

CONTENTS
- Rapid Reference 🚀
- Background
- Clinical features
- Diagnostic tests
- Treatment
- Methanol-induced brain death
- Podcast
- Questions & discussion
- Pitfalls
labs to obtain
- Fingerstick glucose
- Electrolytes including Ca/Mg/Phos
- Lactate & Beta-hydroxybutyrate levels
- Acetaminophen & salicylate levels
- Ethanol level
- Creatinine kinase
- Ethylene glycol & methanol levels


- Ethylene glycol and methanol themselves aren't very toxic. However, alcohols are metabolized by alcohol dehydrogenase and aldehyde dehydrogenase, producing toxic metabolites:
- Ethylene glycol ==> oxalic acid ==> calcium-oxalate precipitation in the kidney, causing renal failure.
- Methanol ==> formaldehyde and formic acid.
- Metabolic conversion explains biphasic clinical and laboratory findings:
- Clinical findings are initially due to alcohol; later on, they are due to toxic metabolites.
- Laboratory findings initially show elevated levels of toxic alcohol; later this disappears, and we see only acid metabolites.
- Treatment mirrors this.
- Early on: fomepizole, to inhibit alcohol dehydrogenase (and thus prevent metabolite generation).
- Later on: once metabolites have been generated, dialysis may be needed to remove them.
mechanism of methanol toxicity:
- Mediated by formate, which is a mitochondrial toxin.
- Particularly affects retinas and basal ganglia.
mechanism of ethylene glycol toxicity:
- Glycolic acid
- Neurologic and cardiopulmonary manifestations.
- Oxalic acid
- Can cause precipitation of calcium-oxalate in kidneys and brain.
- Major driver of renal failure.
- Precipitation of calcium-oxalate may rarely cause symptomatic hypocalcemia.
common scenarios
- Suicide/homicide
- Accidental
- Recreational
- Methanol may be used intentionally or accidentally as an ethanol substitute (including “moonshine” created by incorrect distillation).
- Distribution of tainted alcohol may create epidemics of methanol poisoning.
- Three or more cases of methanol poisoning within 3 days should be considered as a possible “outbreak.” This should be actively investigated to look for other affected people.
ethylene glycol is found in:
- antifreeze, brake fluid
- household cleaning products
- pesticides
- industrial solvents (for paints, plastics)
methanol is found in:
- windshield washing fluid, antifreeze
- varnish, paint removers
- model airplane and model car fuel
- solid cooking fuel (Sterno)
- “moonshine” (incorrectly distilled alcohol)
Below are the typical symptoms when these are ingested alone. When co-ingested with ethanol, onset of toxicity may be delayed.
ethylene glycol
- Stage 1 (30 min-12 hours) – mimics ethanol intoxication
- Gastric irritation (pain, nausea, vomiting)
- Acting drunk (ataxia, nystagmus)
- May see CNS depression, cerebral edema, seizure
- Stage 2 (12-24 hours) = cardiopulmonary stage
- Myocardial dysfunction, shock
- Tachypnea, ARDS
- Stage 3 (24-72 hours) = renal stage
- Renal failure is the primary problem
- Stage 4
- Late neurologic sequelae can occur
methanol
- Stage 1 (0-6 hours) – mimics ethanol intoxication
- Inebriation (dizzy, ataxic, confused)
- Gastric irritation (pain, nausea, vomiting)
- Stage 2 (6-30 hours) – latent phase may occur
- Inebriation resolves
- Can be asymptomatic
- Stage 3 (6-72 hours)
- Visual symptoms (blurred vision, blindness)
- Seizure, coma, cerebral edema, herniation
- Cardiac failure, respiratory arrest can occur
labs to obtain
- Fingerstick glucose
- Electrolytes including Ca/Mg/Phos
- Lactate
- Beta-hydroxybutyrate level
- Acetaminophen & salicylate levels
- Ethanol level
- Creatinine kinase
- Ethylene glycol & methanol levels
- Caution: Many labs have a “volatile alcohols panel” which contains methanol but not ethylene glycol.
- Methemoglobin level (if there is cyanosis following the ingestion of antifreeze, which may contain nitrates).
