
Let's be honest, our decisions to cover MRSA among patients admitted to the hospital with pneumonia are haphazard. It's not our fault. The guidelines are contradictory. For example, the MRSA guidelines by the Infectious Disease Society of America recommend coverage for everyone admitted to the ICU with pneumonia. However, pneumonia guidelines by the same society recommend coverage only for patients with specific risk factors.
A disorganized approach promotes under- and over-treatment:
- Some providers (“MRSA enthusiasts”) treat nearly every patient with healthcare-associated pneumonia and every patient admitted to the ICU for MRSA.
- Other providers (“MRSA skeptics”) are much more selective in who they cover for MRSA, risking under-treatment (1).
Fortunately, new evidence and diagnostic tools may allow us to properly treat MRSA, without drowning the entire hospital in vancomycin.
Underlying problem: Over-diagnosis of MRSA pneumonia
MRSA commonly colonizes the upper airway of asymptomatic people. Imagine that a person colonized with MRSA develops pneumonia with an organism that is difficult to detect (e.g. mycoplasma or viral pneumonia). The patient's sputum may be contaminated with MRSA from their upper airway, leading to an incorrect diagnosis of “MRSA pneumonia.” MRSA is easy to culture, so detecting MRSA contaminant may be easier than detecting the true pathogen. Among pneumonia patients with sputum or endobronchial cultures positive for MRSA, >80% don't appear to have a true MRSA pneumonia (Enomoto 2016, Kawanami 2016)(2).
Most research ignores over-diagnosis. Therefore, as you read the rest of this post, keep in mind that:
- The true incidence of MRSA pneumonia is probably lower than reported rates.
- The sensitivity of diagnostic tests for MRSA pneumonia is probably higher then reported (over-diagnosis tends to inflate the denominator of sensitivity calculations, artificially reducing sensitivity).
- The likelihood of missing a case of MRSA pneumonia is lower than we think (due to #1 and #2).
The remainder of this post will attempt to construct an algorithm, starting with the components.
Component #1: Shorr score
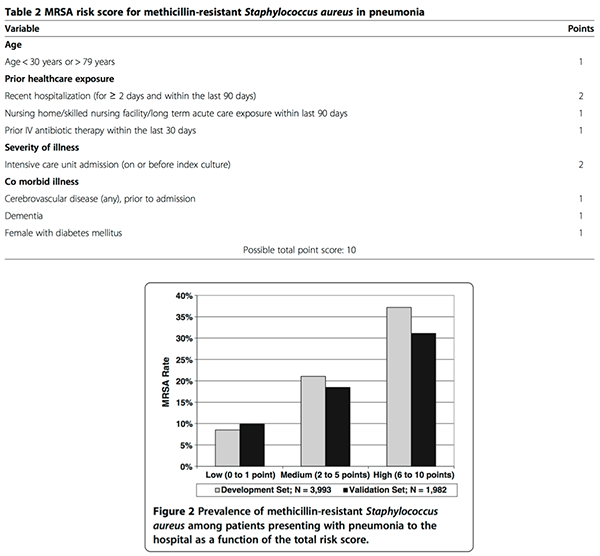
Shorr 2013 performed a retrospective study of 5975 patients admitted to 62 hospitals with pneumonia. Two thirds of this group were used to derive a predictive model for MRSA pneumonia, which was then tested on the remaining third. As shown below, the score divided patients into three tiers of risk:
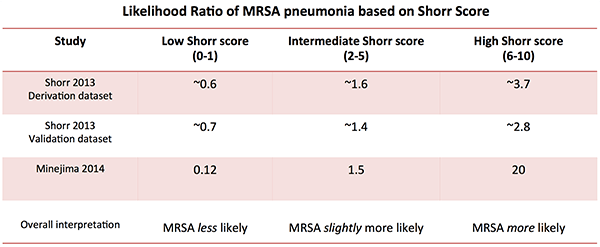
Minejima 2014 validated the Shorr score by comparing 134 patients with MRSA pneumonia vs. 134 patients with non-MRSA pneumonia at the Huntington Hospital in California (table below). The Shorr Score performed even better in this study than in the original publication (3).
