
The ProCESS trial was published less than a week ago (The night before my SMACC lecture on severe sepsis–dohhh!)
If you have no idea what I'm talking about, climb down from your mountain-top monastery, find a damn iphone and read this:
As soon as I returned to the states, I begged and pleaded with the study author, Dr. Derek Angus, to give us his thoughts, he kindly acceded.
 Dr. Angus is chair of the Department of Critical Care Medicine and Distinguished Professor and Mitchell P. Fink Endowed Chair of Critical Care Medicine at the University of Pittsburgh Schools of the Health Sciences and UPMC Health System. His accomplishments are too numerous to list here, so check out his bio page.
Dr. Angus is chair of the Department of Critical Care Medicine and Distinguished Professor and Mitchell P. Fink Endowed Chair of Critical Care Medicine at the University of Pittsburgh Schools of the Health Sciences and UPMC Health System. His accomplishments are too numerous to list here, so check out his bio page.
I will be adding a ton of stuff to this page regarding the trial ASAP; for now I just wanted to get Dr. Angus's interview up on the site.
Most Important Table
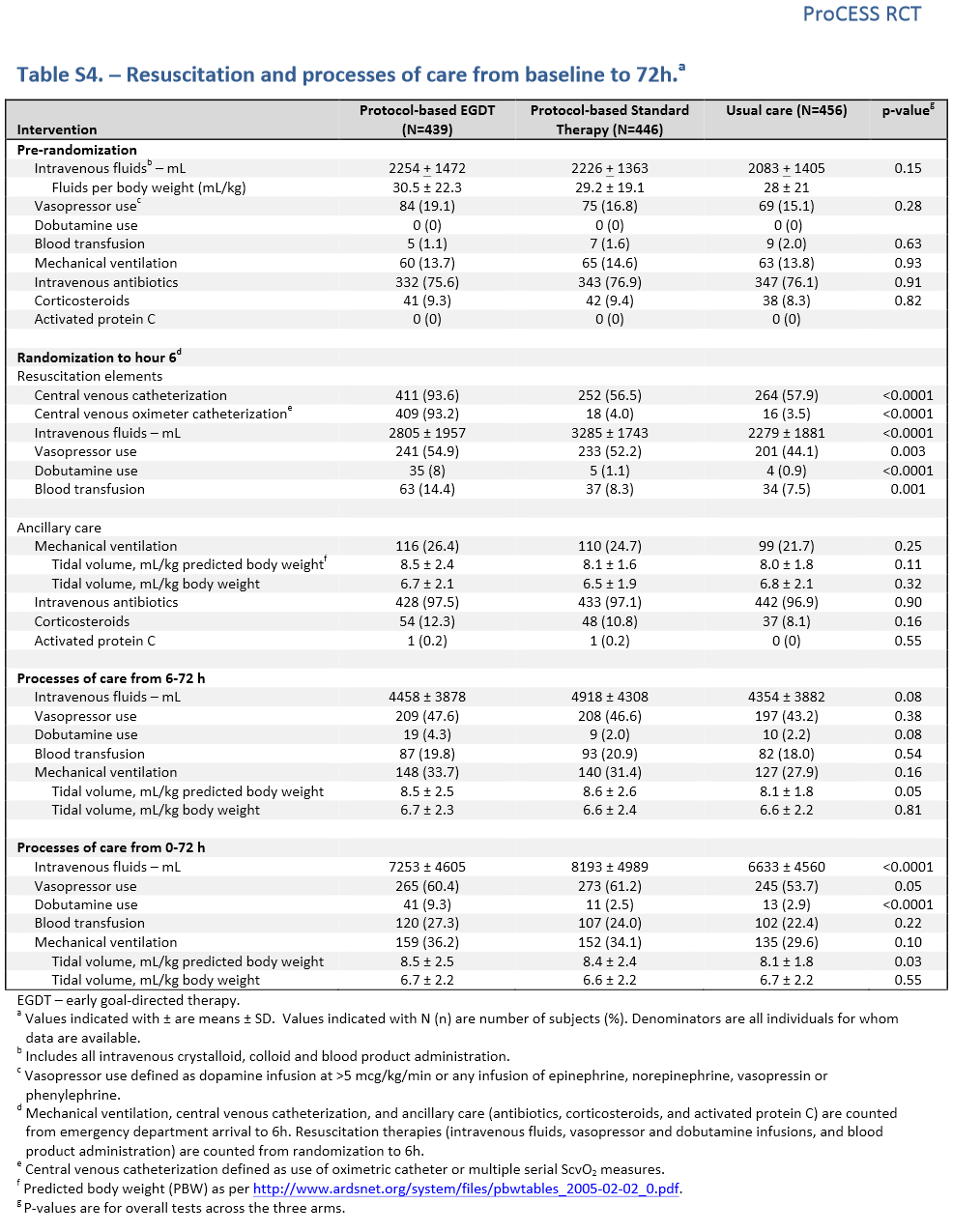
Other Stuff Mentioned
Supplementary Material for ProCESS (this is the corrected version)
High versus Low Blood-Pressure Target in Patients with Septic Shock
Excellent Posts in the FOAMcc World
Additional New Information
More on EMCrit
- EMCrit Wee – Sean Townsend of the SSC and the ProCESS Trial(Opens in a new browser tab)
- Podcast 169 – Sepsis 3.0
- Podcast 241 – Sepsis Update 2019
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Scott! Great work. Amazing the speed at which the study was published. Leading to an error in this case. (Hmmmm) It makes you wonder if all this real time Blog Podcast and #FOAMed stuff is beginning to influence how certain articles are fast tracked by even the NEJM? Are the two other related trails ARISE and PROMISE close to ready? Or is it just that this study and the whole EGDT/Surviving Sepsis story is the medical equivalent of the next Royal baby in England or the next Mrs Tom Cruise? It’s definitely PrimeTime! One way or the other; even as… Read more »
Manny is coming on the show–I’m saving it for him. Yep he changed the game and everything after is elaboration and gem polishing.
