 Introduction with a case of failure
Introduction with a case of failure

A 50-year-old man is transferred from an outside hospital after being intubated for pneumonia. He had been receiving maintence fluid for the past week and is now grossly edematous. Aggressive diuresis is desired to help wean him from the ventilator.
For two days he is diuresed with furosemide, during which time he has a net fluid balance of negative four liters. However, it is subsequently noticed that he is hypernatremic with a sodium of 150 mEq/L. His calculated free water deficit is 3.5 liters. This is repleted over the next two days.
Ultimately, over the first four days of his ICU course his fluid balance ends up being net even (he was diuresed initially, and then received free water). Efforts to diurese him failed. He continued to require the same amount of ventilator support. Why?
Groundwork: Defining terminology & understanding goals of diuresis
Defining dehydration & understanding why it is evil
Although the term dehydration is often used loosely, the medical definition of dehydration is loss of free water resulting in hypernatremia (1). This is common in the ICU, usually from failure to replace daily water losses. Normally, hypernatremia triggers thirst and water intake, but this is impossible among intubated patients.
Hypernatremia should generally be aggressively corrected. Hypernatremia may make patients miserable, manifesting as “agitation” and leading to increased sedative administration (imagine being thirstier than you've ever been in your life yet unable to drink). I've seen some patients with significant agitation on the ventilator which persisted until we fixed their hypernatremia:

To make matters even worse, dehydration does little to improve tissue edema (which is due to excessive extracellular fluid volume). For example, imagine removing one liter of free water from a patient. Since water diffuses freely between the intracellular and extracellular spaces, water will be removed from both spaces. With an equal rise in osmolarity throughout the body, the amount of water loss from each space will be proportionate to its volume. Therefore, since the intracellular volume is about twice the size of the extracellular volume, removing a liter of free water will only remove one third of a liter from the extracellular space.
Electrolytic goals of diuresis
Generally we diurese patients with a goal of removing extracellular volume. Ideally this is achieved by net removal of fluid with an identical electrolyte composition compared to plasma. This is desirable for two reasons:
- Removal of isotonic fluid prevents any change in sodium or osmolarity. This avoids movement of water out of the intracellular volume. Thus, removed fluid is purely drawn out of the extracellular volume.
- Removal of fluid with an electrolyte composition equal to plasma would avoid causing electrolyte derangements (e.g., hypokalemia).
It is generally impossible to achieve this purely via diuresis, because the electrolyte composition of urine is rarely exactly equal to the serum electrolytes. Fortunately, all that is required is that there is a net removal of fluid with an electrolyte composition matching plasma. For example, if excess potassium is excreted in the urine, this may be corrected by increasing potassium intake to achieve a net loss of potassium which is proportional to losses of sodium and water (2).
Nonetheless, when we are diuresing a patient with a goal of volume removal, a sensible goal is for the urine electrolyte composition to be relatively close to the serum electrolyte composition. The greater the differences between urine and serum electrolytes, the more work we will have to do to compensate for these differences (e.g. with exogenous electrolyte or water replacement).
Physiology of occult diuretic resistance
The traditional approach to volume removal in the ICU is furosemide. However, this sometimes fails due to a combination of factors:
- The stress of critical illness often causes patient's kidneys to avidly retain sodium. In this context, furosemide may stimulate production of a dilute urine with little sodium in it.
- Critically ill patients have a significant sodium intake even if they are sodium-restricted (e.g. with various medications and drips formulated in normal saline).
- Critically ill patients usually lack ad libitum access to water as needed to satisfy their thirst (e.g. due to intubation). This may allow them to develop significant dehydration and hypernatremia, before it is recognized and corrected.
The combination of these factors may produce the following situation during diuresis:
- Even sodium balance: The patient is excreting relatively little sodium in the urine, while continuing to have a significant sodium intake with medications.
- Negative water balance: The patient is excreting liters of dilute urine, with relatively little water intake.
