
Some topics that have been batting around my head over the past few months:
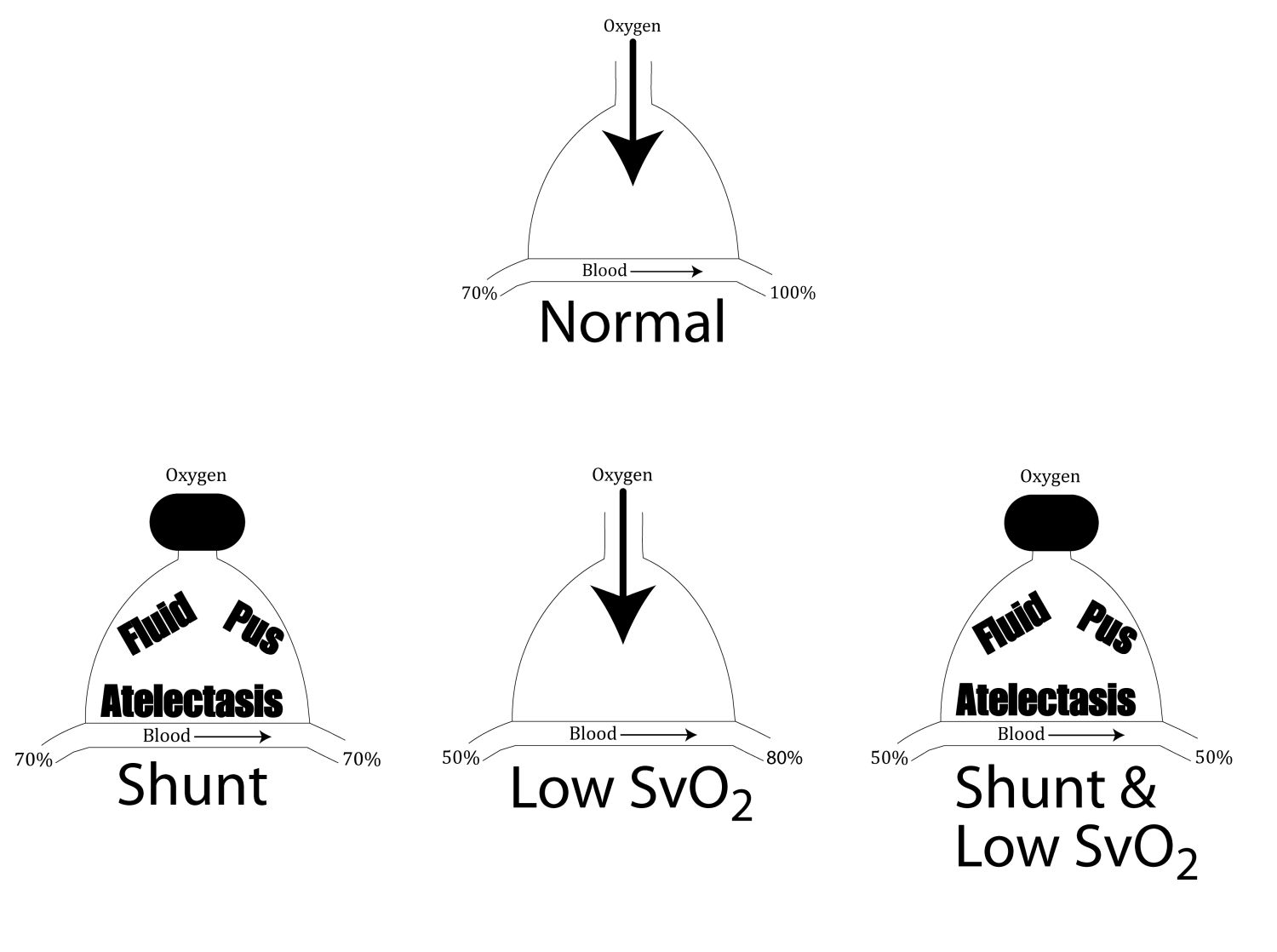
The Secret Sixth Cause of Arterial Hypoxemia
You should know the standard five:
- V/Q Mismatch (Deadspace)
- Low FiO2
- Hypoventilation
- Diffusion Abnormality
- Shunt (Usually Physiologic)
but the sixth cause can be particularly dangerous with cause #5, the physiologic shunt. The sixth cause is Low Mixed Venous Saturation (SvO2).

John Marinaro created this acronym for the causes above:
Shunt
Hypoventilation
Altitude/low PAO2
V/Q mismatch
Excess extraction of O2 from Hb (low SvO2)
Diffusion Abnormalities
Pure Vasoactives
It ain't phenlephrine anymore
Norepinephrine is a pure vasopressor
and
Epinephrine is a pure inotrope
Dissociated Awake for Critical AS/Pulmonary Hypertension
just keep loving this more and more. See the hemodynamically neutral intubation podcast for the final version of this idea.
