Guest Post by Casey Albin, MD (@caseyalbin)
Spend any time in the NeuroICU and you will encounter an abundance of ADH.
1️⃣Pt in Diabetes Insipidus. Give anti-diuretic hormone (ADH), call it “pit drip”
2️⃣Pt in distributive shock. Give ADH, call it “vaso”
3️⃣Pt on ASA needs EVD (external ventricular drain). Give ADH (sort of), call it “DDAVP”
4️⃣Fellow postcall & confused, give….

Kidding. Obviously give Starbucks.
Understanding the various names and purposes of ADH is exhausting and confusing, thus, a post to review all things ADH including:
✅ It’s various aliases
✅ Receptors and function
✅ It’s clinical utility, particularly in the NeuroICU.
Part I: The Aliases
Anti-diuretic hormone, desmopressin, DDAVP, vasopressin, AVP, Pitressin, Vasostrict – are they really all the same?
Not quite.
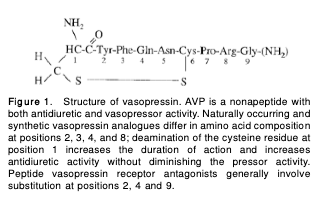
Anti-diuretic hormone (ADH) and arginine vasopressin (AVP) can be used interchangeably for the neurohypophyseal hormone secreted by the posterior pituitary.
In practice these are referred to as either:
 Pitressin® (“pit drip”) = trade name of a synthetic vasopressin solution. Can be made for IV, IM, SC or even intranasal
Pitressin® (“pit drip”) = trade name of a synthetic vasopressin solution. Can be made for IV, IM, SC or even intranasal
Vasostrict® (“vaso”) = trade name of another synthetic vasopressin solution, IV.
Both: 1mL = 20 units vasopressin.
Usually reconstituted to a concentration of 0.1unit/mL.
 In contrast, desmopressin acetate is a synthetic analogue of ADH. Desmopressin is formulated with D-arginine for L-arginine at position 8; position 1 is deaminated.
In contrast, desmopressin acetate is a synthetic analogue of ADH. Desmopressin is formulated with D-arginine for L-arginine at position 8; position 1 is deaminated.
DDAVP ® is a trade name.
The consequence of this small structural tweak is that DDAVP has ⬇️ vasopressor activity but ⬆️ antidiuretic action.
Part 2: Preventing Water Loss

How does ADH prevent diuresis?
⚡️Plasma osmolarity (>280 mOsm)
⚡️Hypotension
⚡️Hypovolemia
all trigger release of ADH.
As can (often inappropriately)
⚡️Nausea
⚡️Pain
⚡️Organic neuropathology
(Resulting in that pesky syndrome… SIADH😲)
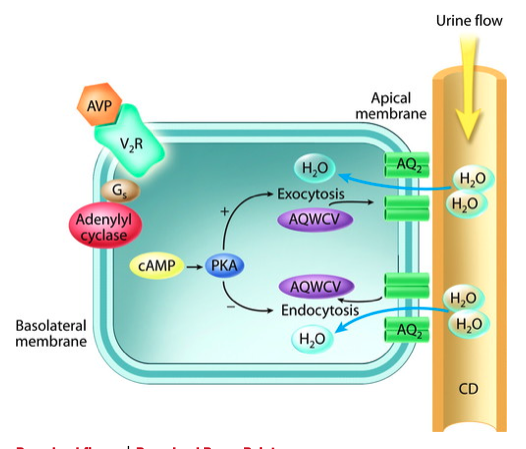
ADH (AVP) then binds to V2️⃣receptors in the principal cells of the kidney collecting system. Binding to V2️⃣ receptors increases water and urea permeability which leads to ⬆️ water reabsorption.
(You can remember that V2️⃣ receptors increase H2️⃣O retention.)
Note that while AVP and DDAVP both bind here, DDAVP has a much stronger affinity to these receptors.
In the NeuroICU, the primary use for ADH in this context is to treat central DI resulting after a transsphenoidal adenomectomy (TSA) or cerebral herniation.
In cerebral herniation the pituitary stalk is compression while during a TSA the pituitary stalk may be severed, injured, or manipulated. The result is that ADH can no longer be secreted and consequentially, the kidneys allow massive pure water loss. This can cause rapid progression to hypovolemic shock and profound hypernatremia if not quickly corrected.
The solution is to give ADH back. In this situation an ADH bolus and gtt (as either a “Vaso” or “Pit” gtt, same thing, different brand name) are usually the initial choice for treatment of DI as these are more easily titrated than DDAVP.
⚡️An IV dose of Vaso/Pit 2.5-5 units can be given to temporize the water loss while waiting for the gtt.
⚡️Then titrate a gtt to Vaso/Pit 0.25-1 unit/hour. This is titrated to Uosm, UOP, and serum sodium.
Dose finding mandates incredibly close monitoring! Checking Uosm Q4 is a quick way to insure than ADH is still “on”, as demonstrated by Uosm >200. The goal is to have the patient in a euvolemic state where their ins match outs. If they cannot keep up with the water losses (or if you are having to replace >~500 Q2H for comatose patients), they need a larger vasopressin dose. If they aren’t peeing at all, the dose is too high. The urine output is a great indicator of how you are currently doing, while the serum sodium is reflective of how you have done.
Long term, if needed, DI is managed with desmopressin (DDAVP) which can be given or PO, intranasally or subQ. As a PO drug, its absorption can be unpredictable and finding the right dose requires some trial and a lot of monitoring.
⚡️PO doses range from 0.1mg qHS to 0.3mg TID.
Totally counterintuitively ADH can also be used to regulate the correction of Na+ in chronically hypovolemic hyponatremic patients. If that seems incredibly ludicrous (…why would we give a patient with low sodium a water retention drug??) see: Taking Control of Severe Hyponatremia

