Today, an update on Push-Dose Pressors. I coined the name Push-Dose Pressors (PDPs) way back on episode 6. The idea was not new, anesthesiologists and resus docs have been using bolus-dose vasopressors for decades. I just thought the name was dumb, these are not boluses in the way I have always thought of them (a brief iv drip). I also thought it was crazy that the concept had not really penetrated very far into emergency medicine and the ICU–at least in the States. My prehospital doc friends told me it was common in their world. Since the podcast, I have received 100s of emails describing the use of PDPs to lifesaving effect (or at least code-preventing), but there has been scant published literature on this technique in EM. Recently that has all changed.
Can We Wait for the Drip?
Resus-Ready EDs should be able to get a vasopressor drip up within 8 minutes (completely made-up number, just like most hospital certification standards)
Dead Space in the Lines
What should you do when you can't wait that long?
How do you treat critically low perfusion to the heart & brain?
Push-Dose Pressors Fill the Gap
Especially in the Peri-Intubation, when patients have an annoying habit of popping into cardiac arrest
ED Pharmacists Discussion of Medication Safety for Push-Dose Pressors
Safety Guidelines for Push Dose Pressors
While there seems to be a slightly negative bias against docs' capability to mix drugs and a pro-pharmD bias (understandable), the messages from this article as a whole were fantastic. Here are some alterations/things to be aware of that I discuss in the podcast:
- The Prohibition against Pre-Filled Saline Syringes
- The Phenylephrine Chart
An Editorial on the Above Article
Cole Editorial on Push-Dose Pressors
Why EPI has won my Heart
Sorry Phenyl you were but a brief fling
Push-Dose Epi Labels
Inspired by the Danny the Medic
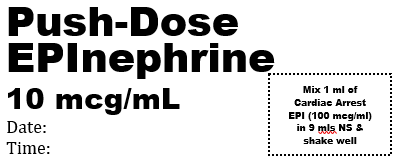
Cardiac Arrest EPI Syringe
0.5 mls of the cardiac arrest epi is an ok stopgap
Dirty Epi Drip
I do not recommend the dirty epi drip. Please, please understand how this makes our specialty look
For the love of all this is Resus, Label the frackin bag!
This is not the time to have something going on in the background that you are paying no attention to
Push-Dose Norepi if you Just Never Want to Deal with Mixing
Check your premixed concentration: If you have the 4mg in 250 ml (16 mcg/ml) you can give 0.5 to 1 ml per minute
Pick One Way to Go in your ED
Otherwise errors are more likely
ED Pharmacists in General
Love having ED PharmDs as part of the team! Are there downsides?
Premixed Push-Dose Epi

Other Lit Mentioned
- The impact of push-dose phenylephrine use on subsequent preload expansion in the ED setting. The American Journal of Emergency Medicine Volume 34, Issue 12, December 2016, Pages 2419–2422
- This study compares push-dose phenylephrine to continuous infusion–no difference between the two (Anesthesia Analgesia 21012;115(6):1343)
- First article in the ED demonstrates efficacy on blood pressure (The Journal of Emergency Medicine Volume 49, Issue 4, October 2015, Pages 488–494)
- Acquisto NM et al. Medication Errors with Push Dose Pressors in the Emergency Department and Intensive Care Units (AJEM In Press)
- Push Dose in CCT
Update
- Some of my favorite EM PharmDs have responded to the Acquisto letter to the editor
- Push-Dose NorEpi
- Two More RCTS: 38476203 & 38264276
- Braude's group published safety data on phenylephrine1
- Epi doesn't seem to raise HR–no more phenyl [Am J EMerg Med 2022;52:43]
- Safety and Efficacy of Phenyl and Epi [Am J Emerg Med 2022;61:137-142]
Additional New Information
More on EMCrit
Additional Resources
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Have never understood why we don’t tend to use push-dose norepi. Any idea?
same reason I like epi better than phenyl–I want a lot of inotropy
But why does the entire idea of bolusing Levo seem so alien in the US? Is there some concern for harm?
I use push norepi all the time. In most patients I don’t think it matters much and I’m mainly giving pressors for alpha activity. In many hospitals including mine, anesthesia uses push norepi routinely.
