 Early Goal-Directed Therapy: A house collapsing in slow motion
Early Goal-Directed Therapy: A house collapsing in slow motion

 The original foundation of the Surviving Sepsis Campaign was the Rivers trial on early goal-directed therapy. This is basically the NINDS trial of the critical care world: a study with ~300 patients showing implausibly positive results, published in NEJM, and rapidly brainwashing an entire discipline. The NINDS and Rivers trials became dogma not because they were rigorous, but rather because people wanted to believe them. After struggling for decades to treat stroke and sepsis, these finally represented some hope.
The original foundation of the Surviving Sepsis Campaign was the Rivers trial on early goal-directed therapy. This is basically the NINDS trial of the critical care world: a study with ~300 patients showing implausibly positive results, published in NEJM, and rapidly brainwashing an entire discipline. The NINDS and Rivers trials became dogma not because they were rigorous, but rather because people wanted to believe them. After struggling for decades to treat stroke and sepsis, these finally represented some hope.
The unfortunate reality is that the Rivers trial was a flimsy study. It was a single-center study with dodgy methodology, including mysterious disappearance of 25 patients who were randomized but never analyzed. Dr. Rivers had major conflicts of interest, including patenting a catheter to monitor svcO2.
The Rivers trial and the Surviving Sepsis Campaign popularized sepsis protocols, which saved lives. Massive accomplishment. However, that doesn't validate the individual components of early goal-directed therapy. Any protocol involving early identification and intensive care of septic patients probably would have worked.
Over time, nearly every component of early goal-directed therapy was disproven. Transfusing patients to a hemoglobin of 10 mg/dL is now recognized to be foolish. Central venous pressure predicts fluid responsiveness about as well as flipping a coin (Marik 2008). Monitoring the svcO2 saturation has been proven to be unnecessary. Massive fluid resuscitation encouraged by the protocol is increasingly recognized to be harmful (in the initial Rivers study, protocoled patients received an average of 13.4 liters!). The only core component that has survived the test of time is maintaining a mean arterial pressure above 65mm.
Although the components of the Rivers protocol have been disproven, it remains blasphemous to admit that the Rivers trial was wrong. The Rivers trial is the underpinning of a decade of research in sepsis. If the Rivers trial isn't valid, then many studies based on it aren't valid either. Admitting Rivers is wrong is like admitting that the foundation of our house has rotted and is about to collapse.
The Surviving Sepsis Campaign was founded on the basis of early goal-directed therapy. As this was disproven, the campaign stubbornly clung to it (for example, continuing to recommend CVP monitoring in 2014). The current guidelines have finally removed early goal-directed therapy, since to do otherwise would have rendered them irredeemably obsolete.
However, many vestiges of early goal-directed therapy remain in the current guidelines (e.g. serial lactate measurement). We must take a hard, objective look at such therapies to determine if they still stand up, now that early goal-directed therapy has collapsed.
Myth #6: Combination therapy is beneficial for gram-negative septic shock.
 Combination therapy is defined as using two drugs against gram-negative pathogens, with a goal of synergy (box above). This has been proven to be ineffective in numerous RCTs and meta-analyses (example below). It remains controversial whether to initially provide double-coverage for gram-negative pathogens. However, even advocates of double-coverage generally admit that combination therapy doesn't work (the main argument for double-coverage is to increase the likelihood that at least one drug covers the pathogen).
Combination therapy is defined as using two drugs against gram-negative pathogens, with a goal of synergy (box above). This has been proven to be ineffective in numerous RCTs and meta-analyses (example below). It remains controversial whether to initially provide double-coverage for gram-negative pathogens. However, even advocates of double-coverage generally admit that combination therapy doesn't work (the main argument for double-coverage is to increase the likelihood that at least one drug covers the pathogen).
 The Surviving Sepsis Campaign has been on the fence about this issue since its inception. The guidelines are slowly inching away from combination therapy. For example, the recommended duration of combination therapy has shrunk from 3-5 days (2012 guidelines) to “the first few days” (2016 guidelines). The indications for combination therapy have been pared back to only the sickest patients:
The Surviving Sepsis Campaign has been on the fence about this issue since its inception. The guidelines are slowly inching away from combination therapy. For example, the recommended duration of combination therapy has shrunk from 3-5 days (2012 guidelines) to “the first few days” (2016 guidelines). The indications for combination therapy have been pared back to only the sickest patients:
 The guidelines attempt to draw a sharp distinction between septic shock and sepsis. This isn't possible, because definitions have shifted over time and many studies of antibiotics contain a mixture of both conditions. Regardless, there is no high-quality evidence to support combination therapy for gram-negatives in either sepsis or septic shock (1).