Part 3: Causing Vasoconstriction
How does ADH result in vasoconstriction?
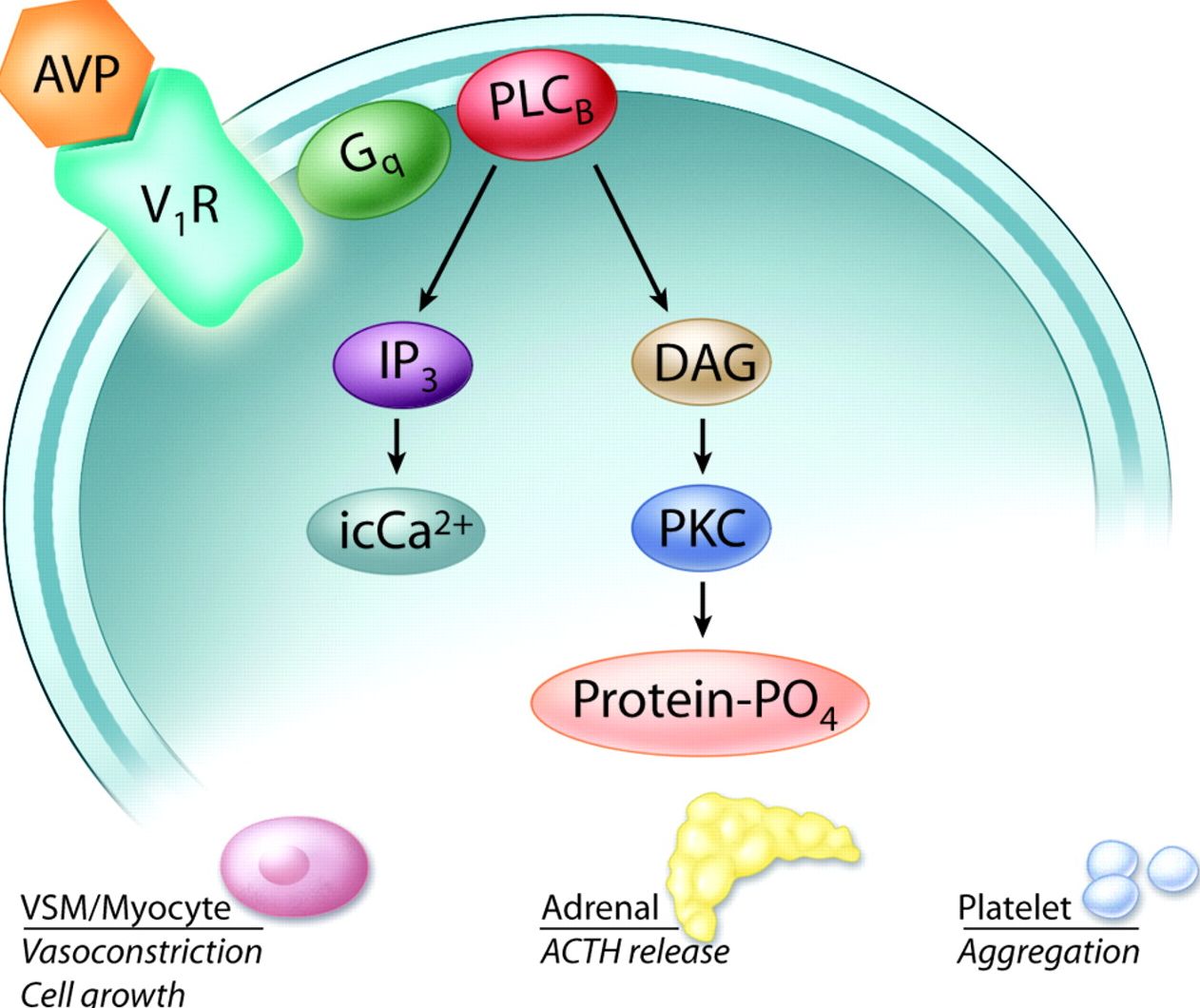
This is mediated by binding of ADH (AVP) to V1️⃣ receptors located in smooth muscles which triggers catecholamine-independent vasoconstriction.

