
CONTENTS
- Rapid Reference – When to consider CAPS? 🚀
- Pathophysiology
- Epidemiology & precipitating factors
- Clinical presentation
- Lab tests
- Tissue diagnosis
- Differential diagnosis
- Diagnostic criteria
- Treatment
- Podcast
- Questions & discussion
- Pitfalls
Diagnosing CAPS is challenging. A thumbnail of clues to consider the diagnosis:
epidemiological clue in ~half of patients
- Known history of anti-phospholipid syndrome.
- History of connective tissue disease (especially lupus).
- History of repeated pregnancy loss, or PE/DVT.
trigger in ~half of patients
- Infection is most common.
- Surgery or trauma.
- Malignancy.
- Anticoagulation withdrawal.
- Pregnancy or initiation of oral contraception.
- Flare of autoimmune disease.
clinical presentation frequently involves:
- Multi-organ failure (kidney > lung > neuro > cardiac).
- Skin manifestations may be a clue:
- Livedo reticularis.
- Cutaneous necrosis, digital gangrene.
laboratory abnormalities may include:
- Thrombocytopenia (~60%).
- Mild microangiopathic hemolytic anemia (20%).
- Disseminated intravascular coagulation (25%).
- Ferritin is often >1,000 ng/ml.
antiphospholipid syndrome
- This is a pro-coagulable condition caused by antibodies which bind to endothelial surfaces and trigger coagulation. Thrombosis may occur in arteries and/or veins.
- Antiphospholipid syndrome is more common in patients with lupus, but it can also occur on its own. It often presents with isolated large vessel vascular occlusions (e.g., DVT or PE).
 catastrophic antiphospholipid syndrome (CAPS)
catastrophic antiphospholipid syndrome (CAPS)
- CAPS is a severe manifestation of antiphospholipid syndrome that involves accelerated and widespread thrombosis, which may lead to multi-organ failure.
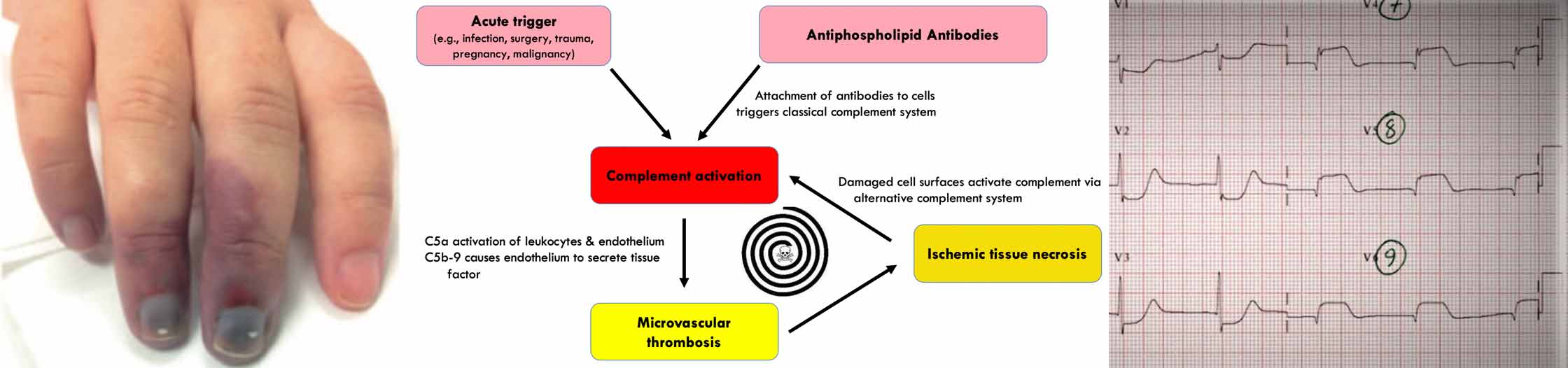
- CAPS appears to involve a vicious spiral of progressive complement activation, leading to microvascular thrombosis and tissue damage. Three general factors seem to be involved in generating this spiral:
- [1] Antiphospholipid antibody.
- [2] Genetic mutations which predispose the patient towards dysregulated complement activation. (31812994)
- [3] Triggers which stimulate complement activation (e.g. acute infection).
overall epidemiology
- CAPS is extremely rare.
- CAPS is the initial manifestation of antiphospholipid syndrome in about half of diagnosed CAPS patients. Remaining patients will carry a history of pre-existing antiphospholipid syndrome.
- Most patients with CAPS have isolated antiphospholipid syndrome, but some patients may have associated disorders (most often lupus, rheumatoid arthritis, or other rheumatologic disorders).
precipitating factor is present in about half of cases
- Infection (49%)
- Respiratory.
