
UPDATE:
- ⚠️ The MIDAS trial suggests that midodrine is not beneficial for accelerated weaning off IV vasopressors (more on the MIDAS trial here).
- Currently, best available evidence indicates that midodrine should not be used to accelerate weaning off vasopressor infusions among non-cirrhotic patients.
- Midodrine may remain useful in patients with cirrhosis and hepatorenal syndrome.
Introduction with a clinical conundrum
An elderly woman is admitted to the ICU with urosepsis. By ICU day #3 she is dramatically improved, but having difficulty weaning off vasopressors. At this point, she has been requiring between 2-4 ug/min of norepinephrine for one day. Whenever the norepinephrine is stopped, her MAP falls into the mid-50s. What is the best approach to this?
- [a] Bolus her with fluid and attempt to wean off norepinephrine.
- [b] Perform bedside ultrasonography and give fluid if the IVC has lots of respiratory variability, then try to wean off norepinephrine.
- [c] Stop norepinephrine and see if she can continue to produce urine despite hypotension.
- [d] Continue norepinephrine infusion.
Until recently, these were the usual approaches to this situation. However, none of them is perfect:
Choice A: Fluid challenge This may be the worst approach. By the time someone has been in a North American ICU for three days with urosepsis, it is essentially impossible that they will be volume depleted.
Choice B: Ultrasound-guided resuscitation Also not a great approach. Ultrasound-guided fluid resuscitation may be helpful during the initial resuscitation, but not on ICU day #3. By this point, she has already received lots of fluid. Therefore, two possibilities exist:
- Ultrasound shows that she is intravascularly fluid replete. In this case, fluid is not indicated.
- Ultrasound shows that she is intravascularly fluid depleted. However, we know that she has already received a lot of fluid during her hospital course. Therefore, if she remains intravascularly depleted, this means that the fluid given to her has leaked out of her capillaries. Thus, she still won't benefit from additional fluid. Additional fluid will work great for a few hours, but then it too will leak out of her vasculature.
Choice C: Wean vasopressors for urine output This isn't a bad approach, but it's not perfect either. Even if the kidneys continue to produce urine, there is still a possibility that they could become injured due to hypotension. Furthermore, regardless of her kidneys, if she remains hypotensive this may inhibit physical therapy and transfer to the ward.
Choice D: Continue norepinephrine: This was previously my usual approach. There are some patients who develop persistent vasodilation (a.k.a., “vasoplegia”), which takes a few days to resolve. With patience, this will resolve. Sometimes the safest approach is to wait it out.
Newer approach to weaning vasopressors: Oral midodrine
Midodrine is an oral agent which functions as an alpha-1 agonist. It has been used in a variety of situations including autonomic dysfunction, hepatorenal syndrome, and dialysis-induced hypotension. Over the past few years there has been increasing interest in using midodrine to facilitate weaning off vasopressors.
Evidence
Sharma 2008
Carotid artery stenting often causes several hours of hypotension due to vagal stimulation, requiring intravenous vasopressors in an ICU. This is a case series of four patients who were treated with oral midodrine in a telemetry unit, to prevent the requirement for receiving intravenous vasopressor therapy. All patients were treated with midodrine 10 mg q8hr for 24 hours, with excellent results and no complications.
Liu 2010 (abstract)
This was a retrospective descriptive study comparing 20 patients with shock who were weaned from IV vasopressors using midodrine versus 20 patients weaned without midodrine. The average duration of intravenous vasopressor use was 0.3 days shorter in patients receiving midodrine (p=0.049).
Levine 2013
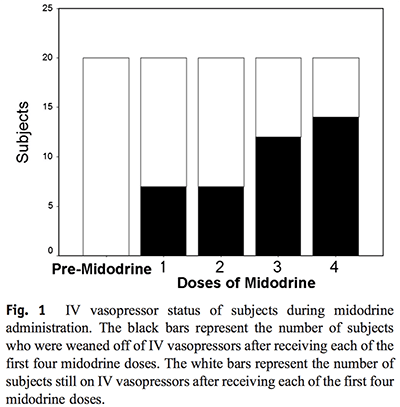 This was a prospective observation study of midodrine use in the surgical ICU at Massachusetts General Hospital. Twenty patients were treated after they had improved and met ICU discharge criteria, aside from requiring low doses of vasopressors (either <150 ug/min phenylephrine or <8 ug/min norepinephrine). Reasons for vasopressor requirement were diverse (including neurogenic shock, medication effect, and systemic inflammation).
