
Introduction
This is the first of a series of four posts about vasopressors and hemodynamics. The first step is to explore the physiology of a pure alpha-1 agonist (phenylephrine).
Make no mistake, I'm not very fond of phenylephrine. I rarely use it (mostly for hypotensive atrial fibrillation). However, understanding phenylephrine is a prerequisite to understanding related vasopressors, particularly midodrine and norepinephrine.
Evidence regarding phenylephrine consists of a patchwork of often contradictory human and animal studies, based mostly on surrogate endpoints. Thus, this post is framed as an alternative viewpoint: a perspective which remains debatable.
Traditional belief #1: Norepinephrine is awesome, but phenylephrine is evil.
Alternative viewpoint: Norepinephrine and phenylephrine have more similarities than differences
 There is a misconception that norepinephrine is dramatically different from phenylephrine. However, the pharmacology of these drugs is similar. Norepinephrine is equivalent to phenylephrine plus a bit of beta-stimulation.
There is a misconception that norepinephrine is dramatically different from phenylephrine. However, the pharmacology of these drugs is similar. Norepinephrine is equivalent to phenylephrine plus a bit of beta-stimulation.
Evidence: Studies comparing phenylephrine vs. norepinephrine
Morelli 2008a randomized 32 patients with hyperdynamic sepsis to receive phenylephrine vs. norepinephrine as a first-line vasopressor (with additional open-label dobutamine as needed). The only difference detected between the groups was that patients in the norepinephrine group had a slightly higher blood pressure. There were no differences in heart rate, cardiac output, systemic vascular resistance, lactate, gastric mucosal perfusion, renal function, or dobutamine requirement:

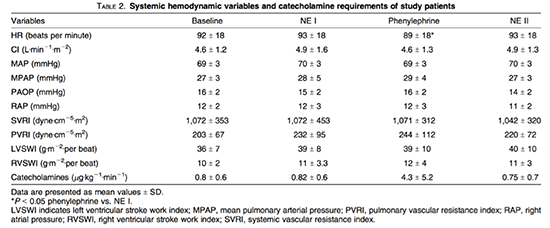
Morelli 2008b and Reinelt 1999 performed crossover studies in patients with septic shock who were transitioned from norepinephrine to phenylephrine, and then back to norepinephrine. Both studies found nearly identical hemodynamics with either drug (the only difference was a slightly lower heart rate in the phenylephrine group in Morelli 2008b, table shown below)(1).
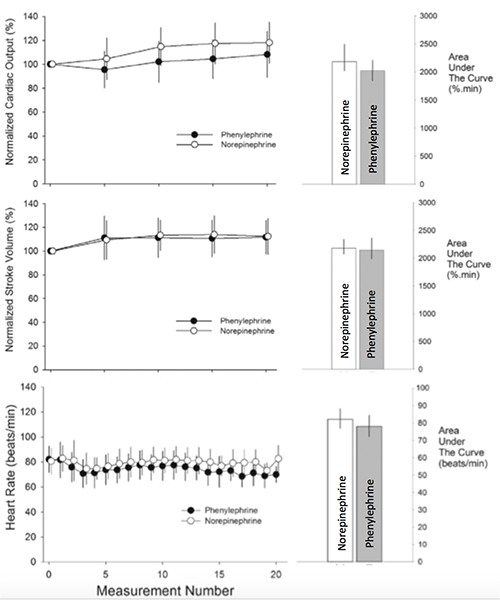
Kee 2015 performed a RCT comparing norepinephrine vs. phenylephrine during spinal anesthesia for cesarean delivery of 104 women. Phenylephrine maintained a stable cardiac output whereas norepinephrine caused a slight increase in the cardiac output (figures below). Patients on either drug had similar stroke volumes, with differences in cardiac output driven by differences in heart rate.
Poterman 2015 performed a RCT comparing norepinephrine vs. phenylephrine among sixty patients undergoing anesthesia with propofol and remifentanil. The physiologic effects of initiating either drug were indistinguishable (2):

Making sense of this data?
