
Management of acidosis in DKA is an ongoing source of confusion. There isn’t much high-quality evidence, nor will there ever be (1). However, a clear understanding of the physiology of DKA may help us treat this rationally and effectively.
Physiology of ketoacidosis in DKA
Ketoacidosis occurs due to an imbalance between insulin dose and insulin requirement:
 Many factors affect the insulin requirement:
Many factors affect the insulin requirement:
- Individuals differ in their baseline insulin resistance and insulin requirements.
- Physiologic stress (e.g. hypovolemia, inflammation) increases the level of catecholamines and cortisol, which increases insulin resistance.
- Hyperglycemia and metabolic acidosis themselves increase insulin resistance (Souto 2011, Gosmanov 2014).
DKA treatment generally consists of two phases: first, we must manage the ketoacidosis. Later, we must prepare the patient to transition back to their home insulin regimen. During both phases, success depends on balancing insulin dose and insulin requirement.
Phase I (Take-off): Initial management of the DKA patient with worrisome acidosis
 Let’s start by considering a patient who presents in severe DKA with worrisome acidosis. This is uncommon. Features that might provoke worry include the following:
Let’s start by considering a patient who presents in severe DKA with worrisome acidosis. This is uncommon. Features that might provoke worry include the following:
- bicarbonate < 7 mEq/L
- pH < 7 (if measured; there is generally little benefit from measuring pH)
- clinically ill-appearing (e.g., dyspnea, marked Kussmaul respirations)
These patients generally have severe metabolic acidosis with respiratory compensation. This creates two concerns:
- If the metabolic acidosis worsens, they may decompensate.
- The patient is depending on respiratory compensation to maintain their pH. If they should fatigue and lose the ability to hyperventilate, their pH would drop. It is important to reverse the acidosis before the patient may fatigue or develop respiratory failure (e.g., due to aspiration or pulmonary edema)(2).
There are several measures that may be used to stabilize and improve these patients.
(1) Give an adequate dose of insulin
The key therapy for ketoacidosis is insulin. The sicker the patient is, the more insulin they will need (because acidosis, hyperglycemia, and stress increase insulin resistance). For the sickest DKA patients, the usual insulin infusion of 0.1 U/kg/hr often won’t be enough.
Loading bolus of insulin
Giving a 0.15 U/kg IV insulin bolus before starting the drip used to be the standard of care. This has currently fallen out of favor given evidence that it isn’t necessary. Studies in adults have found neither significant benefit nor harm from using an insulin bolus (Kitabachi 2008, Goyal 2010).
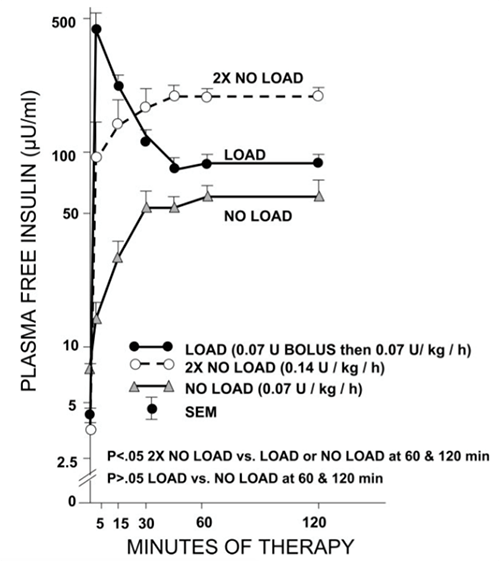 After starting an insulin infusion, blood insulin levels increase rapidly (figure above, Kitabachi 2008). Omitting a loading bolus may cause levels to be subtherapeutic for ~15 minutes, which isn’t important.
After starting an insulin infusion, blood insulin levels increase rapidly (figure above, Kitabachi 2008). Omitting a loading bolus may cause levels to be subtherapeutic for ~15 minutes, which isn’t important.
 However, there is a different way to bolus insulin that may be more useful. It takes ~45 minutes for pharmacy to mix up an insulin infusion and deliver it to the unit. Meanwhile, most EDs and ICUs stock 10-unit vials of insulin which can be given immediately. Therefore, pulling a 10-unit vial of insulin from the Pyxis and bolusing it into the patient will achieve a therapeutic insulin level about an hour earlier than ordering a drip from pharmacy.