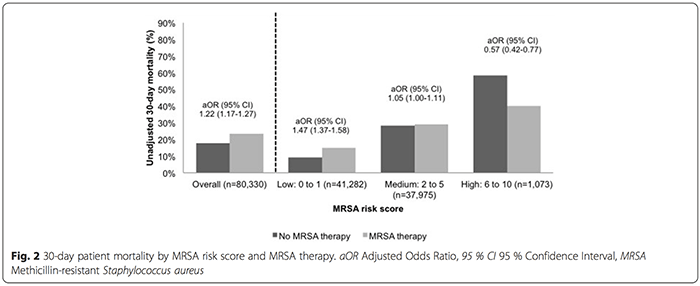
Teshome 2015 validated the Shorr score in a retrospective study involving 80,220 patients admitted with pneumonia at >150 Veterans Administration hospitals. Multivariable regression found that initial MRSA therapy was associated with lower 30-day mortality only in the high-risk group (figure below). One strength of this study is that it used a hard outcome (mortality), avoiding problems with over-diagnosis. This study suggests that the major benefit of empiric MRSA coverage occurs in patients with high Shorr scores.
 Overall, the Shorr Score is a more evidence-based approach to MRSA risk stratification than whether or not the patient has “healthcare-associated pneumonia” (HCAP). The entire concept of HCAP appears ill-conceived, because MRSA and resistant gram-negatives have distinct risk factors and different therapies (Shorr 2013). The term HCAP was introduced in 2005 pneumonia guidelines based on expert opinion rather than firm evidence. Subsequent studies haven't supported the concept of HCAP, which was just abandoned in the new 2016 ventilator-associated pneumonia guidelines (4).
Overall, the Shorr Score is a more evidence-based approach to MRSA risk stratification than whether or not the patient has “healthcare-associated pneumonia” (HCAP). The entire concept of HCAP appears ill-conceived, because MRSA and resistant gram-negatives have distinct risk factors and different therapies (Shorr 2013). The term HCAP was introduced in 2005 pneumonia guidelines based on expert opinion rather than firm evidence. Subsequent studies haven't supported the concept of HCAP, which was just abandoned in the new 2016 ventilator-associated pneumonia guidelines (4).
The Shorr Score may function similarly to the Wells Score for pulmonary embolism. As a validated risk-stratification tool, it is a good starting place for decision-making. However, clinical judgment is still required
Component #2: Nares PCR for MRSA
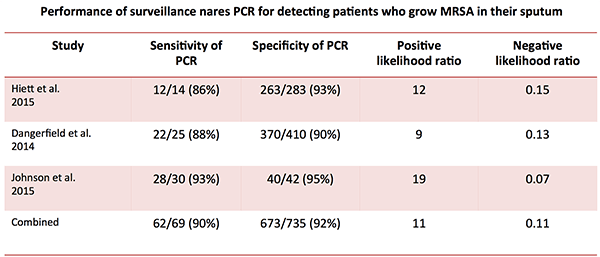
Many hospitals obtain a nares swab for MRSA PCR among all patients upon admission, in efforts to reduce nosocomial MRSA transmission. Among patients admitted with pneumonia, nares PCR has a good performance for detecting patients with MRSA in their sputum (5):
Component #3: Sputum gram stain
Sputum gram stain is occasionally helpful. Performance depends upon obtaining a quality specimen:
- Among non-intubated patients, sputum gram stain has a sensitivity for staphylococcus of ~10% (Garcia-Vazquez 2004, Anevlavis 2009)(6).
- Among intubated patients, tracheal aspirate gram stain has a sensitivity for staphylococcus of ~70% compared to sputum culture (Tetenta 2011, Seligman 2015)(7).
However, the temptation to over-interpret the gram stain must be resisted. Unless the gram stain is high quality and shows a clear predominance of a single morphology of bacteria, its significant is murky:

Component #4: Throat culture for MRSA
Several studies involving >4,000 patients show that the combination of nares plus throat culture is 5-20% more sensitive than nares culture alone for detecting MRSA colonization (8). This provides the basis for testing the throat among patients with a negative nares PCR. Jang 2014 demonstrated that the sensitivity of surveillance throat culture was superior to nares culture for predicting the development of MRSA pneumonia among patients in the ICU.
Throat culture becomes relevant among patients who are unable to produce an adequate-quality sputum sample. This is theoretically attractive for two reasons:
- MRSA usually causes pneumonia by first causing colonization of the oropharynx, then being aspirated into the lungs. Thus, patients with MRSA pneumonia would be expected to have MRSA colonization of the throat.
- Some patients with MRSA PNA may be too weak to expectorate sputum, swallowing it instead. Throat culture might be especially sensitive in these patients, who are continually trafficking MRSA through their throat.
Boyce 2013 showed that vancomycin could be safely discontinued in 91 patients at Yale with HCAP who couldn't produce sputum and had negative nasal and throat cultures. Although this hasn't been replicated, it seems like an sensible approach.
