 Antiviral therapy for influenza is a sore subject. Oseltamavir was initially felt to be a silver bullet. Unfortunately, it turned out that its efficacy was overblown by publication bias. Discordance between guidelines, practice, and evidence remains frustrating.
Antiviral therapy for influenza is a sore subject. Oseltamavir was initially felt to be a silver bullet. Unfortunately, it turned out that its efficacy was overblown by publication bias. Discordance between guidelines, practice, and evidence remains frustrating.
Regardless, flu seasons is upon us again. A recent paper in CHEST provides some tantalizing evidence about possible treatment. Will this pan out, or is it just another fairy tale?
Brief background on naproxen for influenza
Naproxen may inhibit viral replication
 Nucleoprotein is an influenza protein required for viral replication. It has no human counterpart, making it an attractive target for antiviral therapy. Lejal 2013 used a computer simulation to test all available drugs for the ability to block nucleoprotein. This search identified naproxen. Further testing confirmed that naproxen binds to nucleoprotein in vitro. In cell cultures, naproxen inhibited replication by both H1N1 and H3N2 viral strains. In mice, naproxen reduced influenza viral titers and symptoms.
Nucleoprotein is an influenza protein required for viral replication. It has no human counterpart, making it an attractive target for antiviral therapy. Lejal 2013 used a computer simulation to test all available drugs for the ability to block nucleoprotein. This search identified naproxen. Further testing confirmed that naproxen binds to nucleoprotein in vitro. In cell cultures, naproxen inhibited replication by both H1N1 and H3N2 viral strains. In mice, naproxen reduced influenza viral titers and symptoms.
NSAIDs can modulate host immune response
It is also possible that the anti-inflammatory effects of NSAIDs could be beneficial, specifically their ability to block the COX-2 enzyme. Influenza causes up-regulation of COX-2 levels in the lung. Mice deficient in COX-2 are resistant to infection by influenza. This suggests that NSAIDs could improve clinical outcomes by inhibition of the COX-2 enzyme.
Li 2014 investigated the efficacy of zanamavir (a neuraminidase inhibitor similar to oseltamavir) and celecoxib (a COX-2 inhibitor) in mice infected with influenza. When given 48 hours after infection, neither drug could prevent death. However, mice treated with both drugs had improved survival and less lung injury. Addition of celecoxib had no effect on viral levels, suggesting that it was acting as an anti-inflammatory agent.
Brief background on clarithromycin for influenza
Clarithromycin has anti-inflammatory effects
Clarithromycin and azithromycin are well known to have immunomodulatory effects that may reduce lung injury. For example, in mice clarithromycin reduces inflammation and lung damage due to high tidal-volume ventilation (Amado-Rodriguez 2013). It is likely that much of the benefit of these drugs in clinical practice is due to immunomodulation (as explored here regarding pneumonia).
Clarithromycin may inhibit viral replication
 Influenza enters respiratory cells via binding to sialic acids and then being partially digested in endosomes. Clarithromycin may affect both of these processes. It has been shown to down-regulate the sialic acid that binds to influenza (figure below) and also reduce endosome formation. This reduces replication of influenza H3N2 within human tracheal epithelial cells (Yamaya 2010). Clarithromycin also reduces the release of pro-inflammatory cytokines by tracheal epithelial cells (including IL-1, IL-6, and IL-8).
Influenza enters respiratory cells via binding to sialic acids and then being partially digested in endosomes. Clarithromycin may affect both of these processes. It has been shown to down-regulate the sialic acid that binds to influenza (figure below) and also reduce endosome formation. This reduces replication of influenza H3N2 within human tracheal epithelial cells (Yamaya 2010). Clarithromycin also reduces the release of pro-inflammatory cytokines by tracheal epithelial cells (including IL-1, IL-6, and IL-8).
 Clinical evidence regarding clarithromycin for influenza
Clinical evidence regarding clarithromycin for influenza

Higashi 2014 performed a single-center open-label RCT investigating the use of clarithromycin for influenza. All patients received neuraminidase inhibitors (mostly oseltamavir), with half randomized to receive additional treatment with clarithromycin. Clinical outcomes in both groups were similar (table below). Some subgroups appeared to benefit from clarithromycin, but this is hypothesis-generating only.
 A larger study of macrolides for influenza was performed by Nimomiya 2002. 365 children with influenza-like illness were randomized to receive a cephalosporin or a macrolide (148 received clarithromycin and 63 received erythromycin). Patients treated with macrolides defervesced more rapidly and were less likely to progress to influenza pneumonia. Despite methodological problems, this study suggests a benefit from macrolides.
A larger study of macrolides for influenza was performed by Nimomiya 2002. 365 children with influenza-like illness were randomized to receive a cephalosporin or a macrolide (148 received clarithromycin and 63 received erythromycin). Patients treated with macrolides defervesced more rapidly and were less likely to progress to influenza pneumonia. Despite methodological problems, this study suggests a benefit from macrolides.