The guidelines attempt to draw a sharp distinction between septic shock and sepsis. This isn't possible, because definitions have shifted over time and many studies of antibiotics contain a mixture of both conditions. Regardless, there is no high-quality evidence to support combination therapy for gram-negatives in either sepsis or septic shock (1).
Myth #5: Norepinephrine is the best vasopressor for all septic patients.
 Norepinephrine is a great drug for septic shock. Everyone likes norepinephrine. However, this consensus is threatening to create a dogma that norepinephrine is the best drug for every patient.
Norepinephrine is a great drug for septic shock. Everyone likes norepinephrine. However, this consensus is threatening to create a dogma that norepinephrine is the best drug for every patient.
Norepinephrine is clearly superior to dopamine. Beyond this, the evidence is unclear:
- One prospective RCT and a subsequent meta-analysis show equivalent outcomes comparing epinephrine vs. norepinephrine (Myburgh 2008, Avni 2015).
- Recent publication of the VANISH and VANCS trials support the use of vasopressin as a front-line vasopressor in patients with sepsis.
Overall, norepinephrine, epinephrine, and vasopressin are all supported by evidence as potential first-line vasopressors. There is no proof that any is superior to any other. It's possible that the best drug might depend on an individual's physiology:
 Myth #4: If one vasopressor doesn't work, additional drugs should be added in a sequential fashion.
Myth #4: If one vasopressor doesn't work, additional drugs should be added in a sequential fashion.

 The guidelines recommend the strategy above for titrating vasopressors. This algorithm ignores individual differences in hemodynamics and vasopressor responsiveness. For example, rapidly up- and down-titrating vasopressors may reveal how a patient responds to different drugs. This is safe and easy: make a change, observe, if it doesn't help then return to your prior regimen. Vasopressor challenge may be useful to select agents that work, while avoiding agents that aren't helping.
The guidelines recommend the strategy above for titrating vasopressors. This algorithm ignores individual differences in hemodynamics and vasopressor responsiveness. For example, rapidly up- and down-titrating vasopressors may reveal how a patient responds to different drugs. This is safe and easy: make a change, observe, if it doesn't help then return to your prior regimen. Vasopressor challenge may be useful to select agents that work, while avoiding agents that aren't helping.
One problem with the strategy recommended in the guidelines is that patients often wind up on high-dose norepinephrine plus vasopressin. This combination provides a lot of afterload, which may drop cardiac output in patients with cardiomyopathy (yes, that's right: vasopressor-induced shock). Such patients often respond nicely to up-titration of epinephrine with simultaneous down-titration of norepinephrine.
Myth #3: Lactate is a measure of tissue perfusion. Normalization of lactate should be used as a resuscitation target.
 It remains widely believed that lactate is a measurement of perfusion, systemic oxygenation, and anaerobic metabolism. This is a myth. Among septic patients, the primary cause of lactate elevation is beta-2 agonist stimulation (from endogenous and exogenous epinephrine). Beta-2 agonist stimulation causes the liver to secrete lactate via an aerobic mechanism. Lactate may be used by the heart and brain as a metabolic fuel, suggesting that this is an adaptive mechanism designed to handle physiologic stress.
It remains widely believed that lactate is a measurement of perfusion, systemic oxygenation, and anaerobic metabolism. This is a myth. Among septic patients, the primary cause of lactate elevation is beta-2 agonist stimulation (from endogenous and exogenous epinephrine). Beta-2 agonist stimulation causes the liver to secrete lactate via an aerobic mechanism. Lactate may be used by the heart and brain as a metabolic fuel, suggesting that this is an adaptive mechanism designed to handle physiologic stress.
 Once we understand lactate as an index of endogenous epinephrine, using it as a resuscitation target stops making sense:
Once we understand lactate as an index of endogenous epinephrine, using it as a resuscitation target stops making sense:
- First, let's imagine a young woman who is doing great, after receiving some fluids and norepinephrine. Her blood pressure, urine output, and skin perfusion are excellent. Her lactate is 6 mM, revealing the presence of endogenous epinephrine. Giving her additional norepinephrine and dobutamine can overdrive suppress her sympathetic nervous system, shutting down endogenous epinephrine production. This will reduce lactate, but it probably won't help her. It's basically using exogenous norepinephrine and dobutamine to replace her endogenous epinephrine (which was working perfectly well).
- Second, let's imagine an elderly man who is doing poorly despite receiving fluids and norepinephrine. His heart rate is in the 70s, his urine output is poor, and his extremities are mottled. His lactate is 0.5 mM. This patient is suffering from an inadequate sympathetic response, with a deficiency of endogenous epinephrine. After an epinephrine infusion is started, he improves dramatically with excellent urine output and skin perfusion. However, the exogenous epinephrine causes his lactate to increase to 6 mM. This increase in lactate is actually a positive prognostic sign, indicating that he is likely to improve (Wutrich 2010). Rising lactate doesn't mean that he's getting sicker – it means that the epinephrine is working (2).