Could make the argument that compared with epi/neo, norepi may pose a higher risk if it extravasates while your giving bolus doses through a peripheral line?
https://emcrit.org/pulmcrit/phenylephrine-epinephrine-central-access/
Wonder if that’s why — although hard to imagine it would be worse (i.e. more vasoconstrictive at our doses) than epi!
In a patient who has a compensatory tachycardia (lets say 130-140), Epi has more chonotropy which we don’t necessarily want, so then why isn’t push dose levo standard? We use levo as our first line pressor for most hypotensive situations with few exceptions. I understand desire for inotropy, but levo also has intropy without much chonotropy. in relation to epi. My question really boils down to this: if all of our pressers work almost instantly, and levo is our first line drip, then why is it not our first line push-dose? Also it makes the logistics easier because you already… Read more »
Phil
did you listen to the podcast????????????????????????
I asked the same thing about levophed Brandon. Seems like something that just hasn’t been discussed much. Especially in EMS where neo isn’t an option.
I just wanted to comment on why I think drawing up into the saline flushes is not recommended. It may be due to sterility, but more likely it’s due to the safety issue of the syringe not being labeled or the label falling offf and now someone thinks they are giving a saline flush but are actually giving a medication.
https://www.ismp.org/newsletters/acutecare/articles/20061116_2.asp
would only be a problem in unlabeled syringes–push dose pressors should ALWAYS be labeled. Hope this is not the study author’s rationale, but still great find
The issue of the syringes isn’t labeling. It’s a technicality the FDA identified:
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/detail.cfm?mdrfoi__id=2501052
The saline flush syringes are used to mix and prepare medications and they are technically a “medical device” and should not be used to reconstitute medication.
Use a fresh syringe and you’ll always be safe.
Thanks! that explains the why.
i can’t for the life of me understand what the FDA/IMSP’s issues are–that paragraph made no sense. If the saline flush is labelled, I see no difference in safety between this and a 10ml syringe
In a perfect world I agree with you. But it’s not a perfect world.. Lables come off, I’ve seen sharpies get smeared. I’ts an error waiting to happen and it has. In my risk manager days and as a Legal consultant I’ve seen cases here lables have come off and people were given mixed paralytic thinking that it was just a flush. ALso in a perfect world we all would have laminar flow hoods to mix meds in. In reality it’s not that much harder to mix in a plane 10cc syringe and the actual infection risk although isn’t zero,… Read more »
ok–that makes a lot of sense. I will say that the labels we use cannot come off–they are those kinds that require breaking your thumbnail to remove, but I hear you. But this is assuming that people are less likely to screw up with an unlabelled 10ml syringe rather than an unlabelled saline flush, which I kind of buy.
Doctors…One way to make sure you are administering the desired dose of “dirty epi” would be to use a buretrol. There will likely be one in every pediatric code kit. It will eliminate the need to repeatedly draw up epi from the “dirty epi” bag, and eliminate any problems with contamination, assuming you set up the bag and buretrol correctly in the first place, which is easy. Want 10 mcg – put 10 ml into the buretrol and set your drip rate from the chamber below to empty the buretrol in 1 minute. Want 15 -put in 15, etc. Buretrols… Read more »
that actually is a pretty great idea; but it still baffles me why they don’t just put this drip on a pump
In my mind dirty epi drip to be used within limited resources situation; i.e. back of an ambulance, no pump available, busy caregivers allocated to other tasks (i.e. bagging, etc). For transfers with precarious patients I always bring a set of push dose pressors in my pocket. Sure we like to free our mind from as many tasks as possible by putting the patient on a drip though…
My understanding for using a “dirty epi” gtt was for a coding patient. With limited resources the every 3-5 min epi dose administrations are offloaded from the caregivers. Granted this isn’t ACLS but some providers are going to an epi gtt at 0.7 mcg/kg/min during a code for constant state of drug vs the yo yo effect. Ultimately the pt will get a liter and no more than a regular push of 1 mg.