- Negative volume balance: This makes it seem like the patient is being effectively diuresed.
The ultimate effect of diuresis, then, is merely loss of free water (dehydration and hypernatremia). As discussed above, dehydration is evil and requires correction. After correcting the hypernatremia with administration of water, the patient is returned back to their original condition (with no change in volume status at all).
“Occult diuretic resistance” may be used to describe this phenomenon, when attempts to diurese a patient merely cause dehydration (as opposed to overt diuretic resistance, when a patient doesn't urinate). Occult diuretic resistance is frustrating because initially it seems like the patient is responding to therapy, with a gratifying increase in urine output. Apte 2008 documented an example of this phenomenon among ten patients (3).
The above description (diuresis resulting in zero sodium loss, with purely loss of water) is the most extreme form of occult diuretic resistance. A more common scenario may be a patient with some net sodium loss as well as a large net free water loss. In this latter case, after replacing the free water loss, there is still some net volume loss.
Management strategies for occult diuretic resistance
Traditional approach: Give furosemide and replace free water losses
The traditional approach to the emergence of hypernatremia during diuresis is to replace the free water losses (e.g. with enteral water or intravenous D5W). Meanwhile, diuresis may be continued. If the urine isn't too dilute, this strategy may work. However, this approach is often challenging. Large volumes of supplemental water may be needed. If enteral water cannot be given, then infusion of D5W may cause hyperglycemia. The ultimate amount of volume lost is often disappointingly low.
Better approach: addition of thiazide to enhance natriuresis
Furosemide blocks sodium reabsorption by the descending loop of Henle. The physiologic problem that drives occult diuretic resistance is avid sodium retention by the remainder of the nephron (especially the distal convoluted tubule). Addition of a thiazide diuretic blocks this, preventing sodium absorption in the distal convoluted tubule and thereby increasing urinary sodium excretion (natriuresis). This promotes balanced excretion of both sodium and water, causing effective volume loss without hypernatremia.
The ability of a thiazide to increase urine sodium concentrations when added to a loop diuretic has been shown in numerous studies dating back to the 1970s. Thus, there is a robust scientific rationale for combining a loop diuretic and thiazide to promote natriuresis. However, there hasn't been much clinical evidence about this among critically ill patients… until recently…
Bihari 2016: Prospective RCT of furosemide + thiazide diuresis in the ICU
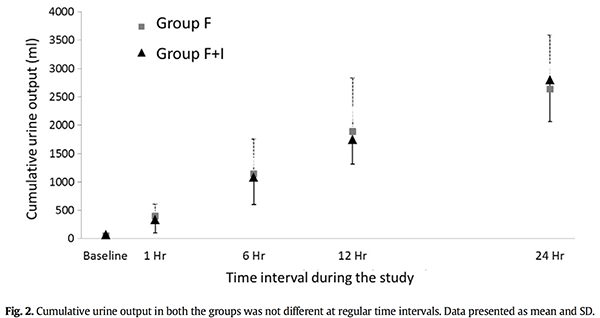
This is a prospective RCT comparing diuresis with furosemide vs. furosemide plus indapamide (a thiazide diuretic) among forty fluid overloaded ICU patients. Patients were randomized to receive the following therapy and followed for 24 hours:
- Furosemide group: 1 mg/kg IV furosemide (up to 60 mg) IV
- Indapamide group: 1 mg/kg IV furosemide (up to 60 mg) IV plus enteral indapamide 5 mg
The volume of urine output was identical between the two groups (figure below). This is surprising given that, among patients with chronic CHF, the addition of a thiazide to furosemide increases urine output. This difference could reflect chronic compensatory changes in the distal convoluted tubule in patients with CHF exposed to furosemide chronically (in contrast, this study included only patients who were not on chronic diuretics).