However, there is a different way to bolus insulin that may be more useful. It takes ~45 minutes for pharmacy to mix up an insulin infusion and deliver it to the unit. Meanwhile, most EDs and ICUs stock 10-unit vials of insulin which can be given immediately. Therefore, pulling a 10-unit vial of insulin from the Pyxis and bolusing it into the patient will achieve a therapeutic insulin level about an hour earlier than ordering a drip from pharmacy.
This doesn’t matter for most DKA patients. However, getting insulin on board immediately makes sense for the sickest patients. Although the efficacy of a loading bolus is debatable, this was used routinely for years and appears safe in adults (it may increase the risk of cerebral edema among pediatric patients)(3).
Some protocols fail to give enough insulin
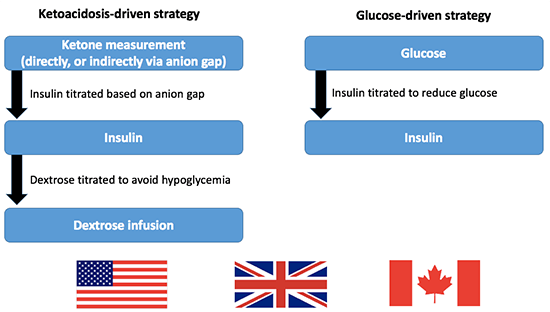 Insulin titration in DKA may be driven by either ketoacidosis or glucose (above). For example, the American guidelines recommend titrating the insulin based on the glucose level (Kitabchi 2009). Alternatively, the Canadian guidelines recommend insulin titration based on the degree of ketoacidosis. British guidelines use a hybrid strategy, with monitoring of both ketones and glucose (4).
Insulin titration in DKA may be driven by either ketoacidosis or glucose (above). For example, the American guidelines recommend titrating the insulin based on the glucose level (Kitabchi 2009). Alternatively, the Canadian guidelines recommend insulin titration based on the degree of ketoacidosis. British guidelines use a hybrid strategy, with monitoring of both ketones and glucose (4).
Either strategy usually works. However, sometimes a glucose-driven protocol won’t provide enough insulin to control the ketoacidosis. Reasons this may occur include:
- Occasional patients have a severe ketoacidosis without much hyperglycemia. The most extreme example of this is euglycemic DKA, which involves ketoacidosis despite normal glucose (due to pregnancy, starvation, or glitflozins)(5).
- Serum glucose may initially fall simply due to dilution from large-volume resuscitation. Glucose-driven protocols will interpret this drop as evidence that the insulin dose is adequate (even when it isn’t).
If your hospital uses a glucose-driven protocol, it is important to be aware of this pitfall. In some cases it may be necessary to deviate from the protocol in order to provide higher doses of insulin (with additional dextrose supplementation as needed to prevent hypoglycemia)(6). This should be considered whenever ketoacidosis isn’t responding to per-protocol therapy.
(2) Avoid normal saline
DKA patients are often quite volume depleted. Volume resuscitation indirectly helps them resolve their acidosis, since it reduces the physiologic stress that they are under (thereby decreasing their catecholamine and cortisol levels, which improves their insulin sensitivity).
Many guidelines recommend the use of normal saline, but this is an acidotic fluid which will worsen the patient’s acidosis. A balanced crystalloid such as lactated ringers may be preferable, as previously explored here. For most patients this difference isn’t important, but it may be relevant in patients with severe acidosis.
(3) Consider high-flow nasal cannula
If there is concern that the patient may develop diaphragmatic fatigue from Kussmaul respiration, high-flow nasal cannula (HFNC) is a reasonable consideration. The goal here is to use the flow rate to help blow off CO2 (by reducing the anatomic dead space and improving ventilation efficiency).
 There’s no literature on this. Supporting evidence includes the following:
There’s no literature on this. Supporting evidence includes the following:
- HFNC has been proven to reduce respiratory rate and work of breathing in other contexts.
- DKA patients usually won’t achieve a compensatory PaCO2 below ~10mm. With HFNC, surprisingly low PaCO2 values may be seen, supporting the concept that HFNC promotes CO2 clearance (adjacent).
This isn’t usually necessary, but it might help and it is safe. In contrast, BiPAP could carry an aspiration risk since these patients have a tendency towards gastroparesis and emesis.
(4) Bicarbonate is a distraction here.