Nice job Scott.
Regarding the question above pertaining to ProMISe – is it “..close to ready?” About 45 patients left.
Warm regards as always
thanks for the update, Tiff!
Sir, is there a description of what “usual care” actually is? With all of us aware; perhaps using EGDT; it seems hard to think that it would vary much from the standard care arm. IVF and early antibiotics; pressors prn. Just a thought. Thanks for all that you do for our profession!
Neil Perera,MD
Emergency Medicine
US Army (community based practice)
My point on the cast was that aside from central lines, the groups looked mostly the same.
Hopefully the death of blood transfusion as a standard in sepsis, blood is valuable and increasingly scarce in the UK resource. We stop wasting our time with dobutamine, now we just need to persuade cardiologists that NORAD is not the devils spawn.
we moved away from transfusion until they hit 7 g/dl years ago; as to dobutamine not sure where the hatred comes from in UK and Australia–prob. b/c it was crazy expensive at what time. It is a small group that we would even argue about for the drug anyway, so not worth a hullabaloo
Scott, Thanks for the interview with Derek. Overall I think you did a nice job at identifying some practical ED resuscitation issues when interpreting this trial. A few thoughts: I think the fact that these centers had a control group mortality of around 20% leads me to think that they were so good at general resuscitation the sample size would have to be huge (if even calculable) to show any difference at all. Maybe 20% mortality is now our goal for septic shock. If I remember correctly, the Surviving Sepsis Campaign has many more centers and exponentially more patients, and… Read more »
classic poop sandwich brother : )
15,000 pts in NYC are hovering around 20%, I think that’s the standard for average urban centers. Derek said offline his practice looks very much like the standardized group (hybrid) which also matches our NYC experience. The absence of ultrasound makes me sad, but it would be hard to integrate in standardized fashion–wonder how many in usual care were guided by this.
The one thing that really hasn’t come up, which probably will when you speak with Dr. Rivers, is the fact that the initial trial (which started almost 15 years ago) used a physiologic endpoint of ScvO2 to represent a nice balance between an oxygen delivery approach to alleviate oxygen debt. If you don’t have a delivery dependent state of shock, then increasing delivery should have no benefit and only carry the risk of harm each intervention has. Unfortunately without some objective physiologic endpoint (lactate isn’t it) which will help you determine whether or not your patient is in a delivery… Read more »
Yep, fantastic point. I think Manny’s and my own population were far more likely than other centers to wait to arrive at the hospital until they are way into the supply dependence portion of their illness course. Most of the other trials, including Jones, showed there would have been a minimal impact in care regardless of ScvO2. ProCESS certainly showed a markedly lower population who required blood than EGDT trial–which may represent different patients or the fact that some patients got blood for pragmatic reasons rather than ScvO2 indices in the original trial.
Scott,
Great stuff as usual. We never did get the answer to the dobutamine question!!! I still use it if the LV isn’t contracting well. Haven’t used Milrinone in this setting.
I particularly appreciated the closing part as I don’t think this is a repudiation of EGDT so much as a validation of “there’s more than one way to skin a cat”
Mike
same with me with dobutamine. I had to cut it, but Derek stated if a fellow showed him an echo with a hypodynamic, filled heart; he would consider dobutamine.
Hi Scott,
Great interview!
A quick question (or a bit of a hijack) regarding the Caironi paper on albumin replacement. Do you think that total protein would have an impact on outcomes different from that of albumin, or is only albumin likely going to say the exact same thing?
Cheers,
Kyle
Hey Scott,
My biggest take-away from the podcast was the point that PROCESS doesn’t investigate the ABC of early sepsis care but the DEF. The patients in all groups were screened and identified early, got early antibiotics and an early couple liters of fluids. My feeling is that ABC part is the most important to be systematic and protocolized, and if that is done well, it’s 80% of the battle won.
