 Introduction with a case
Introduction with a case

A 70-year-old man was admitted with sepsis due to liver abscess. Over the first two hospital days his platelet count decreased from 122 to 39. Prophylactic heparin was held due to concerns about bleeding risk. Additional coagulation studies showed a D-dimer of 1221 ng/ml, a fibrinogen of 672 mg/dL, and the following thromboelastograph:
As a reminder from a prior post:
 Based on the thromboelastograph, his prophylactic heparin was re-started. The next day he developed hypoxemia, leading to a diagnosis of submassive pulmonary embolism. An evaluation for heparin-induced thrombocytopenia was negative.
Based on the thromboelastograph, his prophylactic heparin was re-started. The next day he developed hypoxemia, leading to a diagnosis of submassive pulmonary embolism. An evaluation for heparin-induced thrombocytopenia was negative.
Some points illustrated by this case:
- Despite thrombocytopenia, patients with sepsis are often hypercoagulable.
- Thromboelastography reveals the overall balance of coagulation better than an isolated lab test.
The concept of fibrinogen-platelet function
It remains widely believed that a thromboelastograph tracing can be interpreted as follows:
- Maximal amplitude = measurement of platelet function
- Alpha-angle = measurement of fibrinogen function
This doesn’t appear to be true (Solomon 2015). Instead, both the maximal amplitude and the alpha-angle are a reflection of the combined function of fibrinogen and platelets:
- Maximal amplitude = measurement of fibrinogen & platelet function
- Alpha-angle = measurement of fibrinogen & platelet function
This raises the possibility that the same phenomenon could occur en vivo, with platelets and fibrinogen working in a synergistic fashion. It is possible that only the composite fibrinogen-platelet function matters. For example:
- High fibrinogen levels could compensate for thrombocytopenia.
- A patient with a reduced maximal amplitude who is bleeding could potentially be treated with either fibrinogen or platelets.
Interactions between platelets and fibrinogen can be understood using the Chemistry concept of reaction velocity. Platelets and fibrinogen are the main structural components of a clot. Thus, we can write the following equation to describe clot formation:
[Platelets] + [Fibrinogen] –> Clot
The reaction velocity of this chemical process would be described by the following equation, where k is a constant:
Reaction velocity = k[Platelet concentration][Fibrinogen concentration]
This explains mathematically why platelet and fibrinogen levels may, to some extent, be interchangeable.
The concept of fibrinogen-platelet function is theoretical at this point, but it explains some otherwise confusing events. For example, the patient described above developed a pulmonary embolism, despite severe thrombocytopenia. This may be explained because his fibrinogen level was quite high, thus effectively negating his thrombocytopenia.
The concept of sepsis-associated DIC (S-DIC)
Disseminated intravascular coagulation (DIC) refers to a broad range of situations where coagulation becomes dysregulated, causing diffuse coagulation. In some cases, this consumes coagulation factors, leading to bleeding. Trying to understand DIC is difficult, because it is a mixed bag. There are fundamental differences between different diseases causing DIC, for example:
- Hemorrhage is often seen with DIC due to obstetric catastrophe or leukemia.
- Thrombosis is often seen with sepsis-associated DIC.
Focusing on sepsis-associated DIC may isolate a more homogeneous entity, which is a bit easier to understand.
Overview of sepsis-associated DIC
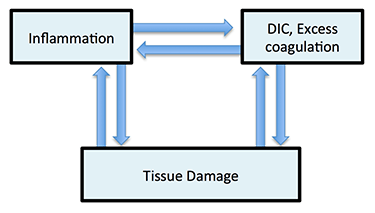 S-DIC may be conceptualized as shown on the right. There are numerous molecular pathways whereby inflammation may cause hypercoagulation, and hypercoagulation may in turn trigger cytokine release and inflammation (Levi 2014). This generates a vicious spiral involving excessive inflammation and hyper coagulability. Diffuse coagulation may lead to microvascular thrombosis which impairs perfusion, causing tissue damage.
S-DIC may be conceptualized as shown on the right. There are numerous molecular pathways whereby inflammation may cause hypercoagulation, and hypercoagulation may in turn trigger cytokine release and inflammation (Levi 2014). This generates a vicious spiral involving excessive inflammation and hyper coagulability. Diffuse coagulation may lead to microvascular thrombosis which impairs perfusion, causing tissue damage.