I just retired from the Army where I was a medic. I now work as a contract medic overseas. I have generally worked in austere conditions where pumps were not an option. In fact, I have never used a pump. It’s not that I have anything against pumps. I just have never had one. That brings up an interesting point. I totally agree with your point about not having PharmDs mix drugs instead of nurses or doctors. If they are the sole providers of the service then you have introduced a single point of failure into the system and that… Read more »
Just an an additional observation on your comment that most RNs and MDs aren’t too concerned about reusing a syringe plunger – agitated saline injections during a bubble study effectively require rescuing syringe plungers. In any case, as you had suggested in the podcast, this, in of itself, is not likely to really harm your patient .
another great point!
What are your thoughts for push dose epi for the super sick asthmatic who you don’t want to intubate. I am not talking about the patient who is already tired, altered, acidotic, and you have no choice but to intubate. My question is for the sick asthmatic who over the next 5-10 minutes will probably need to be intubated unless you throw the kitchen sink (cont nebs, steroids, mag, NIPPV, etc). Epi would help, but takes time to get the gtt. Thank you so much for this update, it was very helpful
i think it is fine. thing is that the asthmatic, unlike severe anaphylaxis, has no perfusion deficits so IM would probably be fine in these patients.
Great episode. Lots of pearls, and I agree wholeheartedly with the bit towards the end about the potential for teaching and “upskilling” that ED Clinical Pharmacists could play — something to think about when I’m on my ED Pharmacy elective later this year. I hope you get Dr. Cole on the show sometime soon — he and the crew at Hennepin have been doing a great job continuing to set the bar for clinical research in emergency medicine, and I have no doubt that they’re working on trying to answer some of the questions he poses as the end of… Read more »
yep noticed the same regarding the formatting, but I think that was the problem with the postscript conversion. I’ll put up a better copy asap
I’ve been intrigued with the idea of push-dose pressors for awhile, and in thought they seem to have a certain ease of use. In the prehospital world we would need to have standing orders for these, or have online medical direction for it’s use. You seem to hint in your podcast that these medications should only be handled by the highest level of practitioner. Does this mean you don’t believe this to be an appropriate prehospital tool?
in EMS world, I think if you RSI you should be able to PDP
Dr. Weingart makes a very valid point about compounding, especially since there isn’t round the clock coverage. Often times, mixing up emergency meds gives us a platform to make recommendations or identify issues before the drugs are given. For example, many premixed & compounded medications are intentionally kept in the ED pharmacy to ensure proper use/dosing. I fear that accepting routine non-pharmacy compounding creates a culture of independence over collaboration. This may cut pharmacy out of the whole equation. Most hospitals justify funding for unit based pharmacies with the amount of orders filled, not the amount of drug information provided… Read more »
thanks for these comments!
excellent as always
Given the extremely effective, and surprisingly rapid, results with IM epinephrine in anaphylactic shock, had there been any consideration in it’s use for other vasodilatory shock states?
just the opposite. many of us feel small IV epi doses would be a much better way to go for anaphylaxis
Dr. Weingart…Regarding your comment “just the opposite. many of us feel small IV epi doses would be a much better way to go for anaphylaxis”, would you likely give a standard 0.3 mg IM dose immediately while getting the IV line established, and to deal with the pt initially, then give the smaller IV doses? I had a call on my last shift to a clinic (still a 911 call rather than interfacility) where there was no IV line which I quickly established, but while getting it ready and in I had to stop and give 0.3 mg IM (remember… Read more »
when i had to do drips without pumps on the bus, it always struck me as one of the worst medical practices out there. dirty epi is just a recapitulation of that. push-dose at lease lets you know what you are doing.
i’d always give the IM dose while waiting to get an IV
My colleagues and I recently published this paper in JAMA pediatrics that addresses the accuracy of pushing small doses of epi from the prefilled cardiac syringes. We were considering this for pediatric cardiac arrest scenarios but the findings are applicable here. Bottom line: when you try to push 0.5 mL or 1 mL of epi from a code cart sryinge, much more actually comes out. If you want to be as accurate as possible, you will need to transfer the epi using a 1 mL syringe. http://jamanetwork.com/journals/jamapediatrics/fullarticle/2604748
yep saw it when it first came out. it was great stuff. your variances of error are just fine for my adults given the circumstance we are talking about, i.e. about to code, no time to mix PDP.