The question that always seems to come up here is whether to use bicarbonate. This is very simply the wrong question. A better question is: what is the fastest way to resolve this patient’s ketoacidosis? (Answer: lots of insulin, fluid, glucose, potassium, treatment of any underlying process).
These patients don’t need bicarbonate – what they need is maximally aggressive management of their DKA. There is no evidence that bicarbonate works as a treatment of ketoacidosis. Bicarbonate may act as a dangerous distraction here, drawing attention away from the treatments that we should be pursuing.
Phase 2 (Landing): Treating non-gap acidosis to facilitate transition off the insulin drip
 Now let’s consider a much more common problem, which is the patient whose anion gap closes but who continues to have a non-anion gap metabolic acidosis. Often patients will be left with a bicarbonate around 12-18 mEq/L after resolution of the ketoacidosis. A non-gap metabolic acidosis occurs for two reasons:
Now let’s consider a much more common problem, which is the patient whose anion gap closes but who continues to have a non-anion gap metabolic acidosis. Often patients will be left with a bicarbonate around 12-18 mEq/L after resolution of the ketoacidosis. A non-gap metabolic acidosis occurs for two reasons:
- Resuscitation with normal saline or half-normal saline.
- Urinary excretion of ketoacids causing loss of “potential bicarbonate.”
Why should we care?
 The clinical significance of non-gap acidosis in general is debatable. In DKA, a non-gap acidosis is problematic for two reasons:
The clinical significance of non-gap acidosis in general is debatable. In DKA, a non-gap acidosis is problematic for two reasons:
- Most protocols require that the bicarbonate be >15 mEq/L before stopping the insulin drip. Therefore, persistent non-gap acidosis may delay transition off the insulin drip.
- Metabolic acidosis increases insulin resistance. My opinion is that even a mild acidosis (i.e. bicarbonate 15-20 mEq/L) may increase the likelihood of recurrent DKA after stopping the insulin drip:
 Bicarbonate is a logical therapy for non-anion gap metabolic acidosis
Bicarbonate is a logical therapy for non-anion gap metabolic acidosis

As discussed above, bicarbonate is an irrational therapy for ketoacidosis. In contrast, bicarbonate is a logical therapy for non-anion gap metabolic acidosis, because this fundamentally reflects a bicarbonate deficiency (7). Without therapy, it may take awhile for the patient’s kidneys to generate bicarbonate and correct the non-gap acidosis.
Nuts and bolts of bicarbonate repletion
The smoothest way to do this is to infuse isotonic bicarbonate towards the end of the DKA resuscitation (8). When the anion gap is nearly closed, the predicted final bicarbonate level may be estimated (assuming that the anion gap will end up ~10 mM):
Predicted Final Bicarb level = Bicarbonate level + Ketone level
Ketone level = Anion gap – 10 = (Na – Cl – Bicarb) – 10
Predicted Final Bicarb Level = Na – Cl – 10
If the predicted final bicarbonate level is significantly low, then isotonic bicarbonate may be infused (D5W with 3 amps of bicarbonate per liter, to generate a 150 mEq/L solution of sodium bicarbonate)(9). The volume of bicarbonate required can be estimated by calculating the bicarbonate deficit (a liter is usually fine).


- During a DKA resuscitation, patients may display different types of metabolic acidosis. Understanding the physiologic problem will facilitate logical and effective treatment.
- Occasionally patients present with severe ketoacidosis. Treatment for this involves maximally aggressive therapy for DKA:
- Adequate insulin doses (possibly with a loading bolus)
- Aggressive volume resuscitation with balanced crystalloid
- High-flow nasal cannula may be considered to support the patient’s respiratory compensation
- Many patients will have a mild non-gap acidosis during the resolution phase of DKA. Although not life-threatening, this may prolong the length of stay and increase the risk of recurrent DKA after stopping the insulin drip. Isotonic bicarbonate is a rational therapy for this problem.
Related posts
- DKA pearls (PulmCrit)
- Bicarb in DKA? See Chris Nickson on LITFL, Anand Swaminathan on EMDocs, Salim Rezai on RebelEM, Darrel Hughes on RebelEM.
- Insulin bolus? Darrel Hughes on RebelEM
- Euglycemic DKA: Craig Cocchio on RebelEM
- ABG/VBG unhelpful in DKA (PulmCrit)
Notes
- It would be very difficult to perform a RCT on patients with DKA and severe acidosis (i.e. pH<6.9) due to the rarity and urgency of this situation. The logistics surrounding recruitment and consent for such a study would probably be insurmountable in the United States.