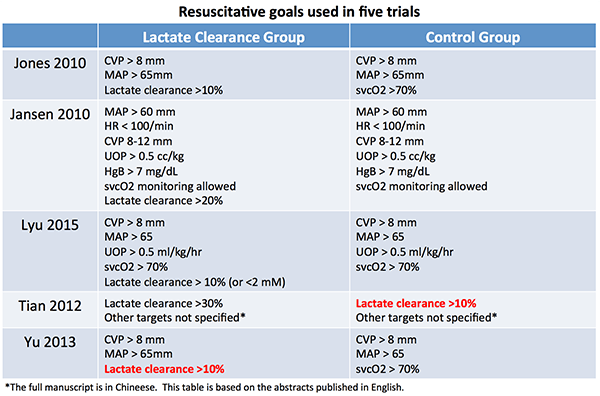
There is no persuasive evidence that trying to “normalize” lactate is beneficial. The new guidelines recommend using lactate to guide resuscitation on the basis of five studies:
- Jones 2010: This showed that chasing lactate was equivalent to chasing svcO2. However, recent studies suggest that chasing svcO2 isn't helpful… so chasing lactate and chasing svcO2 may be equally ineffective.
- Jansen 2010: This prospective RCT found no mortality benefit among patients whose lactate levels were measured. However, a post-hoc adjusted analysis did find benefit.
- The remaining three studies aren't available in English (Lyu 2015, Tian 2012, Yu 2013).
These five studies have been combined into a meta-analysis, showing that targeting lactate clearance was beneficial:
 However, these studies are horrifically heterogeneous. For example, Tian 2012 used lactate clearance >10% in the control group, whereas Yu 2013 used this same goal in the experimental group (table below, red text). It's simply not valid to combine such heterogeneous studies into a meta-analysis.
However, these studies are horrifically heterogeneous. For example, Tian 2012 used lactate clearance >10% in the control group, whereas Yu 2013 used this same goal in the experimental group (table below, red text). It's simply not valid to combine such heterogeneous studies into a meta-analysis.
 Ultimately, the available evidence is limited (3). However, it is doubtful that trying to “normalize” the lactate is beneficial. Septic patients probably aren't supposed to have a “normal” lactate (an example of inappropriate euboxia).
Ultimately, the available evidence is limited (3). However, it is doubtful that trying to “normalize” the lactate is beneficial. Septic patients probably aren't supposed to have a “normal” lactate (an example of inappropriate euboxia).
 Myth #2: All septic patients must receive 30 ml/kg fluid initially.
Myth #2: All septic patients must receive 30 ml/kg fluid initially.

 I recently cared for a patient nearly killed by this concept. A morbidly obese young woman presented to an outside hospital with influenza pneumonia. She met qSOFA criteria due to tachypnea and a blood pressure of 95/60 (her baseline). To comply with CMS regulations, the hospital recently implemented a sepsis order set including 30 cc/kg fluid. The trigger was pulled. Following a single keystroke, she received nearly four liters of saline (dosed per actual weight) plus several IV bags of antibiotics. That pushed her into full-blown ARDS, precipitating a one-week stint on the ventilator while we diuresed her.
I recently cared for a patient nearly killed by this concept. A morbidly obese young woman presented to an outside hospital with influenza pneumonia. She met qSOFA criteria due to tachypnea and a blood pressure of 95/60 (her baseline). To comply with CMS regulations, the hospital recently implemented a sepsis order set including 30 cc/kg fluid. The trigger was pulled. Following a single keystroke, she received nearly four liters of saline (dosed per actual weight) plus several IV bags of antibiotics. That pushed her into full-blown ARDS, precipitating a one-week stint on the ventilator while we diuresed her.
 Let's be honest: nobody really knows the right amount of fluid to give to a patient with sepsis. 30 cc/kg is a reasonable dose for most patients. However, the concept that every patient must receive 30 cc/kg fluid is nuts. For example, septic shock does sometimes coexist with hypervolemia in patients with CHF or pulmonary hypertension (an example of Hickam's Dictum, above).
Let's be honest: nobody really knows the right amount of fluid to give to a patient with sepsis. 30 cc/kg is a reasonable dose for most patients. However, the concept that every patient must receive 30 cc/kg fluid is nuts. For example, septic shock does sometimes coexist with hypervolemia in patients with CHF or pulmonary hypertension (an example of Hickam's Dictum, above).