- More on bedside evaluation for methemoglobinemia here.
Osmolal gap has traditionally been used as a screening test for toxic alcohol ingestion. However, this chapter will argue that it should be abandoned. This is a bit controversial, but there is a considerable amount of evidence that the osmolal gap is unhelpful. Furthermore, many toxicologists have been saying this for a long time. Reasons to stop measuring the osmolal gap are as follows:
theoretical problem #1: no standardization
- There are over thirty different equations in the literature to calculate the osmolal gap! It's unclear which is best.
- There is no consensus about the upper limit of normal of the osmolal gap. Common choices range between 10-20 mOsm.
- Normal ranges of osmolal gap may evolve over time, with different techniques for analyzing electrolyte levels. Likewise, there may be variation between different hospitals.
- The upshot is that there is no standardization regarding whether any given patient has an elevated osmolal gap.
theoretical problem #2: low sensitivity
- The osmolal gap normally ranges over a span of ~ 20 mOsm/L (e.g., from -10 mOsm to +10 mOsm).
- An ethylene glycol level >20 mg/dL is regarded as potentially toxic. That corresponds to an osmolal shift of only 3 mOsm/L.
- If patients start off with a baseline osmolality on the lower end of normal, they could have a clinically significant ethylene glycol intoxication with a normal osmolal gap.
- Additionally, later on in the course of intoxication, the ethylene glycol or methanol will have been metabolized – so the osmolal gap will invariably be absent.
theoretical problem #3: low specificity
- Elevated osmolal gap may be caused by any uncharged molecules in the blood or any non-sodium cations. This may include:
- Toxic alcohols (ethylene glycol, methanol)
- Other alcohols (isopropyl alcohol, mannitol, glycerol, ethanol)
- Ketoacidosis (due to acetone generation)
- Renal failure
- Shock
- Contrast dye, intravenous immunoglobulin
- Hypermagnesemia, hypercalcemia, lithium intoxication
- Pseudohyponatremia (e.g. due to hyperproteinemia or hyperlipidemia)
- Thus, an elevated osmolal gap doesn't prove that the patient has an intoxication with ethylene glycol or methanol.
bottom line: bad test performance

- Available studies of osmolal gap are shown above. No matter which cutoff or equation is used, the test is extremely unreliable.
- Even if the cutoff is made very, very high (30 mOsm), the positive predictive value is still only ~40%.
- The concept of osmolal gap is intellectually appealing, but the data ultimately just don't work.

Over time, the osmolal gap decreases while the anion gap increases. This may make the anion gap more useful than the osmolal gap. The anion gap may be strikingly high.
sensitivity
- Clinically significant poisoning with ethylene glycol or methanol will invariably cause anion gap elevation. The issue is when we can expect to see this elevation in anion gap.
- The relevant pharmacokinetics are as follows:
- Ethylene glycol and methanol are both readily absorbed from the gut (e.g. with peak serum levels occurring ~1 hour after ingestion).
- Ethylene glycol has a half-life of ~3-8 hours, whereas methanol has a half-life of ~2-3 hours. As parent alcohol levels fall, acidic metabolites rise.
- Metabolism may be halted by co-ingestion with ethanol (causing elevation of the anion gap to be delayed).
- Evidentiary support:
- Ethylene Glycol: Jolliff et al. retrospectively analyzed the published literature and found that an acidosis was invariably present by 4 hours after ingestion (provided the patient didn't co-ingest ethanol)(abstract below).
- Methanol: Kostic et al. retrospectively analyzed all published literature and found that an acidosis was almost invariably present by >5 hours after ingestion (provided that the patient wasn't treated early with fomepizole).(14677789)
- This suggests that, overall, serial measurement of anion gap over time should be extremely sensitive to toxic alcohol poisoning. This might be accomplished as follows:
- Anion gap could be measured at baseline and then repeated q2hr-q4hr.