 Paradigm of multi-drug therapy for influenza
Paradigm of multi-drug therapy for influenza

Synergistic antiviral activity
Oseltamavir is undeniably a disappointment. However, it does have some activity against influenza, causing reduced viral shedding and decreased symptom duration. It's not the silver bullet we were hoping for, but it may not be entirely worthless either.

 It's possible that treatment for influenza requires several antivirals working together, similar to therapy for HIV and hepatitis C. This is supported by experients in mice showing that zanamivir alone is ineffective, but it can reduce mortality when combined with celecoxib or celecoxib plus mesalamine (Li 2014, Zheng 2008). Thus, it is possible that an ideal regimen for influenza might be a cocktail of several drugs, each of which is somewhat effective and minimally toxic. Oseltamavir, naproxen, and clarithromycin exert their antiviral effects on different targets, suggesting that their anti-viral activities would work synergistically.
It's possible that treatment for influenza requires several antivirals working together, similar to therapy for HIV and hepatitis C. This is supported by experients in mice showing that zanamivir alone is ineffective, but it can reduce mortality when combined with celecoxib or celecoxib plus mesalamine (Li 2014, Zheng 2008). Thus, it is possible that an ideal regimen for influenza might be a cocktail of several drugs, each of which is somewhat effective and minimally toxic. Oseltamavir, naproxen, and clarithromycin exert their antiviral effects on different targets, suggesting that their anti-viral activities would work synergistically.
Combined antiviral activity and immunomodulation
One question regarding influenza therapy has been whether to try to suppress the immune system (e.g. with steroid). It seems that much of the damage from influenza is due to host inflammation, suggesting that immunosuppression might be beneficial. However, immunosuppression could also lead to inadequate immune control of the virus.
The ideal strategy is probably a combination of antiviral therapy plus immunosuppression. Immunosuppression would block excessive inflammation that causes organ dysfunction. Meanwhile, antiviral therapy prevent inadequate control of the virus. Triple therapy for influenza might achieve this since all agents have anti-viral effects, while naproxen and clarithromycin have immunosuppressive effects.
Hung 2016: Efficacy of clarithromycin-naproxen-oseltamavir combination in the treatment of patients hospitalized for influenza A (H3N2) infection: an open-label, randomized controlled, phase 2b/3 trial.
This is a single-center, unblinded RCT comparing oseltamavir monotherapy vs. triple therapy among patients with pneumonia due to influenza H3N2:
- Control group = oseltamavir 75 mg BID for 5 days
- Combination therapy = oseltamavir plus clarithromycin 500 mg BID & naproxen 200 mg BID for two days
This study was restricted to patients with pulmonary infiltrates who required hospital admission, representing the sickest cohort of influenza patients. Notable inclusion criteria are:
- temperature >38
- symptom duration <72 hours at admission
- initiation of study drugs within 24 hours of admission
- laboratory-confirmed influenza H3N2
- pulmonary infiltrates visualized either via CXR or CT chest
- creatinine clearance > 30 ml/min
217 patients were enrolled over two consecutive years. Patients were well matched at baseline. No patients were lost to follow-up. However, as patients improved they increasingly refused to allow collection of nasopharyngeal samples for viral analysis.
Clinical outcomes
The primary end-point was mortality. Combination therapy reduced mortality from 9/110 to 1/107 (p=0.01, fragility index of 1). Combination therapy reduced admission to the intensive care unit (7/110 vs. 2/107; p=0.1) and the step-down unit (34/110 vs. 17/107; p=0.009). The median duration of hospitalization was decreased from three days to two days in the combination therapy group (p<0.0001).
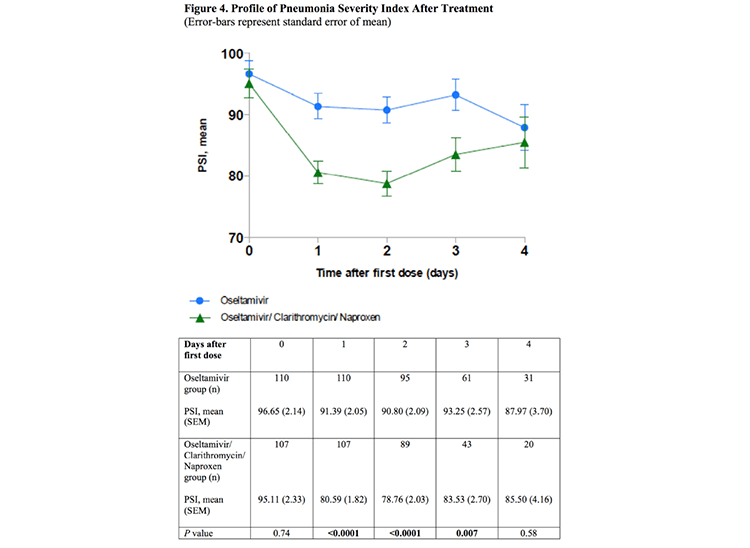 Port Severity Index is a prognostic score for pneumonia (incorporating data such as age, comorbidities, vital signs, and labs). Over the first day, patients in the combination therapy group experienced a greater improvement in Port Severity Index (p<0.0001; figure above). Please note that data from days #3-4 is unreliable, because many patients had already left the hospital by then. It should be noted that some decrease in the Port score could simply reflect the antipyretic effect of naproxen.