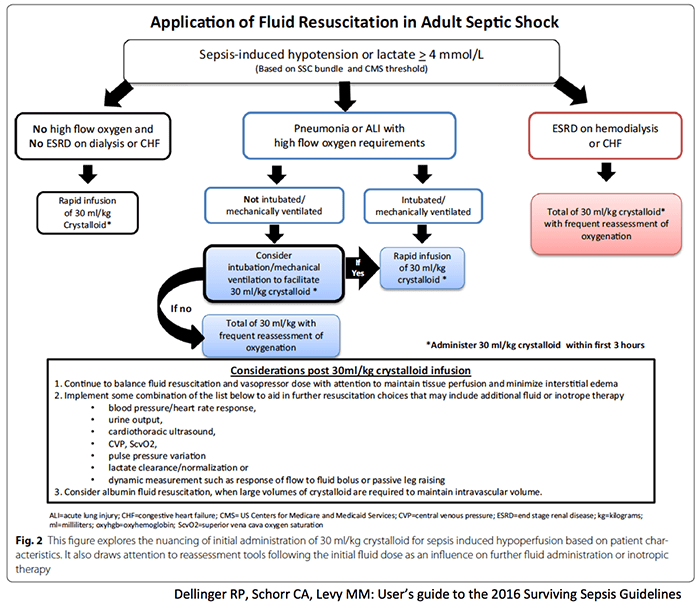 The above algorithm may be frankly dangerous. For example, consider the recommendation that a patient with ARDS and either hypotension or hyperlactatemia may be intubated to facilitate fluid administration (4). This is dubious for many reasons:
The above algorithm may be frankly dangerous. For example, consider the recommendation that a patient with ARDS and either hypotension or hyperlactatemia may be intubated to facilitate fluid administration (4). This is dubious for many reasons:
- We must always consider the entire patient to answer the key question: what physiologic process represents this patient's greatest life-threat? For many patients with ARDS and mild hypotension/hyperlactatemia, their primary life-threat is ARDS. In that case, the risk of large-volume resuscitation outweighs the possible benefit.
- Intubation, sedation, and positive-pressure ventilation typically cause patients to become more hemodynamically unstable. In many cases, the amount of hemodynamic instability caused by intubation and sedation will outweigh any hemodynamic benefit from 30 cc/kg fluid.
- There is no evidence to support the practice of pre-emptive intubation to facilitate fluid loading in the context of ARDS. If anything, evidence might suggest the opposite: diuresis to facilitate extubation (FACTT trial).
Myth #1: It's helpful to mandate that specific sepsis therapies be given within a rigid time frame.
 It is widely believed that early antibiotics are essential, with each hour being critical. This is based on retrospective studies which correlate the delay to antibiotics with outcome. However, delay to antibiotics also correlates with numerous confounders (atypical clinical presentation, mental status alteration, day of the week, time of day, delay to other treatments, etc.). These correlational studies should be used only for hypothesis generation.
It is widely believed that early antibiotics are essential, with each hour being critical. This is based on retrospective studies which correlate the delay to antibiotics with outcome. However, delay to antibiotics also correlates with numerous confounders (atypical clinical presentation, mental status alteration, day of the week, time of day, delay to other treatments, etc.). These correlational studies should be used only for hypothesis generation.
To make matters even muddier, studies disagree. A meta-analysis detected no benefit from early antibiotics (Sterling 2015). Ultimately, there is no scientific answer to this question (5).
However, let's suppose that earlier antibiotics do help (probably true). The next question is whether it is beneficial for guidelines to mandate that antibiotics be given within a certain time-frame. This may accelerate care, but it may also force practitioners to cut corners. On the balance, is this helpful? What is better: fast and sloppy care, or slow and accurate care? This, too, is unknown.
A cautionary tale is provided by the case of antibiotics in pneumonia. Retrospective studies in 1997 and 2004 suggested a correlation between reduced mortality and antibiotics administration within four hours. Subsequently, numerous regulatory bodies adopted this as a quality benchmark. Over the following years, it was shown that this benchmark increased misdiagnosis and inappropriate antibiotic use. Finally, the four-hour benchmark was abandoned.

- We have a history of over-estimating our knowledge of sepsis and the benefit of our interventions.
- Acknowledging uncertainty is uncomfortable, but it may ultimately make us more thoughtful and flexible clinicians.
- We need to be honest with ourselves about what is actually known about sepsis therapy (which is surprisingly little). For example:
- Intentional double-coverage of gram-negative bacilli to achieve synergy has no proven benefit.
- Norepinephrine is a good vasopressor, but it is unclear whether it is the best drug for every patient. The ideal drug selection and dose is unknown.