This was a prospective observation study of midodrine use in the surgical ICU at Massachusetts General Hospital. Twenty patients were treated after they had improved and met ICU discharge criteria, aside from requiring low doses of vasopressors (either <150 ug/min phenylephrine or <8 ug/min norepinephrine). Reasons for vasopressor requirement were diverse (including neurogenic shock, medication effect, and systemic inflammation).
Midodrine was successful in allowing discontinuation of intravenous vasopressors within 24 hours in 70% patients. The rate of weaning off vasopressors was significantly faster after starting midodrine, suggesting that this wasn't merely coincidental. Hemodynamics remained stable throughout the transition. The median duration of midodrine use during the entire hospitalization was four days, with a range of 3-7 days. No complications were noted.
Whitson 2016
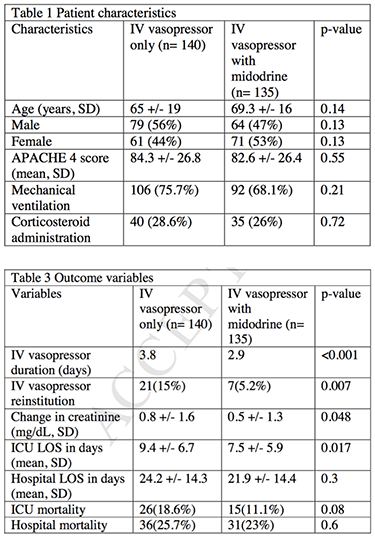 This was a retrospective observational study of patients weaned from vasopressors using midodrine following the resolution of septic shock. 140 patients weaned using midodrine were compared to 135 patients weaned without midodrine. Prior to starting midodrine, the average vasopressor requirement was either 0.09 +/- 0.09 mcg/kg/min norepinephrine or 1.05 +/- 0.77 mcg/kg/min phenylephrine. Although the study wasn't randomized, the two groups were fairly well matched (Table 1 on right).
This was a retrospective observational study of patients weaned from vasopressors using midodrine following the resolution of septic shock. 140 patients weaned using midodrine were compared to 135 patients weaned without midodrine. Prior to starting midodrine, the average vasopressor requirement was either 0.09 +/- 0.09 mcg/kg/min norepinephrine or 1.05 +/- 0.77 mcg/kg/min phenylephrine. Although the study wasn't randomized, the two groups were fairly well matched (Table 1 on right).
Midodrine use correlated with a lower duration of IV vasopressor use and ICU length of stay (Table 3 on right). Transitioning to midodrine also correlated with a lower rate of re-starting intravenous vasopressors (5% vs. 15%). Perhaps most provocative, midodrine was associated with a lower rise in serum creatinine (0.5 vs. 0.8 mg/dL, p=0.048).
There were no complications associated with midodrine except for transient bradycardia in one patient, which resolved following discontinuation. 87% of patients discontinued midodrine while in the hospital, with an average duration of six days treatment.
This retrospective study cannot prove causality. For example, it is possible that more robust patients were selected for midodrine therapy. Nonetheless, it is notable that patients treated with midodrine experienced less hemodynamic instability (defined as hypotension requiring re-initiation of IV vasopressor) and less renal impairment. This suggests that using midodrine to perform a more gradual vasopressor wean could improve perfusion and renal function. Alternatively, patients weaned without midodrine may have been under pressure to terminate vasopressor therapy prematurely, in order to facilitate transfer out of the ICU (as in choice [C] above).