Doses here are fixed at either vasopressin 0.03 or 0.04 units/*min* (1.8-2.4 units/hour).
Remember, the DI dose of vasopressin is 0.5-1 unit/hour… (I remember initially thinking that they were orders of magnitude different, but because of the time denominator, the shock dose is ~2-5x larger.)
For more about the use of vasopressin as a vasopressor in management of septic shock, see IBCC Sepsis

Part 4: Platelet Booster
Perhaps most interestingly, both vasopressin and desmopressin/DDAVP have intrinsic platelet activating properties, but DDAVP has the added effect of releasing von Willebrand Factor & Factor VIII from endothelial cells by increasing platelet activating factor.
Since the 1970s desmopressin it has been used to prevent bleeding in patients with von Willebrand Factor deficiency and hemophilia A
The bleeding dose is a one-time IV Desmopressin 0.3-0.4mcg/kg (so around 20-30mcg). For comparison, the anti-diuretic dose is DDAVP 1-2 mcg IV. The hemostasis dose is thus x10 higher. Effect is maximal in ~30 mins.
Why does this matter in the neuroICU? Because quite commonly have patients on anti-platelet meds who then develop an ICU. The PATCH trial (PMID: 27178479) demonstrated worse outcomes in patients who received platelet transfusion to “reverse” ASA’s effect. The odds of death or dependence where higher in the plt transfusion group, with higher rates of serious adverse events in this group as well.
Given DDAVP’s platelet activating effect, could this an effective alternative?
 Maybe… kind of.
Maybe… kind of.
- Effect of Desmopressin on Platelet Dysfunction During Antiplatelet Therapy: A Systematic Review (PMID: 32748210)
- Early Administration of Desmopressin and Platelet Transfusion for Reducing Hematoma Expansion in Patients With Acute Antiplatelet Therapy Associated with Intracerebral hemorrhage (PMID: 32304415)
Hopefully, the DASH randomized trial will sort this out further (PMID: 33172941)
➡️➡️➡️
What comes up even more frequently is when a patient presents with IPH/IVH or SAH and needs an EVD but was on antiplatelet therapy. Can DDAVP be used in those cases to transiently upregulate von Willebrand factor and promote platelet adhesion to limit tract-related hemorrhage?
The short answer is we don’t know.
Below: a patient’s platelet function assay on ASA + ticagrelor before DDAVP (timestamp 12:36–no value, comment only) and then 90 mins after DDAVP was given (time stamp 15:31), which shows near normalization of the platelet function assay with DDAVP – a transient effect.

Comment:
![]()
There is a paucity of data about this, but likely a reasonable strategy in an emergent situation.

In Summary


- NeuroEMCrit – 31 #NeuroPostItPearls - August 22, 2022
- NeuroEMCrit – IVIG 🆚 PLEX - May 3, 2022
- NeuroEMCrit – Does Vent Over-Breathing Always Disqualify Brain Death Testing? - December 27, 2021
Dr. Albin, nice summary post even for experienced docs like me!
One comment: while the content is 100/100, the numbering of the sections and numbering the Starbucks joke made me have to make a table for myself just to compare and contrast. Perhaps a robust summary like Josh’s bullet at the end would hammer your points home?
One piece of trivia: there have been a few drug errors confusion PITOCIN and PITRESSIN in past … different but related drugs for very different conditions!
One question: for DI when would you recommend vasopressin infusion, DDAVP prn and DDAVP scheduled?
Thanks! Anant
Hey Anant, great suggestion! Yes, our fellow told me that when he heard us say you can start a “pit drip” he did a double take, “like am I back on OB?” ha! In DI I almost always start with vasopressin infusion, as our patients are initially not cognitively stable enough to reliably drink to thirst. In the post op patient, I usually will use vasopressin for a day or two and get a sense of their requirements before transitioning to DDAVP, then I do a scheduled DDAVP dose in the AM and watch them incredibly closely especially around the… Read more »