Component #5: Procalcitonin
Procalcitonin is an established tool for antibiotic de-escalation. A negative procalcitonin challenges the diagnosis of pneumonia (versus, for example, aspiration pneumonitis or atelectasis). This may be useful, because patients who receive broad-spectrum antibiotics for suspected HCAP often don't actually have pneumonia (Boyce 2013). However, a negative procalcitonin may be seen with some types of pneumonia (e.g. viral or atypical pneumonia including legionella; Haeuptle 2009).
Regardless, a patient with MRSA pneumonia really ought to have an elevated procalcitonin (unless they are neutropenic). Thus, for a patient with a negative procalcitonin, discontinuation of MRSA coverage is generally reasonable.
Component #6: Clinical judgment
No risk score or algorithm can replace clinical judgment. For example, consider a young patient with IV drug use presenting to the medicine ward with bilateral cavitary pneumonia. I would cover this patient with MRSA regardless of the Shorr score (which would be 1). Thus, clinical judgment may account for some details of patient presentation which are not captured by the Shorr score, for example:
- Radiographic appearance (e.g. multifocal, cavitary lesions would suggest MRSA). The radiologic and ultrasonographic patterns of different types of pneumonia was previously explored here.
- Prior history of MRSA
- Simultaneous skin abscess suspicious for MRSA
- Post-influenza pneumonia
Synthesis: an evidence-based approach to MRSA coverage
This is one way to combine these components into an algorithm:

(1) Decision to start antibiotics
Upon admission, antibiotics may be started based upon a combination of risk stratification and clinical judgment. When in doubt, a single dose of antibiotic for MRSA may be given pending additional information (9).
- If the Shorr score is 0-1, this argues strongly against MRSA. Unless there is some feature that is very suggestive for MRSA, MRSA coverage isn't needed.
- If the Shorr score is 2-5, then the likelihood of MRSA pneumonia is increased slightly (likelihood ratio ~1.5). However, the absolute risk of MRSA remains low (10). Ultimately this decision requires clinical judgment based on the specifics of the case and local MRSA prevalence. For example:
- Patient #1: A 65YO otherwise healthy patient with no MRSA risk factors who is admitted to ICU with a lobar pneumonia has a Shorr score of 2. This patient probably doesn't require MRSA coverage (Wunderink 2013).
- Patient #2: An 85YO woman with diabetes, dementia, recent IV antibiotics, and nursing home residence has a Shorr score of 5. This patient probably warrants temporary coverage for MRSA.
- If the Shorr score is 6-10, start empiric antibiotics for MRSA.
(2) Early re-evaluation based on nares PCR & procalcitonin
Nares PCR and procalcitonin should become available within 24 hours. These may guide early management decisions:
PCR-based initiation of antibiotics
Nares PCR may allow early detection of MRSA among patients without typical risk factors. If the nares PCR is positive, this is strongly suggestive of MRSA within the sputum (positive likelihood ratio of ~11)(11).
PCR-based discontinuation of antibiotics

If the nares PCR is negative, then this may be combined with a Shorr score <6 and clinical judgment to rule-out MRSA. The sputum gram stain should be reviewed if available. The probability of missing a patient with this rule-out can be estimated as follows:
- Probability of Shorr score <6 being falsely negative is 0.71 (Minejima 2014)
- Probability of nares PCR being falsely negative is 0.10
- Probability of sputum gram stain being unavailable or falsely negative is ~0.9 (although for an intubated patient with tracheal aspirate, this would be ~0.3).
- Probability of clinical judgment being falsely negative is ~0.9 (guessing that ~10% of patients will have “highly suspicious” presentations)
Combining this:
Frequency of missed case = (Frequency of MRSA PNA)(0.71)(0.1)(0.9)(0.9)
Frequency of missed case = 0.06 * (Frequency of MRSA PNA)
The frequency of MRSA pneumonia among all patients admitted with pneumonia may vary between ~0.5% to ~5% depending on location (12). This would yield an acceptably low missed case rate of roughly 0.03%-0.3% (1/3,333 – 1/333)(13).
(3) 48-72 hour MRSA rule-out
MRSA coverage can be stopped if either of these conditions are met:
- Negative sputum culture: The concept of discontinuing MRSA coverage on the basis of a negative high-quality sputum culture is generally accepted.
- Unable to produce high-quality sputum plus negative nares PCR plus negative pharyngeal culture: Discussed above, Component #4.