- Urinary tract.
- Skin.
- Gastrointestinal tract.
- Surgery or trauma (17%)
- Malignancy (16%)
- Especially hematologic: Hodgkin's and non-Hodgkin's lymphoma, acute lymphocytic leukemia, angiocentric lymphoma, chronic myelocytic lymphoma
- Solid tumors: Most often lung or colon adenocarcinoma
- Anti-coagulation withdrawal or sub-therapeutic anti-coagulation (8%)
- Pregnancy complications or initiation of oral contraception (8%)
- HELLP syndrome.
- Placental infarction.
- Pelvic thrombosis.
- Medications (5%)
- Flare of underlying autoimmune disease (e.g., lupus)(3%).(29779928)
renal failure (75% of patients)
- Acute kidney injury may occur.
- Hypertension may result from renovascular occlusion.
- Proteinuria may be seen (>500 mg/24 hours).
respiratory involvement (60% of patients)
- ARDS is a common initial presentation of CAPS (occurring in ~20% of CAPS patients overall). ARDS may occur due to a variety of different mechanisms, including:(32252584)
- Pneumonia may be the initial trigger of CAPS.
- DAH (diffuse alveolar hemorrhage).
- Pulmonary embolism is common.
neurologic involvement (50% of patients)
- Encephalopathy, sometimes to the point of coma
- Seizure
- Large vessel infarction in ~10%
- Cerebral venous occlusion
cardiac involvement (45% of patients)
- Heart failure and myocardial infarction can occur. Microvascular occlusions can cause heart failure despite a normal-appearing cardiac catheterization.
- Noninfectious, Libman-Sacks endocarditis
- Adrenal insufficiency occurs in 15%, which may contribute to shock.

skin manifestations (~40%)
- Livedo reticularis (40%)
- Cutaneous necrosis with digital gangrene (~15%)
- Purpura or splinter hemorrhages (31677977)
gastrointestinal
- Small and/or large bowel infarction.(32252937)
- Thrombotic pancreatitis.
- Budd-Chiari syndrome (hepatic vein thrombosis).
other less common manifestations
- Infarction of testes, ovaries, or prostate
- Adrenal infarction
The diagnostic strategy may vary somewhat, depending on whether the patient is already known to have antiphospholipid antibody syndrome.
laboratory testing for antiphospholipid syndrome
laboratory tests
- Anti-cardiolipin antibody (IgG & IgM).
- These are less specific (e.g. found in 1/3 of patients with heparin-induced thrombocytopenia).
- Anti-beta-2-glycoprotein type I (IgG & IgM).
- Lupus anticoagulant may be evaluated for as well. 🌊

test interpretation
- Antiphospholipid antibodies may be present in low levels, as an epiphenomenon due to other conditions which cause endothelial damage (e.g., sepsis). Thus, the mere presence of antiphospholipid antibodies doesn't establish the diagnosis.
- Antibodies will usually be present in high titers among CAPS patients. (29779928) However, it is also possible that antibodies can be consumed by thrombosis, leading to low levels.
laboratory abnormalities seen in CAPS
acute derangement of coagulation
- Thrombocytopenia (60%)
- Microangiopathic hemolytic anemia (20%)
- Lab features of microangiopathic hemolytic anemia include markedly elevated lactate dehydrogenase (LDH), low haptoglobin, and schistocytes.
- Schistocytes, if present, are usually scanty (unlike the abundant numbers seen in thrombotic thrombocytopenic purpura).(29779928)
- Disseminated intravascular coagulation (~25%)
- PTT prolongation due to lupus anticoagulant may be seen.
systemic inflammation
- Elevated ferritin levels (>1,000 ng/ml)
lab panel for investigation of possible CAPS
- Electrolytes.
- Complete Blood Count, with blood smear examination.
- Coagulation studies (including INR, PTT, D-dimer).
- Lactate dehydrogenase (LDH), haptoglobin.
- Anti-phospholipid antibodies:
- anti-cardiolipin IgG & IgM.
- anti-beta-2-glycoprotein type I IgG & IgM.
- Laboratory evaluation for lupus anticoagulant
- dilute Russel Viper Venom test.
- Anti-Nuclear Antibody (ANA).
- Definitive diagnosis of CAPS requires biopsy evidence of small vessel thrombosis, but this is often not possible (due to the patient's instability and coagulation abnormalities).
- If skin lesions are present, these may be biopsied to demonstrate thrombosis.