S-DIC is common among patients dying from septic shock. It correlates with organ failure and poor prognosis. In animal models of sepsis, inhibition of S-DIC can improve survival.
S-DIC is different from some other forms of DIC because inflammation induces the synthesis of fibrinogen (Koami 2016). Unlike other types of DIC, patients with S-DIC have normal or elevated fibrinogen levels. This tends to make patients with S-DIC more hypercoagulable than many other forms of DIC.
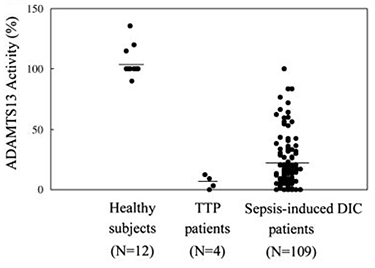
S-DIC may lead to degradation and deficiency of ADAMTS13 (figure below; Ono 2006). Low ADAMTS13 levels may cause a thrombotic microangiopathy, similar to spontaneous thrombotic thrombocytopenic purpura (TTP).
 Diagnosis of sepsis-associated DIC
Diagnosis of sepsis-associated DIC
Diagnosis of DIC among septic patients is slippery for several reasons. First, there is no clear definition or gold standard of DIC (but rather, numerous proposed scoring systems). Second, DIC isn’t an all-or-none diagnosis, but instead includes a range of abnormalities. For example, the term “non-overt DIC” is often used to describe patients with subclinical coagulopathy.
S-DIC causes the following lab abnormalities:
- Fibrinogen is usually normal or elevated. Numerous studies of S-DIC contain no report of any patient with reduced fibrinogen (Kaomi 2016, Kander 2016, Panigada 2015, Ostrowski 2013, Sivula 2009).
- INR is mildly elevated.
- D-dimer is markedly elevated (usually >1,000 ng/mL)( Panigada 2015).
- Platelet count is generally decreased, but not below 30,000/mm3 (Haase 2015, Massion 2012, Panigada 2015, Ostrowski 2013, Sivula 2009).
The main source of diagnostic confusion is usually differentiating S-DIC vs. heparin-induced thrombocytopenia. Timing is often helpful here, with S-DIC being a gradual process that usually occurs shortly after admission. In contrast, heparin-induced thrombocytopenia tends to lead to an abrupt fall in platelet count >5 days after admission.

Purpura fulminans is a particularly malignant form of S-DIC associated with hemorrhagic infarction of dermal arteries. This produces a characteristic pattern of confluent purpura which progresses to gangrene, typically involving the extremities. Purpura fulminans is most often caused by profound bacterial sepsis (particularly meningococcus and pneumococcus). One report detected low ADAMTS13 levels in two patients with purpura fulminans, suggesting that this disease could represent an overlap syndrome between S-DIC and sepsis-induced thrombotic thrombocytopenic purpura (TTP)(Wang 2011).
Thromboelastography in sepsis-associated DIC
Thromboelastography would be expected to help understand a patient with S-DIC for two reasons:
- DIC may cause consumption of both clotting factors and endogenous anticoagulants (e.g. protein C, antithrombin III). Clinically, coagulation depends on a balance of clotting factors vs. endogenous anticoagulants. However, INR only tests the level of clotting factors (revealing nothing about endogenous anticoagulants). In contrast, TEG may reveal this balance (reflected in the R-time).
- Patients with S-DIC may have thrombocytopenia and elevated fibrinogen. The maximal amplitude on the TEG may help elucidate the overall platelet-fibrinogen function.
Patients in S-DIC may be very roughly categorized into three TEG patterns (table below; Ostrowski 2013, Sivula 2009). Most patients have a hypercoagulable or normocoagulable pattern, due to elevated fibrinogen levels. In the sickest patients, consumption of fibrinogen and platelets shifts the balance towards a hypocoagulable state.