Physiologic effect of midodrine
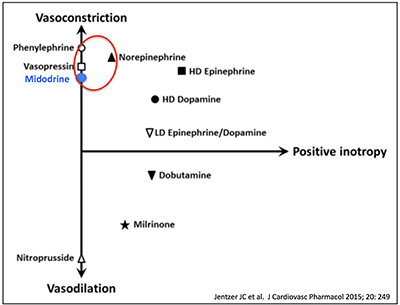 Midodrine is essentially an oral equivalent of phenylephrine, another alpha-1 agonist. It is commonly feared that alpha-1 agonists may decrease cardiac output and impair renal function. However, this fear does not appear to be justified regarding the use of low doses of alpha-1 agonists in vasodilatory shock.
Midodrine is essentially an oral equivalent of phenylephrine, another alpha-1 agonist. It is commonly feared that alpha-1 agonists may decrease cardiac output and impair renal function. However, this fear does not appear to be justified regarding the use of low doses of alpha-1 agonists in vasodilatory shock.
As explored previously, alpha-1 agonists have a similar mechanism of action compared to norepinephrine. Specifically, they may increase both preload and afterload, with a tendency to maintain or increase cardiac output in sepsis. Midodrine is known to improve renal function in hepatorenal syndrome, a vasodilatory state similar to septic vasoplegia. Overall, midodrine should be able to substitute for a low dose of phenylephrine, vasopressin, or norepinephrine.
Pharmacology & dosing
Following oral administration, >90% of midodrine is rapidly absorbed. Midodrine is an inactive prodrug, which is rapidly converted to its active metabolite desglymidodrine. Levels of desglymidodrine peak within 1-2 hours, with a subsequent half-life of 3-4 hours (80% being excreted in the urine). Midodrine is typically administered every eight hours when used in the ICU for blood pressure support (not “three times daily with meals,” which will generate uneven dosing intervals). The half-life of desglymidodrine increases up to 10 hours in end-stage renal disease, which may require extending of dosing interval (House 2011).
Whitson 2016 utilized an initial dose of 10 mg q8hr, with an average required dose of 19 +/- 10 mg q8hr (the maximum allowed dose was 40 mg q8hr). Levine 2013 also reported that the most commonly required dose was 20 mg q8hr. Thus, a reasonable approach may be to start dosing at 10 mg q8hr with rapid escalation to 15-20 mg q8hr if needed. Among patients with severe renal dysfunction, the dosing interval may be extended, for example from q8hr to q12hr (1).
Benefits of liberation from IV vasopressor
Oral vasopressors may potentially reduce ICU length of stay, while avoiding complications such as central line infection and delirium. Faster transition from the ICU could facilitate greater mobility, avoiding deconditioning.
Oral vasopressors could also reduce costs. One day in the ICU costs roughly $2,500, whereas midodrine costs under $50/day. Now, let's suppose that oral midodrine might reduce ICU length of stay by an average of one day for every patient admitted with septic shock who don't require intubation (2). Multiplied out over 180,000 such admissions per year in the US, this could save $441 million dollars per year in the US.
Safety & contraindications
Potential complications of midodrine include supine hypertension, reflex bradycardia, urinary retention, piloerection, shivering, and paresthesias. Overall, midodrine is a fairly safe medication, which has been prescribed to outpatients since the early 1980s. This supports the safety of titrating midodrine in the ICU with close monitoring. Contraindications to midodrine include urinary retention, pheochromocytoma, and thyrotoxicosis.

- Some patients recovering from septic shock develop a state of persistent vasodilation (“vasoplegia”) which may take a few days to resolve. This delays discharge from ICU due to a persistent requirement for low-dose intravenous vasopressors.
- Midodrine is an oral alpha-1 agonist, with the same mechanism of action as phenylephrine. It is a fairly safe drug which has been used among outpatients for decades.
- Several reports support the use of midodrine to facilitate weaning off intravenous vasopressors in appropriately selected patients with careful monitoring. This may reduce ICU length of stay, avoiding ICU complications (e.g. central line infection and delirium).
This is the second of a four-part series on hemodynamics. Stay tuned for the next installments, which will be administered q2weeks barring any unforeseen adverse events.