- The risk/benefit ratio of pursuing biopsy of other organs is unknown. (29978552)
closest mimics of CAPS (30504326)
- Microangiopathic hemolytic anemia:
- TTP (thrombotic thrombocytopenic purpura).
- HUS (hemolytic uremic syndrome HUS) & atypical HUS.
- HIT (heparin induced thrombocytopenia).
- Purpura fulminans.
- Medication-related thrombotic microangiopathy.
- Malignant hypertension
- Disseminated malignancy.
- Sepsis
- Adrenal insufficiency (note: CAPS may cause adrenal insufficiency)
- Endocarditis
- Vasculitis
- Cholesterol emboli

diagnostic criteria
- Involvement of three or more organs, systems, or tissues.
- Development of manifestations simultaneously or within less than a week.
- Confirmation by histopathology of small vessel occlusion in at least one organ or tissue.
- Laboratory confirmation of the presence of anti-phospholipid antibodies (i.e., lupus anticoagulant and/or anti-cardiolipin antibodies).
definition of CAPS:
- Definite CAPS = all four criteria. Sources disagree about whether it is necessary to demonstrate that antiphospholipid antibodies persist for six weeks after the initial episode (if anti-phospholipid syndrome wasn't previously diagnosed).
- Probable CAPS may be reached in a variety of different ways:
- All four criteria, except that only two organs/systems involved.
- All four criteria, except for absence of laboratory confirmation due to early death of a patient never tested for antiphospholipid antibodies.
- Criteria #1, #2, and #4 (everything except pathological confirmation).
- Criteria #1, #3, and #4 are met, with the development of a third event within 1-4 weeks after presentation (despite anticoagulation).
Treatment for CAPS is poorly defined, due to the rarity of this condition (no RCT-level evidence exists). To make matters more confusing, treatment often needs to be started before the diagnosis is entirely certain. Initial treatments are shown below, but hematology consultation should be obtained regarding additional therapies (e.g., rituximab, eculizumab, plasmapheresis).
general measures
- Identify and treat any underlying cause (e.g., sepsis, debridement/amputation of necrotic tissue).
- Aggressive anti-hypertensive therapy (uncontrolled hypertension may worsen intravascular hemolysis).
- Avoid intravascular catheters (especially arterial lines), as these tend to clot off.
heparin anti-coagulation
- Heparin is probably the most important treatment (correlating most strongly with good outcomes in retrospective series).
- Heparin infusion is used initially, although low molecular weight heparin also seems to work.
- Ideally, heparin infusions should be titrated against anti-Xa level (because many patients will have lupus anticoagulant, which artificially increases the PTT).
- Eventually, heparin should be transitioned to oral anticoagulation with warfarin. Case reports suggest oral anti-Xa inhibitors may not work well. (32223511)
steroid
- Rationales for steroid use:
- CAPS typically involves a pro-inflammatory state.
- Steroid could treat some underlying rheumatological disorders (e.g., lupus), potentially decreasing the production of anti-phospholipid antibodies.
- The CAPS registry shows that steroid was used in 99% of cases. Unfortunately, there is no high-quality data to support steroid use.
- The optimal steroid dose is unknown. Traditionally a pulse of methylprednisolone is used (e.g., 1,000 mg/day for 3-5 days), but it's dubious whether such a high dose is actually needed. For example, 250-750 mg methylprednisolone daily for three days could be sufficient. (29779928) The McMaster guidelines recommended against steroid monotherapy, but did recommend steroid in combination with heparin and IVIG or plasmapheresis – illustrating the level of equipoise regarding steroid. (29978552)
plasmapheresis and/or intravenous immunoglobulin
- These are both nonspecific therapies aimed at reducing the activity of anti-phospholipid antibodies. Plasmapheresis removes antibodies directly, whereas intravenous immunoglobulin may increase antibody turnover.
- Where these therapies should fit within an overall treatment strategy remains unclear. To date, retrospective case series suggest the best outcomes occur when treatment includes steroid, heparin, and either plasmapheresis or IVIG. (29779928, 29978552)
- Plasmapheresis
- Plasmapheresis might be preferred over IVIG in patients with microangiopathic hemolytic anemia or renal dysfunction (given the risk of kidney injury with IVIG). (29978552)
- IVIG
- IVIG might be preferred over plasmapheresis in CAPS patients with immune thrombocytopenia, given evidence of benefit in that condition. (29978552)
- Typical regimens include 0.4 g/kg/day for five days or 1 g/kg/day for two days.
eculizumab
- This is a monoclonal antibody that binds and inhibits complement protein C5.