 Patients may have variable responsiveness to the relatively weak beta-adrenergic effects of norepinephrine. For example, responsiveness to beta-adrenergic stimulation may be lower in patients with sepsis (in whom cardiac beta-receptors may be down-regulated) or patients with a robust endogenous beta-adrenergic activity (in whom exogenous norepinephrine may have little additional effect).
Patients may have variable responsiveness to the relatively weak beta-adrenergic effects of norepinephrine. For example, responsiveness to beta-adrenergic stimulation may be lower in patients with sepsis (in whom cardiac beta-receptors may be down-regulated) or patients with a robust endogenous beta-adrenergic activity (in whom exogenous norepinephrine may have little additional effect).
Thus in some contexts, the beta-agonist activity of norepinephrine seems to have no clinical effect (e.g. Morelli 2008a, Reinelt 1999, and Poterman 2015 above). In these situations, norepinephrine and phenylephrine act in an identical fashion. Alternatively, in Kee 2015, norepinephrine did have measurable beta-agonist effects, leading to an increase in heart rate and cardiac output compared to phenylephrine.
Traditional belief #2: Phenylephrine reduces the cardiac output.
Alternative viewpoint: Phenylephrine has a variable effect on cardiac output
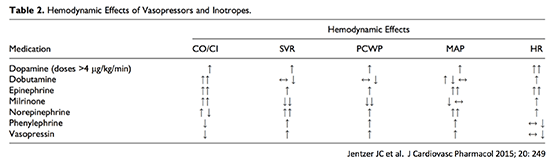
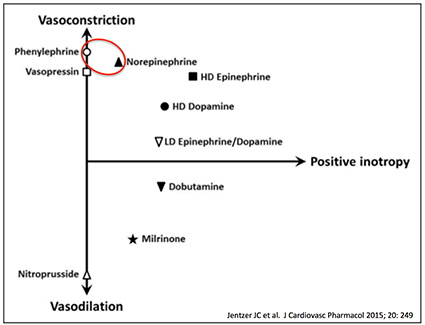
Most textbooks and review articles contain a table showing a reduction in cardiac output from phenylephrine (example above). The usual explanation is that phenylephrine increases systemic vascular resistance (afterload), which makes it harder for the heart to pump blood forward. Reality is more complicated.
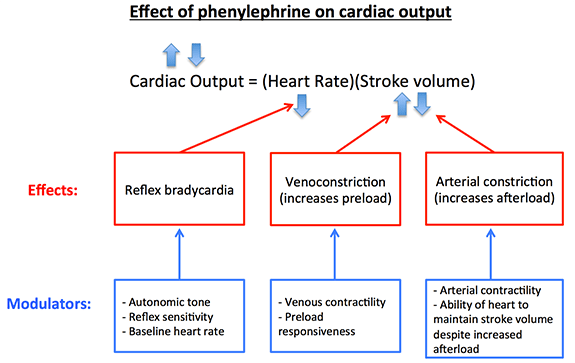
Phenylephrine can affect cardiac output in several ways:
- Reflex bradycardia: Increased blood pressure may trigger the carotid baroreflex, causing a decreased heart rate which reduces cardiac output.
- Venoconstriction: Constriction of veins increases venous return (i.e. the preload), potentially increasing cardiac output.
- Arterial constriction: Constriction of systemic arteries increases the systemic vascular resistance (i.e. the afterload), potentially reducing cardiac output.
 The effect in any specific patient may be variable, modulated by several factors:
The effect in any specific patient may be variable, modulated by several factors:
- Baseline heart rate and autonomic tone: For a patient who is severely tachycardic (e.g. atrial fibrillation), reducing the heart rate could be beneficial. Alternatively, in patients with very high endogenous adrenergic tone driving a sinus tachycardia, phenylephrine could have less effect on heart rate.
- Preload-responsiveness: Venoconstriction will serve to increase the cardiac output only in patients who are preload-responsive (i.e. fluid-responsive).
- Afterload responsiveness: Patients with systolic heart failure may respond to increased afterload with a decrease in stroke volume, whereas patients with greater cardiac reserve function may maintain their stroke volume.