Related topics
- Hemodynamics I: An alternative viewpoint on phenylephrine infusions (PulmCrit)
- Vasopressor Basics (EMCrit)
- Early initiation of norepinephrine in septic shock (PulmCrit) Note: the rationale for starting norepinepinephrine early also argues for continuing a vasopressor for a longer duration with gradual taper.
- Collapsed IVC doesn't equal hypovolemia (PulmCrit)
Notes
- Renal failure is not necessarily a contraindication (for example, midodrine has proven efficacy when given immediately prior to hemodialysis to reduce intra-dialytic hypotension and Whitson 2016 included some patients on hemodialysis in their study). However, the ideal dosing regimen in renal failure is unclear. One approach might be to extend the dosing interval from q8hr to q12hr, with re-assessment of vital signs prior to each dose. Thoughtful manual titration to effect should avoid the risk of drug accumulation.
- My guess is that midodrine wouldn't reduce the ICU length of stay so much for patients who require intubation, because weaning from the ventilator is more often the factor delaying transfer out of the ICU.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Josh – another hugely helpful clinical topic and review that will benefit patients, except you missed a major trial that was JUST published, supporting the utility of it’s use: Paul, Seth, Mangala and one of their stellar residents (Micah Whitson), performed a “prospective” trial on the topic in Chest 2 weeks ago, comparing 140 pts treated with midodrine vs 135 without… Basically shows the same utility you argue for above, but with bigger numbers and substantial ICU LOS reduction…
Whoops, just saw that you did review Whitson et al (you had it as 2014 which is why I missed it, however, shame on me for thinking you would miss it!!). That paper, for me, is now stimulating significant interest in the practical benefits of using midodrine in such patients – thanks as always for the thoughtful topics and reviews!
Hi Pierre, great to hear from you. Thanks for pointing out that I got the date wrong on Whitson et al (I’ve corrected it now). What happened is that I wrote the blog before the Whitson manuscript was released, initially including a 2014 abstract by the same group. When Whitson was release I up-graded the entry but failed to change the date. I really like these papers because I must admit that I’ve done this occasionally for a long time and it always felt a bit like cheating. It worked, but there was always a nagging doubt that perhaps I… Read more »
Hey Josh, It gets worse than “three times daily with meals” dosing for midodrine. The correct dosage schedule for orthostatic hypotension is 3 times daily during daytime hours (every 3 to 4 hours) when patient is upright. In one of my previous institutions, this led to a dosing schedule of 0800, 1130, and 1400. This is typically “pre-filled” into the CPOE and the ordering resident will have to go in and manually alter it. I would say that > 75% of our attempts at using midodrine in the ICU at this previous institution were scheduled incorrectly, and this would typically… Read more »
I can’t agree more. I am continually confounded by errors regarding electronic order entry (including my own), most commonly failure to check off the boxes “first dose now” and “stat.” Thus, a common error is to order an antibiotic for someone with septic shock at 2AM but the first dose doesn’t end up being scheduled until 8AM. I’ve run into two errors when ordering midodrine, similar to what you’ve mentioned: (1) When you first order midodrine it comes up “TID with meals” – which is no good (2) There is a “Q8hr MN – 8 AM – 4 PM” option.… Read more »
So, is it presumptive to attempt to use oral midodrine in ED patients who are borderline ICU players? For example, I had a 68 yo with a pneumonia who was maintaining her MAP on a low dose norepi gtt but would dip to a MAP of 55-60 when the gtt was d/c’d. ICU was chock-a-block full and stepdown unit doesn’t do vasopressor gtt’s. Since she was with us most of the night, had sufficient time to gauge the benefit under close observation.
Great question. I was tempted to speculate about this in the blog post, but I figured that there wasn’t much evidence about it so it might get me into hot water. But here goes… I think there is a broad range of reasonable approaches to vasopressors, with the most important thing being that you observe the patient and make sure that they’re responding the way you want them to. My guess is that if you start midodrine and observe the patient for sufficient time (i.e. 6-8 hr) and they’re doing great, that’s probably fine – especially if you’re sending them… Read more »
I was curious about ED use too. However, the down side to observing in the ED for 6-8 hours is going to cause the heat to be turned up regarding ED LOS/delaying ICU transfer if indeed it becomes required… I suppose it’s a catch 22.