Very interesting, on many different levels. First off, thanks to Scott as recognising PharmD’s as more than just extremely expensive typists/human dispensing machines. I wish that more hospital administrators were on the same page. It is sad that as PharmDs , we still have to fight for our identity as clinicians in many hospital systems. Secondly, as to the mixing of drugs in an ED/ICU, I feel that much of this could be minimized by having sticks/drips of epi or whatever already right there when you need them ( pre-made in the pharmacy under an IV hood ), and throwing… Read more »
Cary–as to your specialist analogy. Mixing up TPA and Kcentra has to be the job of the specialist known as the ED RN or MD unless there is somebody else available 24/7/365.
Trudat Scott.
And that’s why at adequately staffed hospitals, like mine, you will have pharmacists there 24/7/365, not just to simply mix up the drug, but to help decide which drug to mix and how much to give.
What does floating a pacer have to do with diluting and pushing epinephrine? Whether you do it all the time or not, in the ED the ED physician should prepare to manage emergencies that don’t happen often. Anything that walks through the door, right. I have used pushed dose epi successfully, not because I use it all the time, but because I am mentally prepared to use it in the appropriate situation. Additionally, I am the physician; pharmacists don’t resuscite patients. They can make their recommendations, but they are not clinicians and don’t bear the responsibility of managing acutely life… Read more »
Agree here wrt relevance of floating a pacer- not sure how diluting a solution by 10 is similar? Seems to Be a lot of discussion over essentially, diluting something by 10. Big adrenaline little adrenaline that’s how I was taught well over 15yes ago in Bristol, UK. In my mind big 1:100 000 I use for bridging sepsis plus others and 1:10 000 for anaphylaxis. Giving one ml every 5 mins of ‘big’ equates to starting your sepsis inoptrope at the lower dosing scale 0.01mcg/kg/min (in average adult). In Aus tendency is for 6mg in 100ml so the “60s” cancel… Read more »
Scott, Thank you for featuring my article on your podcast. It is always rewarding as an author when your work is read. As usual, I enjoyed the podcast, and I agree with the vast majority of what you said. Your point about time to infusion preparation is important. When discussing push-dose pressors at our hospital and bridging to drips, it’s interesting that our consensus was the same as yours; 5 minutes is what to expect for a drip. This window is a difficult period to manage, and I agree there are patients that need a bridge therapy to a drip;… Read more »
Great podcast! I agree with you on most points, however I do not believe pharmacy should take a backseat when mixing meds. Having pharmacists that mix meds (even when they’re only part time) increases both medication safety and efficiency. This is not to say that pharmacists are any faster than nurses/doctors at mixing meds–only that those roles have other tasks to perform in an emergent situation. It seems entirely inefficient to take an additional member of the response team out of the equation to mix meds when a pharmacist alone is capable of doing so.
Scott, completely agree with your comments regarding PharmD mixing meds vs MDs/RNs. I’m a former military ED/ICU RN that has worked in many different civilian facilities all across the country as well as doing critical care flight in the military. The last several places i worked we mixed most of own stuff in emergent or urgent situations and used a readily available protocol flip book for concentrations/compatibility etc. We did have a critical care PharmD but they were only there for supervision/consultation or as a liaison to the main pharmacy and they were not there overnight. It was expected that… Read more »
have noted the exact same situation!!
Push-Dose Pressors are likely here to stay. We have been purchasing and using only pre-mixed Phenylephrine 100 mcg/mL and Epinephrine 10 mcg/mL syringes from a company called Pharmedium for the past year or so. Anesthesia had already been using premixed phenylephrine and ephedrine. The premix eliminates some of the risk of error, concentration inconsistencies, and sterility issues as well as featuring extended expiration dating so they can be loaded in automated dispensing cabinets. I would attach a picture but I’m not sure it’s possible. You can search images online. To our Administration, it was worth the extra cost to not… Read more »
fantastic! I’ve been looking for a compunder that will do push-dose epi.
Hey Scott thanks for the great FOAMed/podcast as always! What is your position on pressors for the acute hemorrhage patient that is severely unstable and actively dying on you? I didn’t see this patient population mentioned in this podcast. I haven’t found any evidence that supports/benefits pressor use before blood product replacement in this patient population and there may definitely be harm. There are providers that do support this though. Thoughts?