Depending on the balance of these factors, phenylephrine can have any effect on cardiac output (increased, decreased, or unchanged). This was demonstrated by Yamazaki 1982, who administered phenylephrine to either patients with hyperdynamic septic shock or heart failure. Patients with heart failure experienced a decrease in cardiac output with phenylephrine (adjacent figure). These patients may not have been preload-responsive due to their cardiac disease. Thus, the increase in afterload had a dominant effect, causing their cardiac output to decrease.
Patients with hyperdynamic sepsis responded differently. These patients didn’t experience an increase in afterload at the dose of phenylephrine used, possibly due to systemic vasoplegia from sepsis. The dominant effect in these patients was an increase in preload, which caused an increase in cardiac output.

Additional studies confirm that phenylephrine usually doesn't reduce cardiac output in hyperdynamic sepsis. Flancbaum 1997 found cardiac output to be stable in septic patients despite titrating phenylephrine up to 8 ug/kg/min (table above). Gregory 1991 found that phenylephrine produced a stable/increased cardiac output, with increased stroke volume:

Traditional belief #3: Phenylephrine reduces the cardiac output by increasing afterload, leading to a reduced stroke volume.
Alternative viewpoint: Reduced heart rate might be the most common mechanism of decreased cardiac output
There are clearly situations where phenylephrine reduces the cardiac output. This has traditionally been attributed to increased afterload causing a reduction in stroke volume. Reduced stroke volume has been shown after phenylephrine boluses and in patients with heart failure (who may be unable to tolerate additional afterload, Yamazaki 1982)(3).
 However, in most studies reduced cardiac output from phenylephrine infusions occurs due to reflex bradycardia (without any reduction in stroke volume; Bellomo 2012). For example, Soeding 2013 described the effect of phenylephrine versus fluid loading in patients undergoing upright positioning for shoulder surgery. As shown here, phenylephrine caused a parallel reduction in heart rate and cardiac index, without reducing fractional shortening (a measurement of ejection fraction).
However, in most studies reduced cardiac output from phenylephrine infusions occurs due to reflex bradycardia (without any reduction in stroke volume; Bellomo 2012). For example, Soeding 2013 described the effect of phenylephrine versus fluid loading in patients undergoing upright positioning for shoulder surgery. As shown here, phenylephrine caused a parallel reduction in heart rate and cardiac index, without reducing fractional shortening (a measurement of ejection fraction).
This is usually a subtle effect that easily goes unnoticed. For example, a patient's heart rate might drop from 87 b/m to 70 b/m, causing their cardiac output to fall by 20%. A heart rate of 70 b/m isn't technically “abnormal,” so it won't draw attention. Nonetheless, this heart rate may be suboptimal for a shocked patient (“abnormally normal”).
Effects on heart rate may be a useful clinical sign, because they are easily observable without sophisticated hemodynamic monitors. An inappropriately low heart rate in a patient on phenylephrine might suggest that cardiac output is being suppressed by reflex bradycardia (4).
Studies investigating cardiac output changes associated with phenylephrine suggest that heart rate changes parallel changes in cardiac output. –Habib 2012
Pre-existing tachycardia changes this. Jain 2010 randomized septic patients refractory to high-dose dopamine to receive norepinephrine or phenylephrine. At baseline, patients had an average heart rate of 150 b/m from the dopamine. Compared to norepinephrine, phenylephrine caused a decreased heart rate, an increase in stroke volume (better diastolic filling), and no reduction in cardiac output. This supports using phenylephrine for patients with hypotension and severe tachycardia (e.g. hypotensive atrial fibrillation).
Traditional belief #4: Phenylephrine reduces renal blood flow and hurts the kidneys.
Alternative viewpoint: Phenylephrine may be beneficial to the kidneys in some situations.
Phenylephrine is widely believed to reduce renal blood flow and thereby impair renal function. However, phenylephrine doesn't vasoconstrict the renal vasculature more than other vascular beds. Thus, it is possible that the effect of phenylephrine on renal blood flow, similar to the effect on cardiac output, may be context-dependent. For example, Bellomo 2012 found that phenylephrine increased renal blood flow both in normal and septic sheep.