Philosophy of critical care: de-escalation
Structured de-escalation
Most pneumonia algorithms focus on initial empiric antibiotic regimens, with little thought about how these regimens might be de-escalated. Consequently, several days may go by before we start thinking about de-escalation. Patients who are unable to produce sputum may be exposed to a complete course of anti-MRSA antibiotics despite having zero evidence of MRSA.
A structured approach to de-escalation may facilitate prompt discontinuation of antibiotics. Structure promotes ordering appropriate tests immediately (e.g. procalcitonin, sputum culture). This may minimize antibiotic side-effects, especially vancomycin nephrotoxicity.
Aggressive escalation & aggressive de-escalation
 A good approach to critical care is often one of aggressive escalation followed by aggressive de-escalation (discussed here by Scott Weingart).
A good approach to critical care is often one of aggressive escalation followed by aggressive de-escalation (discussed here by Scott Weingart).
- Aggressive escalation: Initially when the patient is critically ill, treat rapidly and unapologetically with vasopressors, fluid, antibiotics, respiratory support, etc.
- Aggressive de-escalation: After the patient is improving, these therapies should be removed as soon as possible.
Aggressive escalation plus aggressive de-escalation may allow us to provide maximally aggressive care initially, while simultaneously avoiding iatrogenic harm (e.g. due to prolonged exposure to antibiotics). The algorithm above for MRSA illustrates this:
- If you're worried about MRSA in a sick pneumonia patient, don't hesitate to cover the patient (aggressive escalation).
- Once the dust settles, carefully re-evaluate and discontinue MRSA coverage as soon as possible (aggressive de-escalation).
Being comfortable with aggressive de-escalation can actually facilitate aggressive escalation. For example, imagine that once vancomycin is started, nobody feels comfortable stopping it (de-escalation failure). In this scenario, providers will be hesitant to start MRSA coverage, because starting MRSA therapy obligates the patient to receive a full course of therapy. Thus, timid de-escalation encourages timid escalation.

- Current guidelines regarding MRSA coverage are contradictory, leading to confusion. The concept of healthcare-associated pneumonia (HCAP) doesn't help matters.
- Four newer tests may help determine if patients have MRSA PNA:
- (1) The Shorr Score is a MRSA risk-stratification tool, which was empirically derived and validated.
- (2) Nares PCR is ~90% sensitive for detecting MRSA pneumonia.
- (3) Throat culture for MRSA may be used as a surrogate for sputum culture in patients who cannot expectorate.
- (4) Procalcitonin should be elevated in patients with MRSA pneumonia.
- These tests may be arranged to create an evidence-based algorithm:
Stay tuned… will have more to say about antibiotics and the new VAP guidelines soon.
Related links
- Escalation & de-escalation in critical care (EMCrit)
- Ultrasonographic patterns of CAP (PulmCrit)
- Evidence-based treatment of severe CAP (PulmCrit)
Notes
- For example, Dangerfield 2014 reported that 28% of patients with MRSA pneumonia failed to receive empiric coverage at a prominent tertiary care teaching hospital, while Minejima 2014 reported a 34% failure rate. Thus it seems that current strategies for covering MRSA pneumonia aren't working very well.
- Unfortunately, MRSA over-diagnosis is often unavoidable. For a patient with clinical pneumonia and MRSA in their sputum, the only practical way to exclude MRSA pneumonia is occasionally if the procalcitonin is negative. MRSA pneumonia could be excluded by using bronchoalveolar lavage with quantative culture and also protected bronchoscopic brushing (a special technique which avoids contamination of the sample with mucus suctioned through the working channel of the bronchoscope). Trying to perform these tests rapidly (prior to significant antibiotic exposure) is impractical and rarely done.
- The original publication by Shorr didn't include enough data to precisely calculate likelihood ratios. However, these could be estimated as follows. First, the probability of MRSA pneumonia across the entire study was 14%. The probability wasn't reported within the development and validation datasets, so it was assumed that the probability of MRSA pneumonia was probably ~14% within both groups. Second, the post-test probabilities weren't reported numerically, but could be estimated by pixel mapping of Figure 2 (the original image obtained from supplemental data). Based on these pre-test and post-test probabilities, likelihood ratios were estimated. This isn't very precise but may provide some objective fashion to compare the results from these studies.
- In the future it looks like “HCAP” and “CAP” will be merged together into a single entity of “community-onset pneumonia” or something like that (i.e. patients presenting with pneumonia or patients who manifest with pneumonia within the first 48 hours of their hospital stay). All patients with community-onset pneumonia would require risk stratification for drug-resistant pathogens (e.g. with a Shorr Score).
