

Large-volume regurgitation is an uncommon airway problem, which is mostly encountered in the prehospital setting, ED, or ICU. It is sufficiently rare that it is commonly ignored. An average clinician might encounter severe regurgitation once every 2-5 years, which is infrequent enough to write it off as a “freak” event that doesn't mandate practice change (1). However, this may be fatal, so despite its rarity it deserves to be addressed systematically. Perhaps the easiest systematic practice change would be to improve our choice and utilization of suction catheters.
The Yankauer catheter sucks at intubation
The Yankauer suction catheter was designed by Sidney Yankauer around 1907 to facilitate clearing the surgical field during tonsillectomy. The tip of the Yankauer has small holes, to allow the gentle removal of blood without traumatizing delicate tissue.
The Yankauer fails to manage large-volume regurgitation. The flow rate is proven to be lower than large-bore suction catheters (Andreae 2016). The small holes of the Yankauer are easily clogged with debris (Kei 2017). The ideal suction tool for intubations is debatable, but it seems clear that the Yankauer is a poor choice. Persistent use of the Yankauer suction catheter for airway management represents a profession-wide failure in our ability to manage large-volume regurgitation.
Requisite features of any suction device used for intubation
An ideal suction tool for intubation should have the following features:
- Appropriate geometry for deployment during direct or indirect laryngoscopy.
- Large internal diameter and hole size, which largely eliminates clogging by particulate matter.
- Ability to pass a bougie or airway exchange catheter through the suction device (more on this below).
The Yankauer has feature #1, but lacks #2-3. The large-bore suction devices discussed below satisfy all three of these criteria.
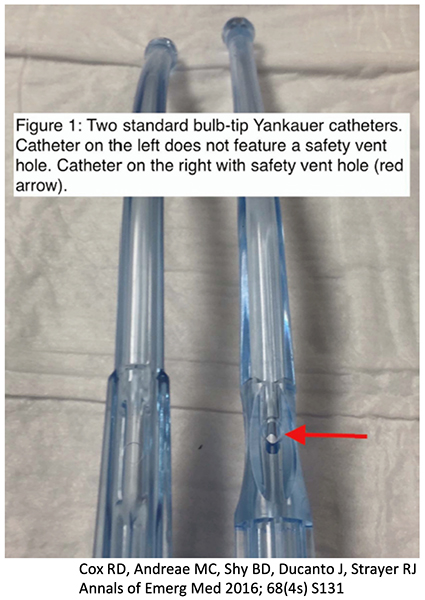 Some suction catheters have a safety vent hole on their side, which prevent the catheter from suctioning too hard. This may be desirable for delicate surgical procedures, but it's a design flaw with regards to intubation. The vent hole must be occluded by the operator's finger to achieve optimal suction during intubation. However, during simulated intubations, operators often failed to occlude the vent hole promptly, thereby extending the procedure duration (Cox 2017). An ideal suction catheter would lack any such hole. However, if your catheter does have a hole, this problem is easily fixed by wrapping tape around the hole before the procedure begins.
Some suction catheters have a safety vent hole on their side, which prevent the catheter from suctioning too hard. This may be desirable for delicate surgical procedures, but it's a design flaw with regards to intubation. The vent hole must be occluded by the operator's finger to achieve optimal suction during intubation. However, during simulated intubations, operators often failed to occlude the vent hole promptly, thereby extending the procedure duration (Cox 2017). An ideal suction catheter would lack any such hole. However, if your catheter does have a hole, this problem is easily fixed by wrapping tape around the hole before the procedure begins.
Basic maneuvers with a large-bore suction device
Three basic strategies are as follows:
Intermittent suction
This is the most common way to use a suction catheter. The operator inserts the suction catheter to clear the airway, then removes the suction catheter prior to inserting the endotracheal tube. This works fine for the vast majority of intubations. However, if regurgitation is ongoing, then intermittent suctioning will fail (as soon as the operator removes the suction catheter, the oropharynx rapidly fills with vomitus).
Continuous suction
This technique is useful to manage a situation with ongoing regurgitation. The suction catheter is inserted and left in place while the endotracheal tube is being placed. Thus, the suction catheter can continuously remove fluid from the oropharynx throughout the entire procedure. Dr. Ducanto has dubbed this technique the “Salad Park Technique” in reference to “parking” the suction catheter at the left side of the laryngoscope (illustrated in the video below). This technique may also be facilitated by having a second operator maneuver the suction catheter during intubation.