- Exactly how long to follow the anion gap is unclear. Jolliff et al. below suggests that 4-6 hours should generally suffice for ethylene glycol. However, in the presence of ethanol co-ingestion, anion gap should arguably be cycled until 6 hours after the ethanol is metabolized. A recent review suggested cycling the anion gap for 12 hours. (29427181)
- The intensity and duration of anion gap measurement could be adjusted based on clinical scenario and index of suspicion. For example, if the patient had a toxic ingestion >6 hours previously and ethanol levels are negative, then serial anion gap measurements might not be needed at all.

specificity
- Elevated anion gap is certainly not specific for toxic alcohol ingestion, since it may be caused by a myriad of disorders.
- An elevated anion gap should prompt thorough evaluation for alternative etiologies (e.g. including measurement of lactate and ketoacid levels). In the absence of other etiologies, toxic alcohol ingestion may be more likely.
real lactate elevation
- Patients with ethylene glycol or methanol poisoning can have true elevation of their lactate levels, for a variety of reasons:
- Methanol results in formic acid production, which is a mitochondrial poison.
- Patients are often alcoholic, with low thiamine levels.
- Physiologic stress, elevated endogenous epinephrine, and elevated levels of NADH due to alcohol poisoning may all favor lactate production.
- Generally, the level of lactate is fairly low (e.g. <5 mM).
- The degree of lactate elevation is generally too low to fully account for the elevated anion gap (anion gap elevation is due primarily to other anions, such as formate and glyoxylate).
artifactual elevation of “lactate” & the “lactate gap”
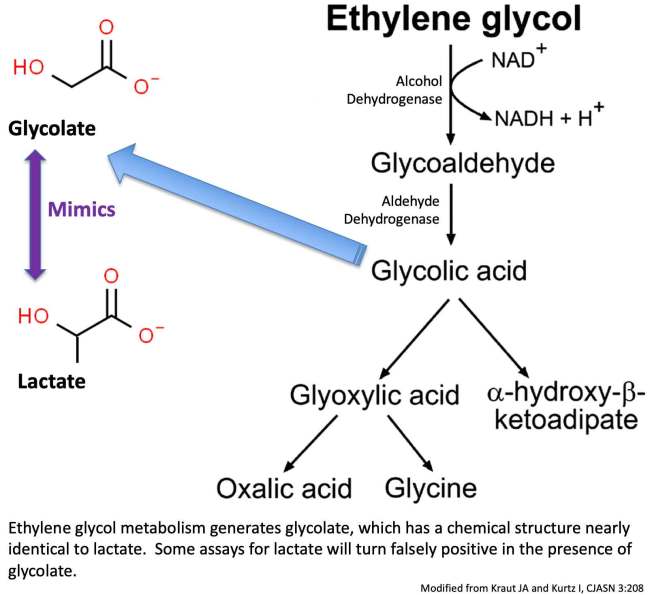
- Ethylene glycol metabolism generates glycolate, which can be mistaken for lactate by portable lab assays utilizing lactate oxidase.
- Lactate gap refers to the difference in lactate measurement via different methods:
- Elevated lactate on portable blood gas machine utilizing lactate oxidase.
- Lower lactate as measured by the laboratory assay utilizing lactate dehydrogenase.
hypocalcemia
- May be seen, but uncommon overall.
calcium oxalate crystals
- Unfortunately, these are neither sensitive nor specific.
- Calcium oxalate crystals in the urine should prompt consideration of ethylene glycol toxicity. However, these crystals shouldn't be used to dictate major management decisions.
direct measurements of ethylene glycol or methanol
- Elevated only early in intoxication.
- Levels > 20 mg/dL are considered potentially toxic (or methanol >6.2 mM or ethylene glycol >3.2 mM)
- This cutoff is probably overly conservative but is a reasonable starting point.
traditional assay uses gas chromatography
- Problems:
- (a) Not widely available.
- (b) Has a relatively long turnaround time (may take time for the machine to warm up).
veterinary medicine assay for ethylene glycol metabolites
- An assay developed for veterinary medicine allows for the rapid detection of ethylene glycol metabolites (including glycolic acid).
- This assay is not widely available currently, although it is being used at some larger centers.
- Limitations:
- i) Since the assay evaluates for the presence of ethylene glycol metabolites, it could be falsely negative very early following ingestion.