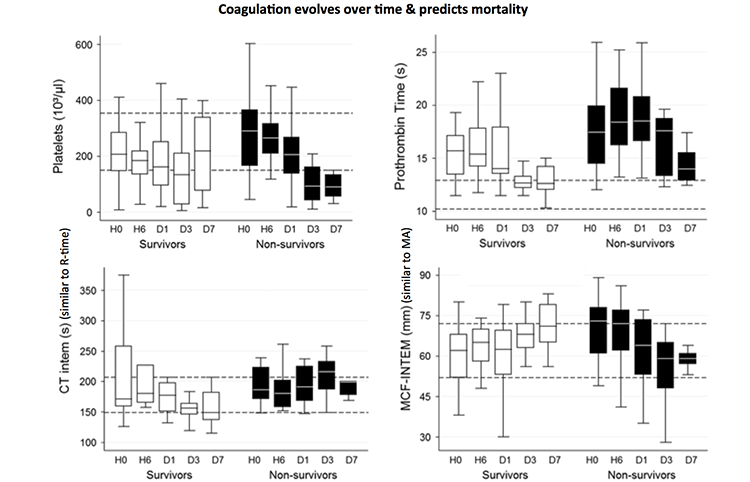
 Coagulopathy my evolve in parallel with changes in the patient's condition. Massion 2012 evaluated serial thromboelastometry among patients in septic shock (1). Survivors tended to become more hypercoagulable, whereas non-survivors became more hypocoagulable:
Coagulopathy my evolve in parallel with changes in the patient's condition. Massion 2012 evaluated serial thromboelastometry among patients in septic shock (1). Survivors tended to become more hypercoagulable, whereas non-survivors became more hypocoagulable:
 Thromboelastography may be most useful in patients with S-DIC who are bleeding or scheduled for a procedure. Current guidelines recommend attempting to fix all the coagulation parameters (Wada 2013):
Thromboelastography may be most useful in patients with S-DIC who are bleeding or scheduled for a procedure. Current guidelines recommend attempting to fix all the coagulation parameters (Wada 2013):
- Platelet transfusion to target platelets >50,000/mm3
- FFP transfusion to target an INR < 1.5
- Cryoprecipitate or fibrinogen to target a fibrinogen > 150 mg/dL
Thromboelastography might provide deeper insight into the patient's true coagulation status, allowing transfusion in a more intelligent fashion. For example, a patient with thrombocytopenia, elevated fibrinogen level, and a normal maximal amplitude might not actually need a platelet transfusion (platelet-fibrinogen function is preserved, despite absolute thrombocytopenia).
In septic patients, thromboelastometry might be useful in defining transfusion trigger limits, as most patients with less severe coagulopathy are in a hypercoagulation state despite reductions in platelets and coagulation factors –Sivula 2009
 Currently there is no direct evidence to support a TEG-based transfusion strategy for S-DIC (Muuler 2014). However, TEG has been used successfully for intra-operative management of patients with DIC due to trauma and surgery. Given that TEG can handle extremely complex coagulopathies in the operating room, it seems likely that it could do the same in non-operative patients.
Currently there is no direct evidence to support a TEG-based transfusion strategy for S-DIC (Muuler 2014). However, TEG has been used successfully for intra-operative management of patients with DIC due to trauma and surgery. Given that TEG can handle extremely complex coagulopathies in the operating room, it seems likely that it could do the same in non-operative patients.
Treatment of sepsis-associated DIC
#1. Treat the underlying disorder
The key treatment of any form of DIC is to treat the underlying process (in this case, infection). Antibiotics and definitive source control are critical. The presence of S-DIC indicates severe disease which requires aggressive management.
#2. Recombinant anticoagulants?
Activated Protein C (Xigris) and Antithrombin III have failed to show benefit in RCTs of septic patients. Unfortunately, these therapies have never been tested in the subset of patients with S-DIC, so it remains possible that they could benefit such patients. In Japan there seems to be greater enthusiasm for such treatments (with frequent use of Antithrombin-III; Iba 2014).
#3. DVT prophylactic dose heparin
DVT prophylaxis is conventionally feared among patients with a platelet count below 50,000/mm3. However, patients with S-DIC and thrombocytopenia may be hyper coagulable. Furthermore, anticoagulation could theoretically diminish the consumption of clotting factors, thereby improving the DIC and reducing inflammation (Iba 2014).