- Most patients will hyperventilate more efficiently on their own than on a ventilator, so intubation is generally best avoided and won’t necessarily salvage this situation. This is discussed further here (see Pearl #3).
- Please note that this post and the entire PulmCrit blog applies only to adult medicine.
- Ketoacidosis can be measured either directly (using a point-of-care ketone meter or perhaps measuring the beta-hydroxybutyrate level) or indirectly (by measuring the anion gap). The British seem to use point-of-care ketone testing, whereas this may be less common in the United States.
- “Glitflozins” refers to a new class of oral medications for type 2 diabetes including CANAgliflozin, DAPAglitflozin, and EMPAglitflozin. These medications work by inhibiting the sodium-glucose transporter protein 2 (SGLT2), thereby causing glucose wasting via the urine. It is increasingly recognized that these can cause euglycemic DKA. More on euglycemic DKA here.
- Essentially this amounts to transitioning from a glucose-driven strategy to a ketoacidosis-driven strategy.
- Or an excess of chloride if you would prefer to think about it that way (the Stewart’s strong acid-base perspective).
- Of course, this can also be done after the anion gap is closed. Infusing bicarbonate slightly early may just speed up the process.
- An ampule of bicarbonate contains 50 mEq of sodium bicarbonate in 50 ml. Adding three ampules to a liter of D5W creates a 150 mEq/L solution of sodium bicarbonate (“isotonic bicarbonate”). The dextrose is absorbed by cells, so physiologically it doesn’t function as an effective osmole. The reason for using D5W (rather than water) is that most hospitals don’t have sterile water for intravenous infusion. Pushing ampules of bicarbonate without dilution in D5W will cause problems with hypernatremia, because bicarbonate ampules have roughly the same osmolarity as 6% sodium chloride.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Excellent review . One question. Most of the guidelines recommend holding insulin if potassium is low. Your thoughts
Thanks for pointing this out, I would agree that insulin should still be held for low potassium. This is important, although fortunately it doesn’t seem to happen too often. Most patients seem to come in with normal or elevated potassium. Potassium should generally be aggressively repleted in anticipation that it will drop; with this strategy hypokalemia usually isn’t a major holdup.
So in the setting where it takes sometime to get your electrolytes (potassium) will you suggest I start a maintenance potassium along the insulin? I must admit that most of the patients I see have normal or low postassium and rarely higher potassium values cannot give any reason.
These patients can be hypokalemic or hyperkalemic, so I would generally hold any insulin or potassium until you know what the electrolytes are. One exception would be if the EKG is strongly suggestive of hyperkalemia, then immediate treatment with insulin would make sense.
Another great practical teaching contribution. No one should die of DKA once they get to medical assistance, so your local policy needs only to be sensible. I particularly like the rationale for high-flow nasal cannula for Kussmaul dyspnoea. Intubating is very dangerous (sux, apnoea, kalaemia, acidosis and inability to reproduce efficiency of ‘spontaneous’ ventilation). Hamburgerphobia is fashionable but unnecessary (we’ve already had that debate), RCT shows Hamburger normalises glycaemia a bit quicker. Chloraemia (if it occurs) will sort itself overnight without interference. Thrilled to see your recommendation of what we used to call Woodcock’s bursting bag of 1,150ml Na 130… Read more »
Hmmm, we may have to agree to disagree on this. Regarding normal saline, I see little impetus to give an acidotic fluid to a patient with severe acidosis. I observe the effects of various fluid loading regimens very often among patients admitted to ICU. Patients who are treated with normal saline will often develop one of two patterns: (#1) anion gap decreases, chloride increases, bicarbonate stays roughly stable, or (#2) sometimes the bicarbonate will actually drop, indicating that the hyperchloremic acidosis from normal saline exceeds any improvement in the ketoacidosis. The second pattern is very frustrating, especially if the patient… Read more »
How does your final bicarb differ from the corrected bicarb which tells you whether there is a co-existing NAG met acidosis or met alkalosis with the AG met acidosis? Also is there a role for normal saline in DKA pt who is very hypochloremic?
So initially acidosis causes a shift of Potassium from inside the cell to outside the cell, correct? Is that because potassium and positively charged and it is trying to balance the acidosis which is negatively charged on the outside of the cell? Thanks for any advice.
