the underlying neurologic disease.
These authors used a 10 mg/kg IM phenobarbital protocol for patients with neurologic injuries (sounds like the MGH protocol described by Nisavic).3 This worked well, demonstrating that finite doses of phenobarbital may be useful even in complex patients. I generally like this protocol, but see no real reason to use multiple intramuscular phenobarbital injections in patients with IV access (slow intravenous administration would be equally efficacious and less painful).

phenobarbital for non-alcohol-related agitated delirium
Phenobarbital is increasingly used for alcohol withdrawal, but it could have utility as a general sedative as well. Phenobarbital's predictable pharmacokinetics and balanced activity on GABA and glutamate systems could make it superior to other sedatives (especially benzodiazepines).4

miscellaneous
pharmacists are life savers! (PHARM-EM & PHARM-CRIT)
Hiring more ICU and ED pharmacists may simultaneously cut costs and improve outcomes. These are two studies detailing the diverse goodness which results from having specialized unit pharmacists who are integrated into the care team. Note that both studies found that pharmacists prevented major adverse drug events and were also are involved in hands-on care (personally I've found pharmacists to be among the most helpful colleagues during codes and crises).
These studies come as zero surprise to me (or, probably, anyone). However, this is some good evidence if you're trying to convince folks in the C-suite to hire more pharmacists. Hiring pharmacists will cut costs, improve quality, avoid lawsuits, de-stress other providers, improve education… I could go on…


do we really need to remove that line?
What should we do about a central line that winds up in the subclavian vein or in the right atrium? Traditional teaching has been that the line must be repositioned or replaced. However, a more zentensivist strategy is to simply use the line (since these locations seem to be safe, whereas repeat procedures will definitely expose the patient to additional risks). This abstract provides further evidence that we can relax our definition of what constitutes an acceptable catheter location.

Rothman Index fails to correlate with mortality in surgical ICU patients
The Rothman Index is an electronic early warning system, which aims to rapidly identify the sickest patients. In this SICU trial, the Rothman Index failed to correlate with mortality. This is consistent with an emerging body of evidence that the Rothman Index doesn't really work.

Image credit: Jennifer Pallain
references
- 1.Ilvento L, Rosati A, Marini C, L’Erario M, Mirabile L, Guerrini R. Ketamine in refractory convulsive status epilepticus in children avoids endotracheal intubation. Epilepsy Behav. 2015;49:343-346. doi:10.1016/j.yebeh.2015.06.019
- 2.Santacruz CA, Pereira AJ, Celis E, Vincent J-L. Which Multicenter Randomized Controlled Trials in Critical Care Medicine Have Shown Reduced Mortality? A Systematic Review. Critical Care Medicine. December 2019:1680-1691. doi:10.1097/ccm.0000000000004000
- 3.Nisavic M, Nejad S, Isenberg B, et al. Use of Phenobarbital in Alcohol Withdrawal Management – A Retrospective Comparison Study of Phenobarbital and Benzodiazepines for Acute Alcohol Withdrawal Management in General Medical Patients. Psychosomatics. 2019;60(5):458-467. doi:10.1016/j.psym.2019.02.002
- 4.Gagnon DJ, Fontaine GV, Riker RR, Fraser GL. Repurposing Valproate, Enteral Clonidine, and Phenobarbital for Comfort in Adult ICU Patients: A Literature Review with Practical Considerations. Pharmacotherapy. October 2017:1309-1321. doi:10.1002/phar.2017

- PulmCrit Wee: Rational selection of infusion rate based on loading dose - June 25, 2024
- PulmCrit: PPIs are safe and effective for GI prophylaxis… the end. - June 18, 2024
- PulmCrit: Bilevel Sequence Intubation (BSI) – The new standard - June 17, 2024
Wow! Thanks for the amazing compilation!!
This is a fantastic post, thank you for the great summary!
Thank you so much for your very creative and expedient formats for learning. We have turned on many of our colleagues to your posts and special stories; always so thought provoking. We frequently cite your content on through our social media and soon to be re-launch website. Best Dave
Does anyone know where one can view these abstracts, would love to get the contact details of the authors of the paper looking into ketamine for status.