Seldinger technique
A large-bore suction device may facilitate intubation using a Seldinger technique, with a bougie (or airway exchange catheter) acting as the “guidewire:”
- First, the large-bore suction catheter is inserted through the vocal cords into the upper trachea
- A bougie is then inserted through the suction catheter, into the trachea.
- The suction catheter is removed, while keeping the bougie in place within the trachea.
- An endotracheal tube is advanced over the bougie into the trachea.
This technique may be helpful in the following situations:
- The patient has a small mouth which doesn't allow for simultaneous passage of a suction catheter and endotracheal tube (making the continuous-suction technique described above impossible).
- Waves of vomitus are threatening to completely occlude the view of the glottis. In this situation, immediately inserting the suction catheter into the trachea will secure access to the trachea and also simultaneously suction out fluid that may be in the trachea. This avoids the risk of losing visualization of the glottis and then being unable to intubate the patient. The concept is that while you have a view of the glottis you should take the shot, because you could lose visualization later. This scenario is demonstrated in the following instructional video (2):
Commercial large-bore suction devices
 Two leading commercial suction catheters are shown above. The Hi-D “big stick” catheter has a geometry suitable for direct laryngoscopy (mostly straight, with mild angulation at the end). The DuCanto catheter has a more graded curve, which facilitates use with hyperangulated videolaryngoscopy.
Two leading commercial suction catheters are shown above. The Hi-D “big stick” catheter has a geometry suitable for direct laryngoscopy (mostly straight, with mild angulation at the end). The DuCanto catheter has a more graded curve, which facilitates use with hyperangulated videolaryngoscopy.
Both of these catheters are available for ~$2 each, which is only trivially more than a Yankauer catheter (~$1). My opinion is that the Yankauer should be banned from use in airway management, replaced instead by routine use of large-bore devices such as these.
MacGyvered large-bore suction devices
Endotracheal tube suction using a meconium aspirator
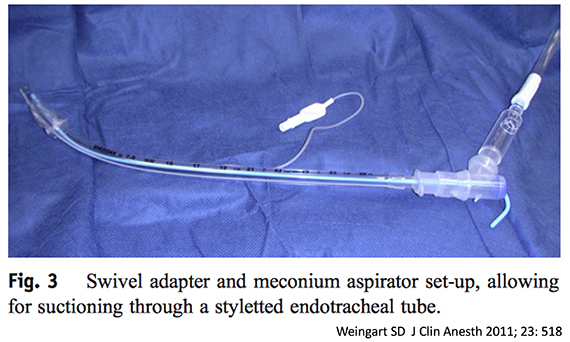
Many hospitals lack commercial large-bore suction devices, which has led to the creation of a variety of work-arounds. This was first proposed by Scott Weingart, who described how to create a large-bore suction device using an endotracheal tube connected to a meconium aspirator (figure below). The stylet can be shaped into any configuration desired, to accommodate either a straight-to-cuff geometry (for direct laryngoscopy) or a more gradual curve (for hyperangulated videolaryngoscopy). This is elegant, but it does have the drawback of requiring a swivel adaptor and meconium aspirator.
Endotracheal tube suction without an adaptor
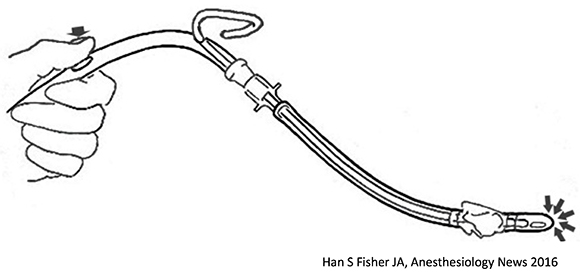 A similar strategy has been described more recently by Han 2016. This involves attaching the suction catheter directly to the endotracheal tube. The stylet may be allowed to poke out of a hole in the suction catheter (figure above). Alternatively, the stylet may be straightened out, so that it fits entirely within the suction catheter. Depending on the specifics of your suction tubing and endotracheal tubes, this can be a bit tricky to construct.