Thanks for a great post.
Question – do you ever worry about the rapidity of correction of acidosis and hyperglycaemia (in particular, with regards to neurologic consequences like cerebral edema)? The topic came up recently with a DKA patient who came in severely acidotic – initial pH 6.6. We put him on CRRT (as well as all of the above therapies) and 6 hours last his pH was 7.4. Immensely satisfying, but made us wonder (after the fact) if there is ever danger in such rapid correction of physiologic disturbances.
i know of no evidence that rapidity of pH normalization is a risk
agree, only potential problem here is rapid correction of osmolarity. This isn’t generally a big problem with DKA, because DKA often evolves fairly rapidly (so the brain doesn’t adapt to changes in osmolarity). Also most DKA patients aren’t all that hypertonic. This could potentially be a problem for patients with true HHNS (aka HONK) with severe hypertonicity that evolves over a period of days-weeks (such that the brain has time to adapt to the hypertonicity). In particular, patients with profound hypertonicity and normal mental status that has occurred very gradually scare me. Fortunately frank HHNS is pretty rare – far… Read more »
Josh
Any thoughts on whether these principles hold fast and true for paediatric DKA. Our hospital protocol holds onto 0.9% sodium chloride with KCl in every bag until Glu is < 14mmol/L. If I asked a nurse to add KCl to Hartmanns/LR I'd get a very unimpressed look. Am I wedded to 0.9% sodium chloride in paediatric DKA forever?
Protocol appears to be very conservative and geared to slow repletion of fluid to avoid cerebral oedema.
I apologize but I don’t know anything about pediatric DKA. I only manage adults.
Josh,
Great post as always. Interesting that you mention HFNC for these patients. I have not tried HFNC for these patients, but I often sit them completely straight up (improving FRC while decreasing aspiration risk) and put them on BIPAP. This seems to work well for work of breathing as well as for improvement in ventilation.
Sam
Whatever works is great, and one advantage of critical care is that with close monitoring it’s reasonable to try lots of things (BiPAP, HFNC, etc). That said, I prefer HFNC here for a few reasons:
– these patients have a tendency to vomit
– easier to assess work of breathing and mentation with HFNC
– HFNC is compatible with giving oral potassium if you’re going to try this (it can be a reasonable approach in patients who aren’t nauseous and are very potassium depleted)
– HFNC often better tolerated
I’m a Brazilian intensivist, graduated just in may this year. I’d like to thank you for this post! Saved a patient life with 7,05 pH, and no mecanichal ventilation. 12h later patient was awake, ph 7,33, just like you said! Medicine is just amazing! Thanks once again!
fantastic! great work. DKA can be extremely satisfying when near-dead patients turn around within 12 hours.
Is this thread still active ? I would like to see your thoughts on a DKA patient that I admitted to ICU.
all threads still active although I’m not always as good about replying comments as I should be
Why would a patient have hyperchloremia prior to treatment and only have been ill for 2 days, but not critical?
Thank you for the great post. I have a question. At what point you will resume patient back on their home oral anti-hyperglycemic agents. Can they be started during the transition phase before stopping IV insulin if patient oral intake is expected to be fine or just do it at time of discharge ?
I agree that generally speaking in the initial resuscitation and treatment phase there is no role for bicarb. However what if you had a patient whom you have started appropriate DKA treatment but they present completely obtunded requiring an RSI and have a pH of 6.8. Would there be a role for giving bicarb prior to performing an RSI which could cause significant hypotension from drop in SVR and impaired myocardial contractility. Would it not be prudent to reduce extracellular acidosis temporarily for the purposes of the RSI to improve cardiac contractility and effects of vasopressors to prevent pre-intubation cardiac… Read more »
IF PH IS 6.5 WITH BICARB 4.5 LASTING FOR MORE THAN 10-12 HOURS WITH MINIMAL IMPROVEMENT OF PH >>6.81 , SAME FOR BICARB & BL GLUCOSE DROP JUST FROM 600 >>>492 MG/DL
QUESTION IS COULD INFUSION OF BICARB BE A SOLUTION ESP IF CONSCIOUS LEVEL IS WORSENING ???
Great and creative way to present the topic.
A complex topic, very lucidly explained!
hola me encanto la revision muy practica, y ademas con un sentido de humor y logica increibles, gracias