More importantly, it is incorrect to assume that renal function changes in parallel with renal blood flow. For example, septic patients may have shunting of blood through the kidneys, with renal failure despite increased total renal blood flow. Drugs that vasoconstrict the efferent arterioles (e.g. vasopressin) may improve renal function despite causing a reduction in renal blood flow. Therefore, instead of focusing on renal blood flow it is better to focus on changes in renal function (e.g. glomerular filtration rate, urine output).
Available evidence suggests that phenylephrine improves renal function. In healthy female volunteers, phenylephrine increased urine output and glomerular filtration rate (Klein 1995). Gregory 1991 found that phenylephrine increased urine output in patients with septic shock.
Other alpha-1 agonists (midodrine and methoxamine) seem to improve renal function. Midodrine is widely used for treatment of renal failure in the context of hepatorenal syndrome. Sun 2014 found that methoxamine increased intraoperative urine output in a prospective RCT involving patients undergoing elective hip replacement.
Norepinephrine has a good track record for defending renal perfusion. How does phenylephrine compare? Morelli 2008a and Jain 2010 found no difference in urine output in RCTs comparing phenylephrine vs. norepinephrine in septic shock.

- Norepinephrine is similar to phenylephrine (norepinephrine is equivalent to phenylephrine plus some beta-1 stimulation). In some situations the two drugs may function in an identical fashion.
- Like norepinephrine, phenylephrine can cause venoconstriction, thereby increasing venous return to the heart.
- Phenylephrine can affect cardiac output in a variety of ways:
- Increased preload may increase cardiac output
- Increased afterload and reflex bradycardia may reduce cardiac output.
- The effect of phenylephrine on cardiac output varies depending on the clinical context.
- The most common mechanism whereby phenylephrine reduces cardiac output may be reflex bradycardia. Thus, an inappropriately low heart rate in a shocked patient on phenylephrine suggests that cardiac output is being suppressed.
- Available evidence suggests that phenylephrine can improve renal function, particularly in hyperdynamic shock states (e.g. cirrhosis, sepsis).
Stay tuned for three additional posts on hemodynamics.
Related topics
- Vasopressor basics (EMCrit)
- The crashing atrial fibrillation patient (EMCrit)
- Decompensation of atrial flutter following cardioversion (PulmCrit)
- Collapsed IVC doesn't equal hypovolemia (PulmCrit)
- Early initiation of norepinephrine in septic shock (PulmCrit)
- Vasopressin and renal microvascular hemodynamics (PulmCrit)
Notes
- Morelli 2008b found a reduced GFR in the phenylephrine group, but this remained low after transitioning back to norepinephrine. Thus, it is not possible to conclude that the low GFR was caused by phenylephrine, it may have simply represented the evolution of septic shock over time. Phenylephrine did reduce the hepatic perfusion compared to norepinephrine, but it is unclear exactly what the hepatic perfusion ideally should be, and whether reduced hepatic perfusion could be a beneficial or detrimental effect.
- The cardiac output data from this study was based on pulse contour analysis using a noninvasive monitoring device (Nexfin), whose validity is unclear. However, reported heart rates should be accurate.
- The physiologic effect of a phenylephrine bolus is not necessarily the same as a phenylephrine infusion. For example, Cannesson 2012 found in pigs that when volume loaded (and preload-independent), a phenylephrine bolus reduced cardiac output. However, in this same setting a phenylephrine infusion had a positive/neutral effect on cardiac output. The response to a phenylephrine bolus represents the body's initial response, but may not represent the new equilibrium state that is eventually reached when ongoing phenylephrine exposure occurs in the form of an infusion. This post is focused on phenylephrine infusions. In general it seems that the response to phenylephrine boluses is less favorable than infusions. It is possible that studies of phenylephrine boluses may have contributed to phenylephrine's bad reputation.