- ii) Propylene glycol may cause false-positive results, but this can generally be recognized due to a unique reaction kinetics caused by propylene glycol.(26553280)
methanol (31589567)
- Bilateral basal ganglia necrosis is the most notable feature, which may selectively involve the putamen.
- Hemorrhagic necrosis appears bright on CT imaging.
- MRI shows hyperintensity on T2/FLAIR sequences, with restricted diffusion. Hemorrhage may be especially notable on SWI/GRE sequences.
- Other features which may also occur:
- Subcortical white matter and cerebellar involvement.
- Optic nerve necrosis.


decontamination
- If ingested within the last hour, place an NG tube and suction the stomach.
- There's no need for a large-bore tube: these are liquids.
- In reality, it's unlikely the patient will present this early after ingestion.
- There is no role for charcoal (it doesn't absorb alcohols).
potential indications to start alcohol dehydrogenase blockade
- (1) Empiric initiation if poisoning is strongly suspected, for example:
- Ingestion history (witnessed or reported).
- Markedly elevated anion gap without alternative explanation, in a context consistent with toxic alcohol poisoning.
- (2) If the patient is known to have an ethylene glycol or methanol level >20 mg/dL (or methanol >6.2 mM or ethylene glycol >3.2 mM)
- Generally, waiting for these labs to come back delays therapy excessively – so treatment should be initiated empirically as above.
when to stop alcohol dehydrogenase blockade
- Stop when levels of toxic alcohol are known to be undetectable or at a safe level (<20 mg/dL, or methanol <6.2 mM, or ethylene glycol <3.2 mM)
- Unfortunately, elimination of ethylene glycol or methanol may take a while:
- Ethylene glycol is renally cleared with a half-life of 17 hours (longer in patients with renal insufficiency).
- Methanol is cleared via respiration, with a half-life of ~50 hours!
- In many cases, dialysis may be required to clear parent alcohols and facilitate discharge from the hospital. Alcohol dehydrogenase blockade can be stopped some hours after hemodialysis, once labs confirm that there is no rebound in toxicity.
fomepizole (a.k.a. 4-methylpyrazole)
- Prevents metabolism of ethylene glycol or methanol into toxic acids.
- Safe, but also very expensive (~$1,500 per dose).
- Dosing
- Initial dose 15 mg/kg IV, then
- 10 mg/kg IV Q12 hours for four doses (two days), then
- 15 mg/kg IV Q12 hours
- Fomepizole induces its own metabolism, so the dose needs to be raised over time.
- Increase the dose during hemodialysis to q4hr. If the last dose was >6 hours previously, give an additional dose when initiating dialysis.
ethanol
- Role of ethanol
- Ethanol is generally a second-line therapy, if fomepizole is unavailable.
- Ethanol does have a major advantage compared to fomepizole in terms of cost ($1500 for a dose of fomepizole vs. ~$15 for a six-pack of beer).
- Dosing ethanol may be a bit tricky:
- The target blood alcohol level is 100-150 mg/dL (for comparison, 80 mg/dL is the level at which one is legally drunk and unable to drive in the United States).
- For most patients with a baseline normal mental status, a blood alcohol level of 100-150 mg/dL corresponds with being moderately drunk.
- This is generally done with oral alcohol (as most hospitals don't have IV alcohol).
- Loading Dose
- Loading dose is 0.8 g/kg ethanol in a sober patient.
- The volume of alcohol required is the loading dose divided by the % alcohol by volume (which is half of the “proof”).
- For example, using 80 proof alcohol (40%), this loading dose would equate to 0.8 g/kg divided by 0.4, yielding a dose of 2 ml/kg.
- Maintenance Dose
- Typically, this is ~66-130 mg/kg/hour, but may be higher in patients who drink regularly (e.g. 100-150 mg/kg/hr). This equates to ~7 grams of ethanol per hour, which is equivalent to half of a standard “drink” of alcohol per hour.
- Patients undergoing hemodialysis may have substantially higher maintenance requirements (e.g. 250-350 mg/kg/hr).