- Lactic acid is not a reliable measurement of tissue perfusion. It is doubtful that using lactate as a resuscitation endpoint is beneficial.
- Nobody knows how much fluid should be given to septic patients or how quickly it should be given.
- The benefit of early therapy is unproven. Insufficient evidence exists to make any concrete recommendation regarding the timing of interventions.
More information
- Surviving Sepsis 2016
- Full guidelines (PDF)
- Users’ Guide to the Guidelines (PDF)
- Podcasts from EMCrit and FOAMcast
- Blog from PulmCCM (Jon-Emile Kenny)
- Myth #6, Combination therapy for gram-negatives
- Myth #5, NE best vasopressor for everyone
- Renal microvascular hemodynamics & vasopressin (PulmCrit)
- Renoresuscitation, vasopressin, vepinephrine & VANISH (PulmCrit)
- Phenylephrine infusions: not pure evil? (PulmCrit)
- Myth #4, Blind sequential vasopressor addition
- Epinephrine challenge in sepsis (PulmCrit)
- Myth #3, Lactate abuse
- Understanding lactate and using it to our advantage (PulmCrit)
- Understanding lactate: SMACC talk (Marik)
- SMACC-Back on Marik & Lactate (EMCrit)
- Euboxia & Ab(Normality) (LITFL, Nickson)
- Myth #2, 30 ml/kg fluid for everyone
- Marik Fluid Lecture (Marik on EMCrit)
- Renoresuscitation: Sepsis resus to avoid long-term complications (PulmCrit)
- Mythbusting: Empty IVC plus hyperkinetic heart doesn't equal volume depletion (PulmCrit)
- Myth #1, Timing dogma
Notes:
- Combination therapy is evidence-based for management of severe pneumonia (azithromycin + beta-lactam) and toxic shock syndrome (clindamycin + beta-lactam). However, the use of combination therapy for gram negatives isn't.
- I've seen this many times, and it's generally a beautiful phenomenon. The lactate spikes in response to epinephrine, and often patients improve a lot and come off vasopressors entirely within the next 24 hours.
- The most meaningful question is whether trending lactate would be beneficial after we stop measuring CVP. None of these trials answer that question (all were performed in the bygone era of early goal-directed therapy).
- The disease previously known as ALI (Acute Lung Injury) has now been re-defined as ARDS.
- It would be nearly impossible to design a RCT to test this, using time as an independent variable.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
However the biggest problem in all of this is Medicare. I’m constantly butting heads with the RN sepsis coordinator at my hospital because, “Well, Medicare says X.” When you try to show why a case doesn’t fit to Medicare standards or use more evidence based medicine (even simply implementing Sepsis 3, for all of it’s warts), the only thing I hear is, “LOL, Medicare don’t care.”
yep, CMS and other “quality metrics” are continually lagging behind the current evidence.
I’m learning a lot from your blog, thanks for the fantastic post! I completely agree with your interpretation of the literature, and deeply disagree with turning little pieces of data into official policy, which at best impairs progress, and at worst kills patients. On the other hand, rather than trash the Rivers study, as a scientist, I prefer to see it as a stepping stone in our path towards truth. Though it has its faults, painting it as flimsy/shady and clouded by COI is misleading in itself, and minimizes the huge efforts made by Rivers and others to bring sepsis… Read more »
Agree, however part of being a scientist is also admitting when we are wrong, and when something has been disproven. From a scientific standpoint, recognizing that something is incorrect is enormously important (perhaps more important than discovering a new piece of information).
maybe, the best PULMcrit ever!!
Thanks!!
Excellent perspective on a difficult problem, in which the push to meet quality metrics far outpaces our knowledge needed to answer important questions. Provides more questions than answers.
With regard to how much fluids, dynamic indices and PLR manuevers with ultrasound evaluation are becoming more popular. Michael Pinksky’s work shows that even volume overloaded pts may be fluid responsive however, he proposes measuring the mean systemic filling pressure I strongly urge you to do a PULMcrit on this. It can easily be done at the bedside with a bit of kowledge and patience.
There’s already a lot of great stuff on this, currently I don’t have much to add to the EMCrit podcast on this: https://emcrit.org/podcasts/assessing-fluid-responsiveness/
…not to mention that fluid responsiveness neither equates to fluid being the best option, nor to the patient being fluid tolerant…
😉
P
Ok, I am an EM Intensivist in Indiana and most of my time is spent in the Medical ICU. I will start this response by saying I trained with Dr. Rivers and he was a huge Mentor for me. He would always say to me “the only ones who have time to rock the boat are the ones not rowing.” I feel that this is one of those articles that “rocks the boat,” being that it goes extensively into critizizing every aspect of the Surviving Sepsis Campaign without offering any alternatives. Yes I agree that CVP is Dead and many… Read more »
If you’re not interested in rocking the boat, you’re reading the wrong blog.