- On a more practical and less arcane level, a shocked patient with a sluggish heart rate who is perfusing poorly could probably benefit from a faster heart rate, regardless of the exact etiology of the heart rate (i.e. phenylephrine, beta-blocker, sinus node disease, etc.). We spend lots of time thinking about inotropy, but chronotropy may also be important. For example, if you double someone's heart rate from 40 b/m to 80 b/m with a stable stroke volume, their cardiac output will double. Meanwhile, it is impossible to double someone's cardiac output by increasing their ejection fraction from 55% to 110%.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Awesome review, really helpful discussion. Any comments on the concept of tachyphylaxis that is reported to occur with phenylepherine,?
Thanks
Casey
Short answer: I don’t know.
Long answer: I’m not aware of evidence about this. The sensitivity to alpha-adrenergic stimulation may fluctuate during the course of illness (especially sepsis), and there are publications regarding the phenomenon of refractory vasodilation/vasoplegia. I’m not aware that this is a specific problem with phenylephrine (e.g. moreso than norepinephrine).
Thanks, Josh
Thanks so much – fantastic job of separating out the nuances of context and effect. Its like an old record player – we’re dealing with both volume and tone. This dovetails very well into Weingart’s questions about fluid responsiveness: Can the RV take it, and can the LV use it? I like that your analysis takes us back to considering the fundamental pathophysiology that is out of order; is volume down? Is vascular tone down? Are catecholamines upregulated? By knowing whats low and what’s high, we can have more informed expectation for how alpha stimulation will affect the clinical picture.… Read more »
Josh,
You are the MAN! I don’t know how you find the time to organize such information and well constructed blog posts! Thank you for this resource!
Do you have any comments on the safety of peripheral IV admin of PE vs NE?
Thanks,
Zammit
Thanks! I think either phenylephrine or norepinephrine can cause trouble if they extravasate. My usual approach is to choose the best drug for the patient, and obtain central access as soon as possible. For more on peripheral vasopressors would see Scott Weingart’s podcast https://emcrit.org/podcasts/peripheral-vasopressors-extravasation/
Wow I’m surprised to see that epinephrine has more ionotropic effects than dobutamine and milrinone (if I’m reading the graph correct)! Apparently prolonged catechoaminergic stimulation is not good which is probably why beta-blockers like esmolol drips are beneficial (larger trial pending to evaluate this). Maybe another reason why an agent with less beta activity is preferred. We might be seeing a pendulum shift in our use of pressors!
Yes, low-dose epinephrine functions primarily as an inotrophe. Epinephrine is actually my inotrophe of choice, especially in septic shock (more on this to follow).
The beta-blocker stuff is very interesting. I’m waiting for more evidence before I reach a conclusion on this.
It is interesting that phenylephrine can result in reflex bradycardia. The assumption is that phenylephrine is used when a patient is hypotensive to start off with, during which the baroreceptors would be inactive. Phenylephrine would help bring the MAP closer to normal and should not (at least theoretically), trigger a reflex bradycardia. I’m wondering if the drop in HR actually reflects a reduction in the endogenous catecholamines (which have chronotropic properties) and that this reduction is the one that results in the mild reduction in HR.
Excellent point. One problem with many hemodynamic interventions is that it is difficult to account for the endogenous catecholamine response, and how it may change in response to our interventions.
Don’t know if your future posts will cover this, but where would you place Isoproterenol on that chart? Equal with dobutamine? The doc’s in my ED like using isoproterenol, but considering it also has beta-2 properties, may not be the best option due to the risk of hypotension. Additionally, now that it’s so expensive, if it was equal with dobutamine, should I be recommending (as the pharmacist), to use dobutamine over isoproterenol? Looking forward to the rest of the hemodynamic posts
Isoproterenol is probably slightly south of dobutamine. Dobutamine has some alpha-agonist activity whereas isoproterenol doesn’t have any, thus isoproterenol might be a touch more vasodilating than dobutamine. Isoproterenol probably isn’t a great drug unless the patient has hypotension driven by bradycardia, in which case the positive chronotropic effects may dominate any vasodilating effects. I rarely use isoproterenol, but it does have the advantage that it doesn’t cause vasoconstriction therefore it is particularly safe to give peripherally. This may occasionally be helpful in a patient with symptomatic bradycardia where you’re trying to avoid placing a central line. More about that here:… Read more »
Regularly use phenylephrine peripherally in anaesthesia and critical care 100-200 mcg/ml to treat vasodilation. Rarely causes problems in terms of extravasation and tissue injury based on our experience. We frequently use it while preparing, getting cvc in and confirming position etc in patients with sepsis then switch over to Norad. Everywhere I have worked in UK phenylephrine is considered suitable for peripheral administration and Norad not. Even with evidence suggesting Norad may be ok with big proximal cannula short term I am not sure we are in a hurry to change locally. We will happily administer phenylephrine through a 20g… Read more »
I would love to see the evidence that says phenylephrine is safe peripherally wheras noradrenaline is not, because in Paul Mayo’s ICU all pressors are safely given through peripherals (except vasopressin as there is no reversal agent) with the understanding that extravasation of any of them has to be treated immediately.