- Patients differ in their ability to metabolize alcohol, so titrate to clinical effect and laboratory values.
- Monitoring
- Follow: electrolytes, glucose, and ethanol level q2hr (targeting an ethanol level of 100-150 mg/dL).
- If the anion gap increases, this suggests inadequate blockade of alcohol dehydrogenase.
- Type of alcohol
- Hard alcohol may be better (to avoid vomiting).
- Beer or wine may be more palatable, but a lot more will be needed.
- Potential complications
- Nausea and vomiting.
- Respiratory depression (this must be distinguished from side-effects of the initial intoxication).
- Hypoglycemia.
- Behavioral disturbances, inappropriate telephone calls.
- Pregnancy
- Ethanol is relatively contraindicated in pregnancy (especially in the first trimester), so fomepizole would be preferable here.
- Ethanol may be used as a temporary treatment until alternative therapies are available (e.g. fomepizole or dialysis). Short-term ethanol exposure may be preferable to untreated ethylene glycol or methanol poisoning.
- This is a particularly challenging issue, so toxicology consultation is warranted.
roles of hemodialysis
- (1) Removes the toxic alcohols themselves.
- This may limit the duration of fomepizole therapy required, and thus the hospital length of stay.
- As explored in the last section, clearance of ethylene glycol or methanol is surprisingly sluggish. Compared to extensive hospital stays and repeated doses of fomepizole, a run of hemodialysis may actually be cost-saving.
- (2) Removal of metabolic byproducts of alcohol metabolism (e.g. formate, oxalate, and glycolate).
- This is the most important role of dialysis.
indications for dialysis
- (Consult nephrology early – ideally before the patient is meeting the criteria below.)
- (1) Acidosis
- Metabolic acidosis (pH <7.15)
- Anion gap >24 mM (calculated as Na – Cl – Bicarb)
- (2) End-organ damage, e.g.
- Coma, seizure
- Vision changes
- Renal failure (this may also inhibit clearance of various substances)
- (3) Methanol or ethylene glycol level
- >50 mg/dL in absence of EtOH or fomepizole therapy
- >60 mg/dL in context of ethanol therapy
- >70 mg/dL in context of fomepizole therapy
- Note: Elevated levels of methanol or ethylene glycol is a less urgent indication for hemodialysis if this is an isolated finding (without anion gap elevation or end-organ damage) and alcohol dehydrogenase is adequately blocked. Dialysis isn't mandatory for these patients, but may be useful to accelerate resolution.
- These are based on the EXTRIP guidelines for methanol.
continue alcohol dehydrogenase blockade during dialysis
- Dose adjustment may be required to maintain adequate levels.
- For example, fomepizole needs to be dosed q4hr (see section above).
other technical details
- Intermittent hemodialysis is preferred, to remove toxins rapidly.
- Methanol poisoning may cause coagulopathy, so be careful if anticoagulation is being used to facilitate dialysis.
- Continue dialysis until alcohol level is <20 mg/dL and acidosis resolves. A repeat level may sometimes be obtained two hours after hemodialysis to exclude rebound.
bicarbonate for management of acidosis
- Normalizing pH could keep toxic metabolites in an ionized state (e.g. formate, glycolate). This is beneficial for two reasons:
- (1) Molecules in the ionized state are less able to penetrate tissues (e.g. the brain and retina).
- (2) Molecules in the ionized state pass into the renal tubules, get “trapped” there, and are excreted in urine.
- The therapeutic target should probably be a normal pH (this isn't alkalinizing the blood, but rather merely bringing the pH back to a normal level).
- Details
- (1) Hypertonic bicarbonate may be used initially to rapidly improve the pH (e.g. slowly pushing ampules of bicarbonate). Ongoing use of hypertonic bicarbonate will be limited by its effect of increasing the sodium level. The amount of hypertonic bicarbonate which can be used may depend to a certain extent on the patient's initial sodium level.
- (2) Isotonic bicarbonate may subsequently be required to elevate the pH without inducing hypernatremia. Isotonic bicarbonate may be continued as a maintenance fluid infusion, pending hemodialysis.