A similar strategy has been described more recently by Han 2016. This involves attaching the suction catheter directly to the endotracheal tube. The stylet may be allowed to poke out of a hole in the suction catheter (figure above). Alternatively, the stylet may be straightened out, so that it fits entirely within the suction catheter. Depending on the specifics of your suction tubing and endotracheal tubes, this can be a bit tricky to construct.
Suction tubing taped to a stylet
The simplest way to create a large-bore suction catheter is to tape suction tubing directly to an endotracheal tube stylet (figure below). The main advantage of this strategy is that it is very easy to set up using universally available materials. It also provides the largest-bore suction which is possible to create, without any junctions which may allow particulate material to lodge and occlude the suction device (5).
 The suction tubing may be large enough to allow passage of an airway exchange catheter or bougie (3). This allows for the Seldinger maneuver to be performed if needed (figure below):
The suction tubing may be large enough to allow passage of an airway exchange catheter or bougie (3). This allows for the Seldinger maneuver to be performed if needed (figure below):
- Pass the suction catheter through the cords into the trachea
- Cut off the tubing of the suction catheter (this will sacrifice the ability to use this device for suction).
- Pass a bougie through the suction catheter, into the trachea.
- Remove the suction catheter, keeping the bougie in the trachea.
- Pass an endotracheal tube over the bougie into the trachea.


- Yankauer suction wasn't developed for intubation, nor does it work well for this situation. Persistent use of the Yankauer for airway management represents a system-wide failing of modern medicine to manage regurgitation.
- Large-bore suction catheters are less likely to be clogged by vomitus and may allow for securing the airway directly using a Seldinger maneuver.
- Commercial large-bore suction catheters are only trivially more expensive than Yankauer catheters and should replace Yankauer suction devices for routine use in airway management (because it's impossible to predict regurgitation with 100% certainty).
- For practitioners who lack access to commercial large-bore suction devices, there are various ways to MacGyver a large-bore suction device. This may be reasonable for selected situations where a patient is at higher risk for large-volume regurgitation.
Related
- Novel set-up to allow suctioning during direct endotracheal intubation (EMCrit)
- Having a vomit SALAD with Dr. Jim Ducanto (EMCrit) – including numerous links at the bottom of this page.
Notes
- Large-volume regurgitation has recently gained a lot of attention in the FOAMed community, largely due to the work of Dr. DuCanto and his large-volume regurgitation simulator. However, many emergency and critical care providers continue to have little awareness of this issue.
- The take-the-shot strategy admittedly didn't work well in this video, illustrating the importance of using this approach only if you have a clean shot (i.e. good visualization of the glottis and vocal cords).
- If the bend at the tip of the suction catheter is too sharp, the bougie will hang up at this angle and will not pass. For this reason, the suction catheter should generally be shaped with a gentle angle (e.g. closer to ~15% than ~30%). It may also be easier to pass an airway exchange catheter instead of a bougie, because the airway exchange catheter is smaller and floppier. This may also depend on the exact diameter and pliability of the suction tubing that you are using (if you are using small-bore tubing this will cause problems on multiple levels).
- There's not much literature about large-volume regurgitation, because this is too rare of an entity to study thoroughly. The rarity of this event also makes it difficult for any practitioner to get extensive experience with it. I make no claim to be an expert on this topic, but instead look forward to a discussion which may pool the experience of many airway experts.
- The internal diameter of this suction device is equal to the internal diameter of the suction tubing itself. This is the largest bore suction device which can possibly be created. In theory you *could* design a larger-bore catheter, but that wouldn't work any better (because the suction would still be limited by the internal diameter of the suction tubing).
Conflicts of Interest: The SSCOR company provided me with two free DuCanto catheters as a promotional offer which is publically and freely available to anyone. I don't think this is a significant COI, but you can be the judge.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Even more basic is to use an 8.0..endotracheal tube and flip the tube connector on the back end and connect the entire modified tube onto suction tubing. Suction better than any yankuer..out there.
Best use for me has been with the channeled devices like the king vision. Even usable with the airtraq.
Ducanto has many videos with channel-less devices like the C-mac..and g lidescope.
Just remember other video laryngoscopy..designs exist as well.