Yup, a question that has run through my mind many a time. It will get its own podcast v. soon.
Okay thanks looking forward to it.
I have used PDPs for some years, but starting in transport medicine. I advocate drawing 2ml 1:10,000 adrenaline into a 20ml syringe and filling with 18ml 0.9% saline. This is specifically to give a visual and tactile (useful in a dark helicopter) cue that you have a very different beast to your 10ml syringe of cardiac arrest adrenaline. Thus I know that in my resus room, adrenaline in a 1ml or 3ml syringe is 1:1000 for IM use, adrenaline in a 10ml syringe is 1:10,000 for IV use in cardiac arrest, and adrenaline in a 20ml syringe is 1:100,000 for… Read more »
super cool lecture, scott
thanks
tom
Great podcast over push dose pressors, but one question I do have is that i do not believe I have ever heard you mention anything about the use of volume expanders such as albumin in any if the past pressor related podcasts. I agree that pts do not always need a ton of fluid but is the use of this class of drug effective in the emergent setting?
it is kind of an evidence-free zone. i do use albumin sometimes, esp. in my cirrhotics, but that may be the only pt group where there is some reasonable proof.
Great podcast. In the prehospital environment without blood available, can push dose pressors be used to raise MAP in hypotensive trauma patients for intubation?
yes–one of the best uses
I wonder if you could elaborate on your reasoning for physicians who use push-dose pressors should be able to place transvenous pacers. If you imagine the scenario of many rural and remote emergency departments around the world, the physicians working there will frequently be in a situation to need to manage hypotension/critical hypo perfusion rapidly and alone (i.e. without anesthesia/critical care/any specialist support on the ground). These are also the very same places in which it is difficult to get a vasopressor infusion set up in 5 minutes (i.e. imagine having only two RNs working in the entire ED and… Read more »
FWIW we have manufacturer pre-made epinephrine 10 mcg/ml and phenyephrine 100 mcg/ml syringes at our shop. No mixing required 🙂
I enjoy your podcasts and there is, as they say here I australia, “heaps” of learning moments packed into each one. I’m genuinely curious too know if you see the irony in calling out the potential bias of a research piece because it’s all pharmacy D’s with only one MD. It immediately made me think about the massive majority of research that is entirely authored by MDs. This also made me think of the number of times research has shown nurses can do something as well as or better than certain medical doctors but the recommendations seemed to mismatch the… Read more »
Don’t expect a response, this post is two years old. We are in COVID and I had a hypotensive probable COVID pt that we asked IV levophed. prior to hospital arrival. Still Had to wait and would have been ideal for push dose EPI pending the start of Levo.
THE PT HAD JUST HAD HYDRALIZINE at the nursing home!!! Bp was 48/28. Crazy that this was the same patient you described. Patient was COVID positive and C diff (+). Did well. Still not clear why the NH gave hydralizine. Keep up the good work!
First of all, thank you for providing the best evidence based podcasts in EMCrit! I just wanted to echo your stand on PharmD’s in the ED supervising the processes not doing them if they aren’t there 24/7. As an MD, PharmD I completely agree. We are looking to add a PharmD (other than me) in the ED, and I will certainly emphasize this concept in planning.
I am a clinical nurse educator and PALS/ACLS instructor. Today during a simulation at a rural ER, a physician said they would use a dirty epi infusion FOR A PEDS PT!! NOne of the staff had even heard of it and during the de-brief I suggested that this was not appropriate due to the safety risks you have shared in your podcast. Thank you for continuing to speak about the risks that something like a dirty epi infusion bring to the critical care environment. Preach on!
Has Lidocaine 1% w/ Epi ever been considered? It would have the 1:100,000 desired epi concentration (10ug/mL) and only Lido 10mg/mL. Although Lido has hypotension listed as a side effect, has this been experienced with such a small dose? This would eliminate the mixing and labeling issues.
Thanks Scott. In the earlier podcast you mentioned push dose phenylephrine for the hypotensive patient with arrhythmia that you were about to cardiovert to make the shock more effective. What would you use now?