Unfortunately when Rivers’ study had more than 250 included in the statistically analysis (which it did) is was no longer statistically signficant. Fortunately, the research coordinator that left his positition was courageous enough to inform those including at the NIH of this “doctored data.” Rivers’ tried to control the stream in his own river. Nothing to be proud of and dangerous to the rest of the field.
Terrific post. Your take on Myth #5 is the most elegant distillation of “vasopressor choices” that I’ve read, and really sums up my own (haphazard, less fully articulated) interpretation of the literature as well. Gonna use that one as a teaching tool!
Additionally in point 6, your screen shot shows that they still recommend antimicrobial de-escalation (ADE) for both culture positive and negative infections.
We recently showed that all the evidence on this was biased and that there is no proof that there is any beneficial effects of ADE on antimicrobial resistance as this has never been studied. ADE may actually cause an increase in the total duration of antimicrobial therapy and have an effect opposite to what is expected.
anyway, thanks for your blog, always a pleasure to read…
https://academic.oup.com/cid/article-lookup/doi/10.1093/cid/civ1199
Can I thumbs up this reply?
Thanks. Great post. This needed to be said.
And yes it’s better than nothing but it’s not gospel.
The goal is to get it right so nothing wrong with rocking the boat
According to CMS measures, are there ways we can get around giving a full 30cc/kg bolus if patients have lactate >4 or hypotension. If a patient is in acute CHF or ESRD with overload, do we still have to intubate/prepare to intubate and give the bolus, or can we write something in the chart to get around this? We can deviate from sepsis protocol for dnr/dni patients but any other way to skirt the rule of the land?
no
Well, except you are allowed to include antibiotic dilution volume and prehospital fluid (with onerous documentation) and the “patient or authorized patient advocate” can refuse the full 30 mL/kg. Perhaps an opportunity for shared decision making…
Yes, there is a “way to skirt the rule”. CMS says you must give the 30 cc/kg bolus, HOWEVER, there is no specified time frame over which you must give the bolus as long as it’s greater than 125 cc/hr?!. I found this important caveat as I am the sepsis monkey at my hospital and have tried to make sense of all of this…I can’t, but I am in the trenches trying to help my patients and I spent a lot of time researching. So here it goes said another way. CMS requires the fluids for any and all patients,… Read more »
From CMS: Question 6: In patients that have congestive heart failure (CHF) with ejection fraction of < 35, are Crystalloid fluids of 30 ml/kg still recommended? Answer 6: Yes, the measure does not exclude cases from the 30 ml/kg crystalloid fluid infusion. Trials of fluid administration for severe sepsis and septic shock have included cases with co-morbitities, such as CHF, and have not noted any deleterious effects from the fluid infusion. We are not aware of any studies of severe sepsis and septic shock indicating that fluids should not be given for cases with co-morbidities such as these. There are… Read more »
i thought the 30/kg had to be given in the first 3 hours? NO?
Don, CMS says the fluids must be STARTED in the first 3 hours of septic shock presentation. Not totally infused in that time frame (I know it seems odd). CMS states “there is not a required time frame or rate for infusion of the fluids, other than a minimum rate or time frame equivalent to greater than 125 ml/hour. Below this rate, the fluids are considered for IV maintenance rather than for fluid resuscitation.”
Yes, there is a “way to skirt the rule”. You must give the 30 cc/kg bolus, HOWEVER, there is no specified time frame over which you must give the bolus as long as it’s greater than 125 cc/hr?!. I found this important caveat as I am the sepsis monkey at my hospital and have tried to make sense of all of this. (Good luck!) CMS requires the fluids for any and all patients, yes, even with CHF or ESRD!! But, as long as you give the fluid at a rate greater than 125 cc/hr, it counts!! Isn’t that insane?! Don’t… Read more »
“small community ERs and hospitals who don’t have any idea of what they are doing”
This is exactly the sort of patronizing and dismissive attitude I’ve come to expect from university hospital doctors and other so-called “centers of excellence.” The arrogance and anger that are triggered whenever someone with a significant amount of clinical experience challenges their dogma is impressive, but does nothing for progress in medicine.
Agree. Some people have defended the surviving sepsis guidelines by arguing essentially “well, they aren’t perfect, but they’re good for uninformed small community-hospital docs who don’t know any better.” I’ve never agreed with that concept. I would argue that the guidelines should make whatever recommendations are supported by good evidence (and nothing more). This will leave lots of gaps, which is OK. Then, physicians can be left to fill in the gaps based on their own experience, setting, and practice.