Thanks for the great blog, I’m kicking myself for not trying this sooner!
Currently there isn’t any evidence about using midodrine up-front in sepsis. In the future a shorter period of observation might be validated to be safe. This might be particularly applicable to certain types of sepsis which are highly amenable to treatment, especially urosepsis. It’s not hard to imagine an accelerated urosepsis therapy pathway for patients with mild sepsis who really look OK and are only moderately hypotensive (i.e. start antibiotics, fluid, and low-dose midodrine *simultaneously*… observe for 2-3 hours then send to step-down if doing great). Unfortunately, there isn’t evidence yet that this is safe. Until such evidence exists, the… Read more »
I am a rapid response team nurse and would love to see research on a safe, calculated approach to the utility of midodrine on infected/septic telemetry/stepdown patients who have a BP that is soft, but not soft enough for ICU to accept. Inevitably the ICU makes the floor MDs give a hefty dose of “iatrogenic salt water drowning” before they will accept the patient (who now needs ICU due to lung injury). I suspect some of these patients could stay out of ICU altogether if they just got a bit of BP support. My institution only allows low dose pressors… Read more »
Absolutely agree, would be great to see more research on this.
Although the concept of oral vasopressors in a non-ICU setting may be scary, the all-to-common approach of massive hydration in efforts to avoid vasopressors may be more harmful.
I had a big reply here that was eaten by the ether…anyway, the basic point was that a decent tele floor or stepdown could handle the burden of initiating oral vasopressors. The problem isn’t where it starts. The problem is, without data and a healthy respect for the error factor, good ideas can result in poor outcomes. I’m uncomfortable with starting those meds for a wide range of soft BPs for a wide assortment of reasons, on different patients, on different floors with different monitoring systems…I have control issues. In fact, drowning patients before accepting them into the ICU is… Read more »
Thank you for publishing and maintaining this resource. I’ve seen midrodrine work well as a bridge to move a patient along, but I’ve also seen those patients return. Not that it’s any different than any other ICU patient–if you never have one come back, you’re waiting too long to move them out. Flippancy aside, another technique for patients with persistent vasodilation during gtt weaning: ensure your gtt is single-strength and turn it down by 0.5-1cc/hr. Some of the facilities I work at don’t use midrodrine except for postural hypotension or prior to dialysis, and when I work there this technique… Read more »
Thanks. Yes, transferring patients out of the ICU is a bit like extubation. If you never have a patient bounce back, or never have an extubation failure, that means that you’re not being aggressive enough about extubating/transferring patients. Of course, if there is too high of a bounceback rate or extubation failure rate, that’s not good either.
I want to know when to introduce midodrine exactly when the patients are on vasopressors
Hi Josh, I read this post when it came out and as an existing midodrine fan I was very encouraged, though wary of confirmation bias! I’ve been using it pretty much as you have for while and really feel it reduces ICU LOS in a certain suitable cohort. I also use it when on the wards with the Rapid Response Team and have definitely kept people out of ICU that would otherwise have come as low acuity admissions. Matt Anstey from Perth and colleagues in Boston are doing this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5361788/ Will be interesting to see the results. I’m creating… Read more »
Here’s a new paper on the topic
https://link.springer.com/article/10.1007/s00134-020-06216-x
Hi Dr. Farkas. I’m sorry, I know this blog is seven years old. However, I have been searching like crazy to find a citation to one of your comments, “by the time someone has been in a North American ICU for three days with urosepsis, it is essentially impossible that they will be volume depleted”. In addition, I noticed that Ali, et al cited you in their paper on midodrine and spinal shock concerning this quote. Really was hoping I could reach out for the reference. The message will echo greatly within our CCM APP group. Thanks in advance if… Read more »