Phenyl is FDA improved for IM/SubCut injection
For more on peripheral vasopressors would look here: https://emcrit.org/podcasts/peripheral-vasopressors-extravasation/
In the uk meteraminol is often the push dose pressors of choice and is often used as a peripheral continuous infusion. As a pure alpha 1 agonist can I generalise the assumptions around the effects of phenylephrine to meteraminol?
I don’t know anything about meteraminol, but you probably could. It seems like midodrine, methoxamine, and phenylephrine (other alpha-1 agonists) act similarly. I don’t know why meteraminol wouldn’t as well.
Typo – under Summary Bullets. Second bullet “norephrine”. Thought there was yet another pressor I had to learn about!
Thanks! I have a special ability to read a draft ten times and still miss basic spelling errors.
Great information! I teach hemodynamics at my facility, and appreciate your attention to the possible benefits of using neo rather than levo for more than “hypotensive with afib rvr.” That said, my primary sticking point with neosynephrine is the volume. Most of our patients are receiving IVF, epi, stacks of antibiotics, etc. and one of the benefits of levo is that I can obtain it in quad-strength form. Neo I can’t. The most our pharmacy will do (after I spend a minimum of three phone calls to the on-duty and one to the director) is make the drip 10mg/250cc. It’s… Read more »
Hilarious but true.
Sometimes folks on the ICU team want to give patients “maintenance fluids.” Aside from being a bad idea in general, it is always important to realize how much fluids the patient is getting simply from infusion and medications… so patients are effectively getting ongoing fluid whether or not we like it.
Along this vein, it would be nice if antibiotics could be available in two formulations:
(1) dilute form dissolved in lots of fluid for peripheral administration
(2) concentrated form dissolved in 10-20 ml for central administration
That is an excellent idea. How about this one: protonix can be given IVP for a total of 10ccs. But many places mix it in a 100cc bag, with one excuse or another for the admixture. Calcium is the same way. Zosyn 2.25 can be given in 50ccs no problem yet often I find it in 100cc bags. Cardene? If you work at a facility that springs for the premix you can get it in 40mg/200cc, but if your pharmacy insists upon gaining the bill for admixture (as mine do) you get the typical 20/200, which means your fresh heart… Read more »
Any studies that show phenylephrine safe in peripheral lines
i am so much enjoying your hemodynamics posts! hoping for more to come!
Dr. Farkas, You make some nice alternative views in this article, however I would like to take serious issue with one of your points if I may. Namely, Traditional belief #4: Phenylephrine reduces renal blood flow and hurts the kidneys. Alternative viewpoint: Phenylephrine may be beneficial to the kidneys in some situations. Now, granted Phenylephrine has been shown to be of benefit in septic shock, and in that particular setting since the patient is very vasodilated already, the net effect of the Phenylephrine on the renal beds may not result in vasoconstriction. That setting aside, I can assure you that… Read more »
I have extensively utilized Neo in critical care settings and my experience has been positive overall. I’m fond of using it, especially when it’s undesirable to have excessive tachycardia, or the patient is tachycardic from either a side effect from another pressor or from endogenous compensation. Like NTG, Neo performs exactly as expected and demonstrates predictive qualities. Thumbs up from me!