- Please note that this doesn't seem to work as well for patients with hospital-acquired pneumonia (HAP), or with nares-based culture
- Among all comers with pneumonia, the likelihood of sputum gram stain to make a diagnosis is low (~10%). However, if you consider only patients who are able to produce sputum, then the yield is higher (perhaps closer to 20%). The real utility of sputum gram stain & culture is the culture component, which may be useful to narrow antibiotics. The gram stain may serve as a quality-control metric to determine if the sample is of adequate quality.
- However, the sensitivity for streptococcal pneumonia may be greater, because patients with true pneumonia should have a greater concentration of staph in their sputum. For example, in the Tetenta study, 75% of the “false-negative” gram stains in this study were from samples that grew only rare or small number of staphylococcus, and probably didn't represent true pneumonia. If these samples that grew sparse staph weren't counted as “positive,” then the sensitivity increases dramatically (from 68% to 89%). This is an example about how over-diagnosis may reduce the apparent sensitivity of clinical tests.
- See studies summarized by Boyce 2013 in Table 1 of their article. Note that these are studies of simply whether the patient is colonized with MRSA, the vast majority of patients in these studies did not have pneumonia.
- Antibiotics for MRSA pneumonia (typically vancomycin or linezolid) are prescribed every 12 hours (or less frequently for vancomycin in renal dysfunction). Thus, a single dose will buy you 12 hours to obtain additional information and consider whether ongoing treatment is needed. Further information often becomes available within 12 hours (e.g. MRSA PCR, urine pneumococcal antigen, gram stain, CT scan, etc.) which may guide subsequent treatment.
- For example, in a rural population with a low rate of MRSA PNA (0.5%), an intermediate Shorr score increases the risk to only 0.75%.
- For example, with a likelihood ratio of 11, a positive nasal PCR may increase the probability of MRSA PCR from a pre-test probability of 1-5% to a post-test probability of 10-37%. Thus a positive PCR result isn't a slam-dunk diagnostic test for MRSA pneumonia, but it increases the probability to a level which warrants antibiotic coverage pending additional information.
- The reported frequency of MRSA PNA varies enormously between studies. This may relate to differences in local epidemiology, MRSA surveillance practices, and diagnostic criteria for MRSA pneumonia. Most evidence suggests that the rate of MRSA pneumonia among all patients admitted with pneumonia ranges between ~0.5% and ~5%, depending on location (Metersky 2016, Wunderink 2013). Note that this frequency describes all patients admitted with pneumonia (including both “CAP” and “HCAP”).
- Some might argue that failing to cover 0.3% of patients is an unacceptably high “miss rate.” However, empiric MRSA coverage rates in real-world scenarios are currently rather poor. For example, among patients who eventually were diagnosed with MRSA pneumonia, initial empiric coverage was adequate in only 72% and 65% in two recent studies (Dangerfield 2014, Minejima 2014). Any strategy which could improve coverage rates >95% would probably be a substantial improvement compared to current practices.
Image credits: Microscope image from wikipedia, hazmat image as well.
{kind=link}

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Awesome post as always. I’ve been reading a lot of papers by Michael Niederman who is on the board that will change the hcap guidelines for good-hopefully soon. It seems that bacteria must lose virulence genes to gain resistance, so MRSA does not have to be this terrible force which eats up the lungs as most people think is a pre-requisite.
Also studies show that when you control for comorbid conditions and functional status having “HCAP” or resistant strains does not in and of itself portend worse prognosis!
A Japanese study shows a nice algorithm for treating HCAP: http://cid.oxfordjournals.org/content/early/2013/09/01/cid.cit571
Thanks for a great post, as usual! Slightly off-topic, but your post led me to the IDSA guidelines where I was surprised to find recommendations to double-cover Pseudomonas in anyone with “risk factors” (which sounds like most of the ICU population). This certainly hasn’t been the empiric choice where I’ve trained – what is your practice?
Agree, I was surprised and a bit disappointed to see this recommendation.
My practice is not to double-cover for pseudomonas. However, please note that I work in Vermont and our rates of multi-drug resistant organisms are fairly low compared to some other areas, so this may not necessarily work if you’re practicing in a hospital with greater drug resistance.
There is little rationale for ever double-covering with a fluoroquinolone as discussed previously here: https://emcrit.org/pulmcrit/double-coverage-of-gram-negatives-with-a-fluoroquinolone/
Planning to write a full post on this topic eventually, so stay tuned.
Eagerly awaiting the post! Thanks 🙂
The proposed algorithm link no longer works – is it possible to email?
Sorry, I fixed it, should be working now.