The authors meticulously analyzed urine as well as fluid and sodium intake from medications, intravenous fluids, and nutrition (table below). Key findings were:
- Patients in the furosemide group had a median sodium balance of only -20 mEq, with a median fluid balance of -691 ml. Thus, these patients didn't lose much sodium, but instead primarily lost free water (occult diuretic resistance).
- Patients in the indapamide group had a medium sodium balance of -100 mEq, with a median fluid balance of -770 ml. This calculates to a sodium concentration of 142 mEq/L among the net fluid lost by these patients. Thus, when taking into account all sources of input and excretion, these patients lost a nearly isotonic balance of sodium and water (4).

The effect on serum electrolytes was consistent with these calculations. Patients in the furosemide group had an average increase in their serum sodium concentration by 2 mEq/L, consistent with removal of ~700 ml free water (dehydration). Alternatively, patients in the indapamide group had no change in their average serum sodium concentration, consistent with net excretion of isotonic fluid.
Effect on tissue edema
Patients underwent blinded scoring for the amount of tissue edema at several locations (pedal, lateral chest wall, hand, and sacrum) to yield an edema score ranging from 0-16. Despite both groups having the same fluid balance, patients in the furosemide group had no significant change in their edema scores, whereas patients in the indapamide group did (decrease from average 8.1 to 4.8, p<0.01).
This is consistent with electrolyte changes. Furosemide led to dehydration, which is ineffective for treating edema because it mostly causes loss of intracellular volume (as discussed earlier). In contrast, patients in the indapamide group lost isotonic fluid, which exclusively drains volume from the extracellular space.
Drawbacks of dual diuretic therapy
The main drawback of combined diuresis with indapamide was greater potassium loss (median of 102 mEq/day vs. 56 mEq/day with furosemide alone). This comes as no surprise, given that combined diuretic therapy is quite effective as treatment for hyperkalemia. Nonetheless, this must be anticipated and repleted. There was no difference in magnesium loss between the two groups.
Could indapamide have renoprotective properties?
Indapamide is technically a “thiazide-like diuretic,” meaning that it blocks the distal sodium-chloride channel, but is chemically dissimilar from classic thiazide diuretics. Indapamide has some unique properties including anti-oxidant, vasodilatory, and anti-inflammatory effects on the kidney (Ma 2013, Uehara 1993). These could theoretically exert a renoprotective effect.
 Madkour 1996 found that in a prospective RCT, indapamide improved renal function compared to hydrochlorothiazide (adjacent figure). Bihari 2016 found that the addition of indapamide to furosemide caused a substantial increase in creatinine clearance (table 2 above). However, the GFR range reported in the indapamide group was supraphysiologic (interquartile range 175-326 ml/min), making this result almost too good to be true.
Madkour 1996 found that in a prospective RCT, indapamide improved renal function compared to hydrochlorothiazide (adjacent figure). Bihari 2016 found that the addition of indapamide to furosemide caused a substantial increase in creatinine clearance (table 2 above). However, the GFR range reported in the indapamide group was supraphysiologic (interquartile range 175-326 ml/min), making this result almost too good to be true.
Further evidence is needed. In the interim, indapamide remains a solid diuretic choice supported by a significant volume of clinical evidence (Waeber 2012).
The future: Triple diuretic therapy?
It's possible that the ideal diuretic therapy would be a combination of furosemide, a thiazide, and spironolactone (Jermyn 2013). Spironolactone could reduce potassium secretion, counteracting the potassium-wasting effects of furosemide and a thiazide. Spironolactone could also promote the excretion of bicarbonate, which would counteract the effects of furosemide and thiazide (which may cause metabolic alkalosis). Overall it is possible that gentle, balanced inhibition of the nephron at three sites might be physiologically superior to intense inhibition of a single site.
P.S.- Quadruple diuretic therapy!