From a nursing perspective, this was very interesting especially in relation to myth 2. I always found it insane that we have to give 30 cc/kg of fluids to a septic patient who is in heart failure, and now learning that the recommendation is based low-quality evidence, it seems even more insane to me. If the patient does truly need the full 30 mL/kg, it would make more sense to me to infuse it slowly and see how they tolerate it rather than infuse rapidly and diurese or intubate them.
There are some interesting arguments for infusing fluid more slowly, rather than giving it as a bolus. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3396245/.
Such a great post Josh!
Re: #2, #4, #5: I have found no more powerful guide than Echo to help answer these questions for the patient in front of me. Then just a few quick follow-up views to assess response gives me a real sense of pathophysiologic evolution.
Sam
Completely agree. My main strategy for trying to understand hemodynamics is echocardiograph and challenging the patient with various therapies (e.g. careful fluid challenge, vasopressor challenge, etc).
We still must work towards consensus. It doesn’t mean that on individual basis clinical judgement should not be applied while decision making.I feel the post is too much out of context.Im not saying everything you saying is wrong but the post should have been mild rather labelling everything as a myth.
It’s doubtful that any consensus on septic shock management will be reached during our lifetimes (if so, it would probably be a sign of the coming of the apocalypse).
Scientific consensus has no bearing on fact. If the research upon which the recommendations were based is faulty or incomplete, then the label of, “Myth,” seems more than appropriate.
My only comments are that you should be on the SSCG committee to shape the future guidelines. I believe this will be very important.
Thanks, that’s very generous.
The problem is, “Early Goal-Directed Therapy” and “Any protocol involving early identification and intensive care of septic patients probably would have worked” (see article) is saying, essentially, the same thing. But nobody had demonstrated that, in a randomized experiment, until Rivers did. EGDT showed that the STANDARD TREATMENT of the time, which was what was applied to the control group, was inferior to EGDT. That was the clinical question and it was answered. The 16% absolute survival advantage in the EGDT cohort, compared to the “usual” care controls, accrued to those in shock with impending CV collapse, not late deaths… Read more »
There is an enormous operational difference between:
(1) saying that sepsis patients require prompt, thoughtful, and flexible intensive care
(2) saying that sepsis patients need CVP>12, HgB>10, svcO2>70%, etc (all goals of EGDT)
Excellent job here Josh. Always best to have “strong recommendations” based on “weak evidence” challenged by deliberate and thoughtful dissent. I especially like the attack on the absolute 30 cc/kg rule and absolute preference to norepinephrine, but are you sure you didn’t go after lactate as a surrogate just to make six myths out of five? We all watch it with anticipation for a reason. In a plea to all the people complaining about absolute CMS metrics, I urge them to voice their concerns and arguments to Sean Townsend at TownseSR@sutterhealth.org. He is often promptly responsive to rational and collegial… Read more »
Thanks, Gil. Let me clarify my thoughts on lactate a bit. (1) Lactate is great for identifying sick patients with sepsis (solid evidence, I don’t think anyone argues that). (2) Cycling lactate in patients not receiving epinephrine can provide some sense of the direction of resuscitation. When the lactate goes down this is reassuring. If the lactate doesn’t go down, this is a signal to globally re-consider the patient (look for additional foci of infection, echo the patient, re-consider antibiotic choices, look at urine output, look at skin perfusion, etc.). (3) I will sometimes cycle lactate in sepsis patients who… Read more »
I am an ICU nurse with experience working in academic centers and community hospitals. I enjoy your articles but I can relate to what Matthew describes. In my experience you don’t need a protocol at large referral centers because the patient is being swarmed by residents, fellows etc. At smaller facilities with limited resources a resus protocol can at least get things moving. Rather than a 250ml bolus or some other symbolic intervention- the sepsis protocol gives me some tools to work with: central line, fluids, norepi. At least it provides a minimum level of care. If you have a… Read more »
Agree with using lactate as a screening tool to identify critically ill patients, absolutely.
Sepsis protocols are better than nothing, but I would still argue that they shouldn’t be a replacement for attentive patient care. Sepsis has a mortality higher than STEMI, so if smaller hospitals aren’t able to provide enough attention to these patients then they should probably transfer them to a place that can.