Port Severity Index is a prognostic score for pneumonia (incorporating data such as age, comorbidities, vital signs, and labs). Over the first day, patients in the combination therapy group experienced a greater improvement in Port Severity Index (p<0.0001; figure above). Please note that data from days #3-4 is unreliable, because many patients had already left the hospital by then. It should be noted that some decrease in the Port score could simply reflect the antipyretic effect of naproxen.
Virology outcomes
The amount of virus in nasal washings appeared to fall more rapidly among patients in the combination therapy group (figure below, left). However, these results could have been compromised over time as patients refused nasopharyngeal washes, leading to data loss.
 Perhaps more impressive, combination therapy prevented the selection of oseltamavir-resistant virus (“NIRV” shown in the figure above, right). Upon admission, both groups had a roughly 3% rate of oseltamavir-resistant viruses. Different therapies had opposite effects on viral resistance:
Perhaps more impressive, combination therapy prevented the selection of oseltamavir-resistant virus (“NIRV” shown in the figure above, right). Upon admission, both groups had a roughly 3% rate of oseltamavir-resistant viruses. Different therapies had opposite effects on viral resistance:
- Oseltamavir monotherapy increased the frequency of resistant viruses. This makes sense: an antimicrobial agent selects for viruses which are resistant to it.
- Combination therapy decreased the frequency of resistant viruses. This might be explained as follows. Oseltamavir-resistant strains of H3N2 are known to be weak, with diminished replication (Baranovich 2011). If naproxen and/or clarithromycin impairs viral replication, then combination therapy could create an environment where oseltamavir-resistant viral strains are too weak to survive. The concept that multi-drug therapy blocks the emergence of resistant viruses has parallels to HIV therapy.
Safety
Two patients in the combination therapy group with baseline creatinine of 1.2 mg/dL developed a rise to 1.4-1.5 mg/dL after completing treatment. This spontaneously decreased back to their baseline value. No other complications were reported.
Antibacterial therapy & possible contamination with pneumonia
One concern regarding this study might be contamination with patients who are co-infected with both influenza and bacterial pneumonia. If this were common, then there could have been a benefit from clarithromycin due to its effect on bacterial pneumonia.
However, this doesn't seem to have been a significant problem. Bacterial superinfection is unlikely to occur among patients who present within three days of symptoms (it usually occurs later on). All patients were found to be negative for atypical pathogens (mycoplasma, chlamydia, legionella), based on PCR of nasopharyngeal washings upon admission. Eight patients had positive bacterial cultures upon admission, although in many cases these may have represented colonization only.
All patients were treated with oral amoxacillin-clavulanic acid to cover the possibility of bacterial pneumonia. The universal presence of antibacterial therapy should reduce any impact that clarithromycin may have via its anti-bacterial effects.
Other study limitations

- Single-center, open-label design. This limits the ability of this study to be definitive. However, the most important outcomes (mortality, viral analysis, Port Severity Index) seem fairly objective.
- Generalization to other influenza strains? This study investigated the H3N2 strain of influenza, which is the dominant strain during this influenza season in the United States (figure above). So this study is ideal for now. However, it remains unproven whether these medications might work against different influenza strains in the future. This is an implicit weakness of most influenza research, because every few years we are facing a slightly different virus.
- Gastric prophylaxis: All patients in this study received 20 mg esomeprazole for ulcer prophylaxis. The risk of naproxen may higher if administered without esomeprazole.
Ready for prime time?
This is a single-center trial with substantial methodological limitations. However, the theoretical rationale for these medications is fairly persuasive. Perhaps most importantly, the safety profiles of clarithromycin and naproxen are very good (when excluding patients with renal failure). The duration of therapy is short (two days), which should also limit any toxicity. Many flu-positive patients with pneumonia would receive anti-bacterial therapy for 1-2 days anyway, for coverage of possible bacterial pneumonia.
 For comparison, a combination of naproxen and pseudoephedrine is available over-the-counter for cold and sinus relief (Aleve-D). A two-day course of naproxen/clarithromycin is probably safer than a longer course of Aleve-D (the patient instructions recommend continuing Aleve-D for up to one week).