After posting this, Dr. Olusanya directed me to Morris 2011, which describes a four-agent diuretic regimen including furosemide, acetazolamide, spironolactone, and aminophylline. The authors report routine use of this regimen with success, including achievement of urine with “composition extremely close to that of plasma.” This is a great example of whole-nephron diuresis with several agents that balance each other out (e.g. acetazolamide and spironolactone cause acidosis whereas furosemide causes alkalosis).

- Critically ill patients often avidly retain sodium. This may cause diuresis attempts to fail, if patients excrete dilute urine leading to a loss of water without loss of sodium. Such patients may seem to respond to diuresis, but in fact they are merely becoming progressively dehydrated and hypernatremic (occult diuresis resistance).
- Combining a loop diuretic and thiazide diuretic is proven to increase sodium excretion in the urine (natriuresis). A recent RCT confirms that this combination promotes balanced loss of sodium and water, allowing volume removal without dehydration.
Related electrolytic madness
- Deresuscitation is covered in this brilliant lecture by the late Dr. John Hinds. The approach to deresuscitation described here involving IV hydrochloric acid and IV water sounds extremely effective. However, this requires buy-in from pharmacy and the ICU group. I would be interested to hear if anyone in the US is doing this.
- Multi-site nephron blockade for treatment of hyperkalemia
- Hyponatremia treatment: Taking control with DDAVP
- pH-guided fluid selection
Notes
- This must be distinguished from volume depletion, which is a balanced loss of water and salt (resulting in hypovolemia with a normal serum sodium concentration).
- Generally potassium replacement is undertaken by measuring the serum potassium and titrating potassium intake accordingly. However, theoretically an equally valid approach would be to measure the concentration of potassium in excreted urine and use this to calculate the required potassium replacement. Calculating potassium losses from the urine could reduce the amount of phlebotomy that the patient was subjected to (e.g. instead of checking chemistries Q12hr during diuresis, they could be measured Q24 hours with monitoring of urine electrolytes in the interim).
- Apte 2008 described 10 intubated patients who were diuresed with furosemide for two days. The average urine output over 48 hours was 3.16 liters. However, taking other sources of fluid input into account, the average fluid balance over this time period was -760 ml. Meanwhile, the serum sodium increased by an average of 3 mEq/L. For an average-sized patient, an increase in sodium by 3 mEq/L equates to a free water deficit of roughly 750-900 ml. Therefore, on averge the net volume loss matches up closely with the free water deficit, implying that these patients mostly underwent dehydration.
- Please note that the urine these patients excreted was not isotonic, but rather it was still hypotonic (with a median sodium concentration of ~74 mEq/L). However, taking into other factors (e.g. 1.5 liters fluid intake daily), the net result was a loss of isotonic fluid.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Dear Josh, Good post, thank you for sharing your thoughts. I might add that mineralocorticoid receptor blockers – such as spironolactone – are not only diuretics, but have potent anti-fibrotic and reverse-remodeling effects (especially in the myocardium). These effects are considered to be the mechanism behind the mortality benefit seen in heart failure and MI patients. (MJ Young – Current opinion in nephrology and hypertension, 2008) Unfortunately the onset of of action of spironolactone is quite slow. It usually requires a few days to have a clinicaly significant effect (Lowder et al. NEJM 1974; Colussi et al. J Hypertens 2013;… Read more »
Excellent point about spironolactone. This probably explains the lack of benefit from acute spironolactone use described in a small study by Apte Y and Bellomo R et al (Crit Care & Resuscitation 10:306 2008). So perhaps if you want more rapid action regarding potassium retention and management of alkalosis you could use triamterene or amiloride. Alternatively, one could start spironolactone early, in anticipation of future hypokalemia and alkalosis.
I’ve personally found the majority of ICU patients don’t become hypernatremic when they get to the point of starting diuresis, but when it does happen, I’ve always struggled trying to decide what to do about their volume status. I definitely will try adding on thiazides in the future. Great article, thanks!
Agree, not all patients develop hypernatremia. My impression is that the patients who are sicker and under more stress are more sodium-avid, and thus more likely to develop hypernatremia.