Understanding that helps me jive how PROCESS’ equivocal findings fit in with hugely successful quality improvement projects like yours in NY.
agree–I put the number as 95% of the gain in my SMACC lecture.
Great stuff – Thanks Scott and Derek.
Hey scott, Thanks for putting this together! You state in your podcast that the amount of fluid received in the first 6 hours (T0 = randomization) was similar. However, when you look at the appendix the usual care arm received ~ 2300cc, the PSC arm received 3300cc (a liter more on AVG), and the EGDT arm around 2800 (500cc more). When looking at these numbers it may seem like a liter isn’t “that much more fluid” but as Dr. Angus mentions that is a 50% increase compared to the PSC arm in MEAN VALUES. Mean values cannot tell you about… Read more »
Hi Dave, If you add the pre-randomisation and randomisation to 6 hrs volumes then you can see where Scott gets the figures from 5l vs 5.5l vs 4.5l….
Great interview! First, I think it is fantastic that you were able to suss out for us the transposition error in the supplemental figure and I hope the print version of the paper does not reflect the error–another example of why print publication should really be banned someday… Second (a smaller point), you mentioned that the EGDT group got dobutamine 8% vs around 1% in the other groups (and that’s the first 6 hours, on the table you link above) and that you didn’t think this was a very big difference. This is just a matter of semantics/opinion, but to… Read more »
THE MAIN PIECE OF DATA MISSING FROM PROCESS IS THE PERCENT ACHIEVEMENT OF SCVO2 > 70% (OR 66% USED IN PROCESS) IN THE EGDT GROUP. IF THE BENEFIT CONFERRED BY EGDT IS THE ACHIEVEMENT OF SCVO2>70 (AS THAT WAS THE ONLY DIFFERENCE BETWEEN THE EXPERIMENTAL AND CONTROL ARMS IN RIVERS’ ORIGINAL STUDY) WE NEED TO KNOW HOW MANY OF EGDT PATIENTS IN PROCESS MET THAT GOAL. IN RIVERS STUDY ALMOST 100% OF PATIENTS IN THE EGDT GROUP MET THE SCVO2 GOAL VERSUS 60-70% IN THE CONTROL ARM.
DEFINITELY APPRECIATE THE DISCUSSION WITH ANGUS. THANKS!
To address my own comment – I found in the text that the mean (+/- SD) SCVO2 after catheterization in the EGDT group was 71 +/- 13% (page 6 above Table 1 of Process study). Therefore, Process does not debunk SCVO2 measurement particularly in the sickest of patients as the SCVO2 goal was probably not achieved in a large proportion of patients receiving EGDT.
Not so fast, here is Dr. Angus’s reply: Hi Scott, So, a quick peak at the data suggest about 88% of patients in the EGDT arm get an ScvO2 up to >70%, and 93% get an ScvO2 up to >65% in the first 6h. Of the remainder, some died before hour 6, some requested their data be withdrawn, some got a good ScvO2 after the first 6h, some just had no more ScvO2s recorded, and, presumably, in some, the docs just couldn’t get the ScvO2 fixed in 6h despite best efforts. Thus, not 100%, but darn close. We have no… Read more »
Just wanted to also state that I really appreciate Dr. Angus’ time to answer these questions. I have the utmost respect for him. Process was an excellent study and will definitely change the way these patients are managed across the world. Thank you for the reply. I think understanding the SCVO2 goal is the key to determining whether classic EGDT works. I wish that data would have been available in a table or supplement somewhere. Any chance that could happen? From the Rivers’ study, 94.9% in the EGDT group and 60.2% in the control group met the SCVO2 > 70… Read more »
Hi. Thanks for the great review here. I see that up to 6 hours a little more than 50 percent received central lines in the protocol and usual care groups. Are the numbers available to see how many patients received central lines after the 6 hours. It would be nice to see if care continued in the intensive care units without the need for the line as well. Thanks in advance for comments.
Hi Scott, Great interview. Just got around to hearing it now. A couple of points: I am quite taken aback at this “transposition” error (that’d be a copy&paste error to you and me). Not so much that it happened, because God only knows how many times I have made a mess of a table on Word or deleted the wrong row on Excel when I am rushing to put together a talk or an abstract at 3 in the morning. It’s more that I am surprised that one of the investigators was putting together a crucial table/doing a crucial bit… Read more »
John,
High-level academic research has been aptly compared to a sausage factory–trust me, you do not want to know what goes into it to make the final product.
As to the 2nd point, when you speak the SSC people, they feel the RIvers’ mortality was actually real so I get why the ProCESS guys went with that even though it seemed silly to us.
I also hate trials getting stopped early unless the results are overwhelming and will be accepted by all.