- Stabilizing the pH with bicarbonate is not intended as an alternative to hemodialysis, but rather as a bridge to hemodialysis.
- A general concept of the amount of bicarbonate required initially may be obtained by calculating the bicarbonate deficit (using MDCalc). Of course, ongoing alcohol metabolism may generate additional acid.
- More on isotonic versus hypertonic bicarbonate here.
hypocalcemia
- Ethylene glycol may cause hypocalcemia, due to chelation with oxalic acid.
- Avoid giving calcium if possible (this may exacerbate the precipitation of calcium oxalate within tissues).
- Calcium is indicated for tetany, seizures, or substantial QT prolongation.(22998995)
These may facilitate metabolism of toxic acid byproducts. Or they may be harmlessly excreted in the urine.
 for ethylene glycol:
for ethylene glycol:
- Thiamine 100 mg IV daily.
- Pyridoxine (vitamin B6) 100 mg IV twice daily.
for methanol:
- Folinic acid (a.k.a. leucovorin), 50-100 mg IV q4hr.
- If unavailable, folic acid may be used at the same dose.
- Severe methanol poisoning can lead to brain death.
- Brain death should be approached carefully in patients with intoxication, given the possibility of residual intoxicant. Confirmatory tests (e.g. perfusion flow scan) should be considered.
- Methanol-induced brain death is compatible with organ donation, so this should be considered if brain death is diagnosed. (12010136)

Follow us on iTunes
The Podcast Episode
Want to Download the Episode?
Right Click Here and Choose Save-As
To keep this page small and fast, questions & discussion about this post can be found on another page here.

- Avoid giving calcium to patients with ethylene glycol intoxication, as this may exacerbate the precipitation of calcium oxalate in tissues.
- Calcium oxalate stones in the urine aren't highly specific for ethylene glycol intoxication, so their presence isn't necessarily an indication for hemodialysis.
- A “volatile alcohol screen” might not include testing for ethylene glycol, depending on your hospital's lab. An ethylene glycol level may have to be ordered separately.
- Beware of relying on the osmolal gap; a normal osmolal gap doesn't exclude toxic alcohol ingestion.
Guide to emoji hyperlinks 
 = Link to online calculator.
= Link to online calculator. = Link to Medscape monograph about a drug.
= Link to Medscape monograph about a drug. = Link to IBCC section about a drug.
= Link to IBCC section about a drug. = Link to IBCC section covering that topic.
= Link to IBCC section covering that topic. = Link to FOAMed site with related information.
= Link to FOAMed site with related information. = Link to supplemental media.
= Link to supplemental media.
References
- 12010136 López-Navidad A, Caballero F, González-Segura C, Cabrer C, Frutos MA. Short- and long-term success of organs transplanted from acute methanol poisoned donors. Clin Transplant. 2002 Jun;16(3):151-62. doi: 10.1034/j.1399-0012.2002.01109.x [PubMed]
- 22998995 Kruse JA. Methanol and ethylene glycol intoxication. Crit Care Clin. 2012 Oct;28(4):661-711. doi: 10.1016/j.ccc.2012.07.002 [PubMed]
- 26553280 Rooney SL, Ehlers A, Morris C, Drees D, Davis SR, Kulhavy J, Krasowski MD. Use of a Rapid Ethylene Glycol Assay: a 4-Year Retrospective Study at an Academic Medical Center. J Med Toxicol. 2016 Jun;12(2):172-9. doi: 10.1007/s13181-015-0516-6 [PubMed]
- 29427181 Ng PCY, Long BJ, Davis WT, Sessions DJ, Koyfman A. Toxic alcohol diagnosis and management: an emergency medicine review. Intern Emerg Med. 2018 Apr;13(3):375-383. doi: 10.1007/s11739-018-1799-9 [PubMed]
- 31589567 de Oliveira AM, Paulino MV, Vieira APF, McKinney AM, da Rocha AJ, Dos Santos GT, Leite CDC, Godoy LFS, Lucato LT. Imaging Patterns of Toxic and Metabolic Brain Disorders. Radiographics. 2019 Oct;39(6):1672-1695. doi: 10.1148/rg.2019190016 [PubMed]