Josh
Very interesting article. Thanks for the references. I’m excited to try it. Do you think it would work with other thiazides, understanding the loss of the “renal protective” effect of indapamide by using others?
Joe
Yes, I think that any thiazide or thiazide-like diuretic should facilitate natriuresis (this is a class effect due to blockade of the Na/Cl channel in the distal tubule).
I’m looking forward to quintuple diuretic therapy with Diamox as well
Or sextuple diuresis with acetazolamide, furosemide, aminophylline, indapamide, spironolactone, and amiloride. Would extract fluid from a stone.
That is a very interesting study regarding the lasix vs lasix/indapamide. With currently available thiazide diuretics only being available in PO formulations, this study seems to suggest enteral thiazides are still working. The traditional teaching it seems is that diuretics in fluid overload states are more effective IV as there is GI edema which decreases PO absorption.
Do you have any thoughts about lasix vs bumex IV diuresis? I’ve preferred to use Bumex in my hypoalbuminemic patients (which ends up being most of my patients – amazed at being morbidly obese but still malnourished)
Was in the shower and had a thought (which is of course where all good ideas originate)
If we go with the assumption that we have these hypernatremic patients with diuretic resistance, who due to their critical illness are retaining sodium > water, would there be any role for an ACE-I in combination with the loop diuretics? Or possibly in combination with this loop/thiazide combination that was discussed. Block aldosterone -> less Na absorption -> increased naturesis, plus more K+ retention so less hypokalemia.
Just a thought…
Dear Paul,
Interessting thought. ACEi are known to improve sodium excretion in heart failure patients (Hypertension. 1997 Aug;30(2 Pt 1):168-76.), although I don’t think a critical ill patient necessarely has the same physiology. More so, in hemodynamic unstable patients I don’t think we would like to start with an ACE because 1) you impair vasomotor response systemically and 2) especially impair the auto-regulatory response to hypotension in the kidney. That significantly increases the risk for renal failure (Rose BD, Post TW. Clinical Physiology of Acid-Base and Electrolyte Disorders, 5th ed, McGraw-Hill, New York 2001; J Hum Hypertens. 2003;17(6):419.)
Great thought, but I think the increased risk of renal failure would make ACEi an undesirable agent. Diuresis is largely a game of chicken with the kidney: how much fluid can you remove without causing renal failure? During active diuresis it may be helpful to avoid any potentially nephrotoxic meds (e.g. ACEi/ARB, NSAIDs, etc.). I have mixed feelings about ACEi/ARB in the ICU in general. These are good drugs for patients with heart failure, especially patients with a tendency to slide into flash pulmonary edema due to elevated afterload. Captopril is sometimes convenient because of its fast onset. However, for… Read more »
Is that effect of Indapamide on creatinine clearance a ‘reverse causation’? Patients with AKI might not have been considered for adding Indapamide.
Dear Josh,
This is one of the best overviews of diuretics and fluid physiology that I have seen. I do have one question for you, however: what are your thoughts on ADH secretion with respect to diuretic use?
As we know, effective circulating volume depletion induced by diuretics is a potent stimulus for ADH release. This in turn causes the kidneys to retain electrolyte-free water (which is why some patients treated with frusemide develop hyponatraemia). How would you try and design a diuretic regimen to circumvent this physiologic response?
Best wishes,
Dilu Perera
Physician Trainee (Melbourne, Australia)
Hey Josh, thanks for the article! I was wondering: if you start off diuresing a patient with Lasix and end up hypernatremic, adding Thiazide (HCTZ or Diuril) will not fix the hypernatremia, will it? (since pt will be urinating isotonic fluid which should not change the serum sodium levels, correct?) In such a case, would the best approach be to add Thiazide to Lasix and simultaneously give the patient free water to correct the hypernatremia as one continues to diurese?
this article is awesome!