Hi Folks, Whenever I speak on SEP-1 I make at least two points, but often more, so be prepared for a long post. In fact, I had to do it in more than one post because it wouldn’t let me do one. Part 1: First, the measure is in a stabilization phase. This is why hospital results are not publicly reported, for instance. We are highly committed to updating the measure to better reflect what’s necessary for care. We have made innumerable changes to the measure since its release at version 5.0 and we will release 5.3 in Jan 2018.… Read more »
Part 2: I won’t address all the points in this blog post here, but for a couple of items I will. As mentioned by another post, maligning EGDT and its impact in promoting protocolized care fails to acknowledge that Dr. River’s study shifted the landscape on how we treat sepsis. EGDT was not perfect and reasonable clinicians can debate the various components cordially. What is not debatable is that EGDT helped us adopt a systematic approach to caring for sepsis patient that has helped improve sepsis care nationally. We must remember that protocol based sepsis care was not the norm… Read more »
Part 3: I must say every option will have their ups and downs, and proponents and detractors. A supermajority of the time the current standards apply, maybe even much more often than that. The measure specifications are the right thing to do for most patients. It’s not perfect but we are committed to improving it. On other items like double covering gram negatives, SEP-1 doesn’t mandate that. Lactate clearance may be helpful in the better papers published. SEP-1 doesn’t tell you to normalize lactate, just check it again, do with it what you like. We don’t tell you what vasopressor… Read more »
Thanks for your comments. First, I should note that the CMS core measures do seem to be further increasing awareness of sepsis. This is leading to more widespread screening for sepsis, broader measurement of lactate among patients in the ED, and earlier involvement of critical care in these patients. I think we could all probably agree that those are positive developments which will likely improve patient outcomes. I maintain that there is no level-I evidence dictating how much fluid should be given to patients with septic shock. Liu 2016 (https://www.ncbi.nlm.nih.gov/pubmed/26695114) is a retrospective study showing that implementation of a sepsis… Read more »
Hi Jeff, I am an intensivist and finished training in 2000 so I can certainly speak to many of your contentions on the current standards of care in sepsis management. I am astounded by your global condemnation of the River’s NEJM article and the cardinal principles of critical care which he advocated NOT invented. Dr Rivers was a student of Max Harry Weil MD one of the founding Fathers of critical care medicine. Dr Weil published extensively on mixed venous saturation validity in animal and human models throughout the 1980 and 1990’s. He help conceptual the Rivers study. The concept… Read more »
First, I’m not trying to malign Dr. Rivers. I’m not impugning his intentions, merely challenging the conclusions of his study. The PROCESS trial and other similar trials (ARISE, PROMISE) represent enormous advances in the study of septic shock, which have rightly had major effects on current sepsis therapy. The failure of these trials to find patients with low svcO2 suggests that Rivers cohort of patients may have represented an anomaly. Rivers is non-replicatable, and such studies cannot be accepted as scientific fact. Early goal-directed therapy was built upon the following concepts, all of which I believe will eventually be proven… Read more »
Unfortunately these assertions are false. Many folks have attempted to replicate Rivers’ study well before Process, Promise, and Arise in smaller fashion. The Only aspect of the guidelines that actually demonstrate any benefit is early antibiotics. Many careful evaluations by various meta-analyses have yet to find good evidence for anything but antibiotics. I’m assuming you havent read Holst et al or Murthy et a. for transfusion. We do live in an age of alternative facts and it is very discouraging when folks continue to propegate these myths via studies that everyone that actually is a sepsis investigator knows were flawed… Read more »
Excelente post. Más datos para enfrentar este problema diario.
How do you handle the CMS requirements regarding septic Shock and lactate over 4? We are told that there is no way out of giving 30cc/kg other than convincing the patient to refuse and documenting this. Just saying you are concerned with fluid overload is not adequate even if you start vasopressors early. Also giving fluid based on ideal or adjusted weight is not an out. So you have to treat every kg of fat with water.
don
If I read the 2018 Core Measure update correctly they are INCREASING the number of patients who require 30 ml/kg. Rather than just people defined as “Septic Shock” it now appears that anyone with “initial hypotension” must get 30 ml/kg.
Nothing to disclose. (but you have to wonder if Baxter is involved in these measures)
Thanks Josh, great post. My first comment. For a couple years now we have been teaching our aeromedical crew at STARS that lactate is not just about anaerobic metabolism and a significant portion of its level is likely from B2 stimulation via endogenous catecholamines. You seem to imply above that all the lactate is produced in this fashion. Could their not be some mitochondrial dysfunction in septic patients resulting in impaired ability to utilize oxygen and thus some component of anaerobic metabolism contributing to some of that lactate level? Again, great post, looking forward to your reply.
Josh – Thank you for an excellent distillation of the data and a very approachable way to explain the trends in the science. What are your thoughts about the organization of Sepsis Response Teams in hospitals. On the one hand, it is a resource to bring attention to potentially sick patients, objectively assessed by a score. On the other hand, it is a protocol and will likely have some of the difficulties you mention – fluids, antibiotics given in great amounts and quickly. There is some fairly dirty data that suggests it may be helpful but where do you come… Read more »