Regardless of thrombocytopenia, thromboprophylaxis is mandatory in patients with acute promyelocytic leukemia and in patients with DIC in intensive care units –Tufano 2011
A recent multi-society guideline recommended DVT prophylaxis with unfractionated or low molecular-weight heparin in critically ill, non-bleeding patients with DIC (Wada 2013). This guideline cited the XPRESS trial as demonstrating the “importance of not stopping heparin in patients with DIC and abnormal coagulation parameters.”
What about patients with profound thrombocytopenia? In several studies of S-DIC, the platelet count always seems to be above 30,000/mm3. DVT prophylaxis seems reasonable among patients with S-DIC and a platelet count above 30,000/mm3 (2). Patients with more severe thrombocytopenia may have an alternative diagnosis and require further evaluation.
#4. Therapeutic dose heparin
Heparin has been trialed as a therapy for patients with septic shock, without success. Anticoagulation with heparin is indicated for patients with clinical evidence of thrombosis (e.g. DVT).
#5. Blood products
Patients with DIC may develop very abnormal coagulation tests. Asymptomatic patients generally shouldn't be treated with blood products in efforts to “normalize” labs.
One fear is that providing blood products could “feed the fire” and worsen DIC. It is unknown whether this occurs. Platelet transfusion may be harmful in patients with thrombotic thrombocytopenia purpura (TTP), implying that it may also be harmful for septic patients with a secondary deficiency of ADAMTS13 causing thrombotic microangiopathy.
Blood products may be indicated for clinical bleeding or a planned procedure. Product administration can be guided by traditional coagulation labs or thromboelastography, depending on whether your training is in anesthesiology or internal medicine (see: silo coagulation paradox above).
#6. Purpura fulminans
Optimal treatment of this rare condition is unknown. Coagulation derangements may be too extreme to respond to simple therapies (for example, antithrombin-III consumption may cause heparin resistance)(3). Plasma exchange (using FFP as a replacement) is theoretically attractive as an approach to restore levels of pro- and anti-coagulant proteins, thereby re-establishing hemostatic balance. The suggestion that these patients may be suffering from a microangiopathy due to low ADAMTS13 levels would further support the use of plasma exchange (by analogy to therapy for thrombotic thrombocytopenic purpura; Schwameis 2015). If plasma exchange is unavailable, resuscitation using fresh frozen plasma may considered (Saraceni 2013). Adrenal gland infarction may occur, requiring steroid replacement (Hale 2016).
[✍️Editor's note: updated information on the treatment of purpura fulminans is here.]

- Sepsis-induced DIC is distinct from other types of DIC.
- S-DIC doesn't cause low fibrinogen levels. It is generally noticed due to a thrombocytopenia.
- Despite thrombocytopenia, most patients with S-DIC are hyper-coagulable or norma-coagulable. The sickest patients are hypocoagulable, indicating poor prognosis.
- Patients with S-DIC and platelet count >30,000/mm3 should receive DVT prophylaxis.
- Blood products should generally be avoided in patients with S-DIC who aren't bleeding.
- Purpura fulminans is an extreme form of S-DIC which may require more aggressive therapy.
Related
Notes
- Thromboelastometry (ROTEM) is similar to Thromboelastography (TEG), being more popular in Europe.
- One reason for the safety of heparin here is that among the patients with the most advanced S-DIC who are hypocoagulable, levels of antithrombin-III will be decreased the most and this will reduce the efficacy of heparin (heparin works via synergy with anti-thrombin III). Theoretically it might make more sense to use a low-dose oral Xa inhibitor (e.g. riveroxiban) in these patients, as that medication could function independent of the antithrombin-III levels.
- Heparin acts via augmentation of Antithrombin-III, and endogenous anticoagulant protein. However, Antithrombin-III is consumed by S-DIC. With low levels of antithrombin-III, heparin may have little biologic effect.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Would love to see a section on SJS/TEN at some point
I am hoping to get some insight on a potential septic DIC patient, who was also on Eliquis for afib, doctor initially saw hgb 6.5 and platelets of 30 and wanted kcentra, after taking a deeper dive i saw the pts ddimer was sky high, INR 5, aPPT elevated, and clearly in sepsis (later found to be due to cholangitis), also with acute liver failure and aki on ckd. I rec to not give 4 factor PCC and order dic panel including fibrinigen, and only replacing platelets or cryo if surgery was needed or if plts dropped further. Not many… Read more »