Hi Josh, it’s Jim DuCanto! Loved the post (of course!). Nothing to add except that I have used the bougie through the suction catheter maneuver clinically in order to reliably use a bougie with the Glidescope and D-Blade (Storz), but this is an off-label use of the suction catheter, and the manufacturer would want me to publicly state that until a time arrives that we have published evidence to present that would allow the catheter to be labelled as such. I would be interested in anyone who does implement this technique clinically (of their own volition, not due to my… Read more »
Thanks Jim, great to hear from you. I really appreciate the tremendous work you’ve done on this topic. Thanks to your work with the SALAD simulator, I think that there is a good level of awareness about these issues in the FOAMed community. However, most hospitals are continuing to use the Yankauer catheter and aren’t very aware of these problems. So I think there is still a lot of work to do in the knowledge-translation department. If you look hard in the literature, people have recognized for decades that we need better suction catheters, but nothing has been done about… Read more »
A Novel Intubation Technique: Bougie Introduction Via DuCanto Suction Catheter
https://www.jem-journal.com/article/S0736-4679(23)00545-0/pdf
So we’re teaching SALAD at most airway workshops now – thabks to Jim DuCanto. Currently running through just the above on Chris Nickson’s wildly popular and oversubscribed Critically Ill Airway course down in Melbourne. Everyone loves SALAD sim
Love it that you have used our Merlion as the banner for the post!
Hi Josh. I think this is a really cool post that may have more applicability to routine practice than you think. Although large-volume regurgitation is rare and terrifying, we are using Yankauers for suction during RSI frequently and always have a Yankauer ready for use when necessary. You’re right that Yankauers are not ideal suction catheters for intubation. Anyone who has used a hard-angle VL blade such as the Glide or C-Mac D blade and then tried to use a Yankauer for suction has probably been frustrated with their suction setup. I do not think we have DuCanto suction catheters… Read more »
Yes great point, another problem I should have pointed out with the Yankauer is that it doesn’t work well with hyperangulated videolaryngoscopy.
Does the Yankhauer narrow toward the tip or is it a consistent internal diameter? If the latter, wonder if cutting off the tip with some trauma shears may improve flow.
Cutting rigid plastic may cause sharp edges resulting in tissue trauma….
yeah, unfortunately there are many problems with this
1) cutting the plastic may cause sharp edges
2) if you cut off too much, then the length/shape of the catheter may be inadequate
3) the Yankauer has a smooth/tapered shape, so even if you cut off the end, the internal diameter will still be too small to use as a true large-bore suction device
Josh, thank you for the thoughtful discussion of this technique. We use a projectile vomiting airway simulator (vomit = soapy water + food coloring + deflated balloons + gummy bears) to make the esophageal suction “parking” less effective. We have found the technique of intubating the larynx with the “big stick” suction and then proceeding to use a bougie a smart solution to this problem and a viable clinical option if patients have adequate preOx & ApOx.
Brilliant. You might consider trying to do a simulation-style study on this. I think the seldinger technique has a lot of potential that we yet haven’t tapped into, because we’re still using these damn Yankaeur catheters.
I found working with Yankaeur rather frustrating. I echo you Josh: Damn you Yankaeur! On another note, has the concept of large bore suction catheter and tubing being explored to its fullest? If we are limited by the inner diameter of the suction tubing, why not make extra large bore tubing? It seems to me like it would have less chance of getting clogged by chunks or extra thick emesis?
Excellent Josh. i suspect its just as effective for massive upper GI bleeds with hematemesis or pharyngeal tumor bleeds; but the pathway for massive hemoptysis has been addressed elsewhere recently on emcrit, and some tips may be transferrable to the latter i think.
thank you, josh very helpful.
ps: who was that in the video (not james bond). i had the pleasure of meeting him at reanimate 3.
I’ll never forget going through upwards of 6 Yankauers on a coding pediatric asthma patient whose airway was filled with chicken soup. The ET tube even clogged once through the cords. The stylet/suction tubing and Seldinger technique may have saved the poor kid’s life. Great tips. Thank you
First, I think it’s awesome that we are finally addressing a problem we’ve all known about for years. We all have our MacGyver tricks for dealing with the problem and I’m glad we’re bringing the problem to the front line. I’ve watched the SALAD technique video and I like it. I’m worried about airway trauma, something not well evaluated with airway simulators. If the choice is between getting the airway and not than the choice is easy, but has anyone had any experience with inadvertent airway trauma utilizing the “park” technique with large bore catheters?
excellent, Josh.
thank you.
very helpful.