For comparison, a combination of naproxen and pseudoephedrine is available over-the-counter for cold and sinus relief (Aleve-D). A two-day course of naproxen/clarithromycin is probably safer than a longer course of Aleve-D (the patient instructions recommend continuing Aleve-D for up to one week).
This trial clearly requires validation. What should we do in the interim? There may not be any definitive right or wrong answer. Waiting for additional data is certainly reasonable. However, giving patients a two-day course of clarithromycin and naproxen seems reasonable as well. This may depend on your practice style, for example whether you are an early-adopter vs. late-adopter. When you get sick, would you prefer to take Aleve-D or wait it out? Hot tea or vodka martini?
One pitfall to avoid is indication creep. This study found a benefit within a small group of patients with a laboratory-confirmed diagnosis of influenza, chest infiltrates, adequate renal function, symptom duration <72 hours, and illness severity requiring hospital admission. Applying this treatment in an indiscriminant fashion should be avoided.

- Although oseltamavir has anti-viral activity against influenza, its efficacy has been clinically disappointing.
- Naproxen and clarithromycin both have anti-viral and immunomodulatory effects in vitro and in mouse studies. Animal studies suggest that NSAIDs work synergistically with neuraminidase-inhibitor therapy.
- Hung 2016 performed a single-center open-label study evaluating the addition of a 2-day course of naproxen and clarithromycin to oseltamavir among inpatients with pneumonia due to H3N2 influenza. Combination therapy reduced mortality, transfer to step-down units, pneumonia severity, and viral replication.
- Further evidence is needed. In the interim, a brief course of naproxen and clarithromycin may be considered for carefully selected patients (e.g., onset <72 hours before presentation, patients admitted to the hospital with lab-proven influenza pneumonia, adequate renal function).
Image credits: cocktail, flu epidemiology images from the CDC
#/media/File:Bright-Field_Lighting.jpg){kind=link}

- PulmCrit Wee: Rational selection of infusion rate based on loading dose - June 25, 2024
- PulmCrit: PPIs are safe and effective for GI prophylaxis… the end. - June 18, 2024
- PulmCrit: Bilevel Sequence Intubation (BSI) – The new standard - June 17, 2024
Thank you for another excellent post!!!
I’ll definitely try it…
Watch out for eosinophilic colitis and naproxen…
https://www.ncbi.nlm.nih.gov/pubmed/2220886
http://bmb.oxfordjournals.org/content/100/1/59.full
Josh – thanks for the great review. There’s a lot of interesting stuff here particularly the physiologic theory of fighting viruses vs. bacteria. Reading the article, I do have some questions in their stats. They stated that they needed to enroll 93 patients/group for 80% power to find an 18% difference in mortality based on prior ICU trials showing a 35% mortality in the influenza group and 17% mortality in the combo therapy group. There are a number of issues here. This study wasn’t looking at ICU patients so basing their numbers on prior ICU trials doesn’t make sense and… Read more »
Anand, Thanks for your thoughts. I agree entirely. The power calculation doesn’t make much sense to me. When they first registered their study, the primary outcome was listed as viral titer (registration here: http://www.isrctn.com/ISRCTN11273879). So it is possible that the study was initially powered to look for viral titer, but then stumbled across a mortality difference, then re-wrote things to make mortality the primary endpoint. This might make more sense overall — to design this study with 200 patients using a primary endpoint of mortality seems excessively optimistic. In fairness, they did do some very clever things. I think limiting… Read more »
Early administration of oseltamivir that is within 12 hrs even within 6 hours of symptom presentation very significantly improves outcomes in many reported trials . With PCR and rapid turnaround efficiencies this can be achieved . The IMPACT study group in J Antimicrob Chemotherapy Jan51(1) 123-129 AokiFY et al Initiation of therapy within 12 hours after fever onset reduced duration of illness by 74.6 hours as well as severity of symptoms and return to baseline . Robert Derlet MD : Infectious diseases 2015 Audiodigest claims a study showing administration of oseltamivir within six hours reduced duration of illness from 182hours… Read more »
Early administration of oseltamavir by early within 6-12 hrs of presentation of patients yield considerably better results in several trials .
And the system has the capacity .With PCR and rapid laboratory turnover.
Thank you. Was just curious since I had a case like this last week. Happy New Year !
very cool , Josh,
is the considerations the same now in nov 2017?
I wrote this post a year ago, but have never used this therapy because I still haven’t encountered a patient who met the inclusion criteria. I think the same considerations apply this season. The question as always is how far you can/should stray from these inclusion criteria (highlighted in purple above in the main blog). I don’t have capacity to obtain serotyping of influenza, so for me a positive flu PCR would be adequate (rather than specifically being H3N2 positive). Strictly avoiding patients with renal dysfunction (GFR<30-45 ml/min) is probably important. I would also try to stick fairly close to… Read more »