Additional New Information
More on EMCrit
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Editor-in-Chief, at EMCrit.org
An ED Intensivist from NY.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
Professor
Nassau University Medical Center
No conflicts of interest (coi).
Latest posts by Scott Weingart, MD FCCM (see all)
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Thanks Scott, I not infrequently will get an Vbg and the PO2 is over 100 or essentially normal and pt not hyperemic. what is up with this? And i don’t think this was an arterial sample.
Hey Scott – Thanks for the venous admixture discussion; it’s a hugely important cause of hypoxemia in clinical medicine. I’ve been fortunate to spend the past couple years learning from some brilliant respiratory physiologists, so I thought I’d share a few gas exchange pearls that blew my mind initially. For a more thorough explanation, check out the following open-access review (co-authored by one of my colleagues, in full disclosure): http://erj.ersjournals.com/content/44/4/1023.long, PMID: 25063240 1) Diffusion limitation: I previously learned and envisioned this cause of hypoxemia as a process that thickens the alveolar-capillary membrane resulting in impaired transit of respiratory gases from… Read more »
Nick fantastic comments. Diffusion is obv. the least important of the causes and rarely rears its head. Fibrotic lungs do indeed exhibit diffusion abnormalities directly related to structural lung changes, see attached IPF article (AJRCCM).Basically deadspace measurements by MIGET, any hypoxemia beyond what that predicts is branded diffusion. (of course this is just spouting off my recollection of pulm boards crap, b/c I’ve never even seen a MIGET much less performed one.) Lost me on the high V/Q not causing hypoxemia, this is the most common cause of hypoxemia in all of the clinical physio books. Problem is not direct… Read more »
Agreed Scott. Think we’re saying the same thing about high V/Q, but in a different way. It’s really the diversion of blood to regions of low V/Q or shunt that directly causes hypoxemia.
I think this article has a nice physiologic breakdown of your argument Nick.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4070768/
Chase Donaldson
EM/CCM
Any literature supporting a (even rough) correlation between peripheral venous pO2 and ScvO2? I had always thought it to be an essentially meaningless figure, and indeed have a hard time seeing why it would be meaningful — presumably the relevant figure is venous oxygenation downstream of the viscera and central circulation, not after reaching the left arm, say.
Meant pt is not hyperoxic as opposed to hyperemic
Hey Scott
I missed any comment on paralytics in the last section.
Are you paralysing just before sliding the ETT over the bougie and through the cords?
Or is this a sedation only intubation?
Dean
no paralytics, that would defeat the purpose
Ok, not a respiratory physiologist but can you clarify?
Are not shunt and V/Q mismatch the same thing? Shunt is perfusion past non-oxygenated alveoli (or simply a true R->L connection) which is essentially lots of Q without any V.
Am I missing something?
And w.r.t. pure vasopressors/inotropes/arterial dilators…. where does vasopressin stand? Amrinone? Milrinone? dare I say it… Digoxin?
Mike
i think i discussed this a bit in the cast, but the extremes are deadspace and shunt. they are both V/Q mismatch. however, many equate the term v/q mismatch with extreme v and no q, i.e. deadspace.
dig is also a pure inotrope in my convoluted new terminology. vaso will cause decreased inotropy from afterload, just like phenyl. amrinone and milrinone are inodilators
Quick question about the aftermath of the dissociated intubation. Once tube is in, you have a pt with 0.5 mg/kg of ketamine on board, intubated, and spontaneously breathing. But the addition of sedation and positive pressure ventilations both still place them at risk for decreased preload and altered hemodynamics which could cause problems d/t the critical AS. How do you add in sedation/PPV on this pt post intubation? Do you leave them only “ketamized” while starting low VT mechanical ventilation with minimal PEEP and add in analgesia with fentanyl after they have equibrilated with the change to PPV? What is… Read more »
you leave them “ketaminized”
on the same PEEP/PSV as they were before intubation and let them spont breathe
try to transition to pain control only without sedation
Dr Weingart- thanks for the great podcast as always. Terrific grab bag!
Can you clarify what you consider to be “inotropic dosing” of epinephrine? Sub 0.3 mcg/kg/min, as some texts suggest? Similar for adults and peds then?
Thanks!
Bryan Winchell, RN, EMT-P
Flight Medic/Nurse, Flight For Life Texas
Hey Scott, Enjoyed your discussion on the vasoactive agents. “Pure” with respect to mechanism of action is not necessarily “pure” with respect to overall physiologic balance. I’ve found no more powerful tool to better guide the clinical question of vasoactive choice in sick patients than Echo (and serial Echos). With regard to Ketamine-Dissociated intubation: my experience with this has been great. There is not much data on this (yet). The only issue I have encountered is the variable jaw tone that results with K dissociation. I think the tone is a result of many factors, (how sick the patient is… Read more »
agree on all of the stuff above