- Traditionally eculizumab has been reserved for more refractory cases. However, increasing insight into the pathophysiology suggests that complement activation is a primary driver of the illness, suggesting that eculizumab may be beneficial if initiated earlier. (31812994)
- Several case reports describe efficacy at initial doses of ~900 mg weekly (analogous to the regimen of eculizumab for atypical hemolytic uremic syndrome).(32252584)
- Eculizumab increases the risk of meningococcal meningitis by ~1,000-fold, so meningococcal vaccines and antibiotic prophylaxis should be considered.
additional immunosuppression
- Rituximab:
- Cyclophosphamide is considered for patients with CAPS in the context of lupus.(32252937) Rheumatology consultation may help determine the optimal therapy.

Follow us on iTunes
The Podcast Episode
Want to Download the Episode?
Right Click Here and Choose Save-As
To keep this page small and fast, questions & discussion about this post can be found on another page here.

- Failure to consider CAPS as a competing diagnosis, in a patient with multi-organ failure who has been labeled as having septic shock.
- Delaying therapy for CAPS pending arrival at a definitive diagnosis.
Guide to emoji hyperlinks 
 = Link to online calculator.
= Link to online calculator. = Link to Medscape monograph about a drug.
= Link to Medscape monograph about a drug. = Link to IBCC section about a drug.
= Link to IBCC section about a drug. = Link to IBCC section covering that topic.
= Link to IBCC section covering that topic. = Link to FOAMed site with related information.
= Link to FOAMed site with related information. = Link to supplemental media.
= Link to supplemental media.
References
- 25694468. Maillard N, Wyatt RJ, Julian BA, et al. Current Understanding of the Role of Complement in IgA Nephropathy. J Am Soc Nephrol. 2015;26(7):1503-1512. doi:10.1681/ASN.2014101000 [PubMed]
- 28277850. Carmi O, Berla M, Shoenfeld Y, Levy Y. Diagnosis and management of catastrophic antiphospholipid syndrome. Expert Rev Hematol. 2017;10(4):365-374. doi:10.1080/17474086.2017.1300522 [PubMed]
- 29779928. Cervera R, Rodríguez-Pintó I, Espinosa G. The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: A comprehensive review. J Autoimmun. 2018;92:1-11. doi:10.1016/j.jaut.2018.05.007 [PubMed]
- 29978552. Legault K, Schunemann H, Hillis C, et al. McMaster RARE-Bestpractices clinical practice guideline on diagnosis and management of the catastrophic antiphospholipid syndrome. J Thromb Haemost. 2018;10.1111/jth.14192. doi:10.1111/jth.14192 [PubMed]
- 30504326. Gansner JM, Berliner N. The rheumatology/hematology interface: CAPS and MAS diagnosis and management. Hematology Am Soc Hematol Educ Program. 2018;2018(1):313-317. doi:10.1182/asheducation-2018.1.313 [PubMed]
- 30515245. Sadick V, Lane S, Fischer E, Seppelt I, Shetty A, McLean A. Post-partum catastrophic antiphospholipid syndrome presenting with shock and digital ischaemia – A diagnostic and management challenge. J Intensive Care Soc. 2018;19(4):357-364. doi:10.1177/1751143718762343 [PubMed]
- 31677977. Roit Z, Weil J, Llovera I. More Than Skin Deep: A Case of Catastrophic Antiphospholipid Syndrome. J Emerg Med. 2019;57(6):880-882. doi:10.1016/j.jemermed.2019.08.030 [PubMed]
- 31812994. Chaturvedi S, Braunstein EM, Yuan X, et al. Complement activity and complement regulatory gene mutations are associated with thrombosis in APS and CAPS. Blood. 2020;135(4):239-251. doi:10.1182/blood.2019003863 [PubMed]
- 32223511. Stammler R, Legendre P, Cacoub P, Blanche P, Piette JC, Costedoat-Chalumeau N. Catastrophic antiphospholipid syndrome following the introduction of rivaroxaban. Lupus. 2020;29(7):787-790. doi:10.1177/0961203320914363 [PubMed]
- 32252584. Skoczynska M, Crowther MA, Chowaniec M, Ponikowska M, Chaturvedi S, Legault K. Thrombotic microangiopathy in the course of catastrophic antiphospholipid syndrome successfully treated with eculizumab: case report and systematic review of the literature. Lupus. 2020;29(6):631-639. doi:10.1177/0961203320917460 [PubMed]
- 32252937 Hyde R, Chung J, Faruqi I. A 36-Year-Old Woman Presenting With Left Upper Quadrant Discomfort, Encephalopathy, and Respiratory Failure. Chest. 2020 Apr;157(4):e127-e130. doi: 10.1016/j.chest.2019.10.038 [PubMed]
