
 Today, we discuss the PROPPR Trial with its lead author, John Holcomb, MD. This was an RCT of trauma patients with severe hemorrhage. It pitted 1:1:1 matched product transfusion with a 1:1:2 control group. Dr. Holcomb is a Trauma Surgeon at University of Texas, Houston. He spent decades in the military as a surgeon before continuing his career in Houston.
Today, we discuss the PROPPR Trial with its lead author, John Holcomb, MD. This was an RCT of trauma patients with severe hemorrhage. It pitted 1:1:1 matched product transfusion with a 1:1:2 control group. Dr. Holcomb is a Trauma Surgeon at University of Texas, Houston. He spent decades in the military as a surgeon before continuing his career in Houston.
This podcast is coming out a week early, but it is too good to wait!
The Study
Study Summary
As per their routine, the Bottom Line Review summarized the study beautifully
Questions I discussed with Dr. Holcomb
- If you had to give the elevator pitch for the take-home message of the trial, what would it be?
- The doubters may say that the control group in the study should have been 1:3 (plasma:rbc) or even no fixed ratio, but solely an INR/Plt lab based approach. They may say that PROPPR shows 1:1:1 is as good as or better than 1:1:2, but may not be better than a much lower rate of plasma and PLT transfusion. What do you say to this line of commentary?
- The trigger for massive transfusion in the PROPPR trial was ABC>=2 or clinician judgment. Do you bother with scores in your personal practice? Should we be using them?
- In the 1:1:1 group, platelets were given up front (0 unit mark). In the 1:1:2 group, they were only given after 9 units of product. What was the rationale for this? Do you think it might have made a difference?
- It seems the 1:1:2 group played catch up for plasma over the next 24 hours. Do you think this supports the contention that early 1:1:1 may spare the need for products down the road, especially in light of the fact that exsanguination deaths were an early phenomenon.
- Median RBCs were 9 units over 24 hours, which means over half of the patients did not receive the 10 units of RBC that traditionally define Massive Transfusion. Should we redefine MT? What is the point at which it was beneficial to have matched plasma/plt to RBCs.
- This trial was not designed to look at this question, but I want to know what you think. In 2015, should we be using the empiric ratios of the PROPPR trial or should we be switching to a visco-elastic (TEG/TEM) based strategy?
- Let’s do some rapid fire… Aside from the randomized intervention, the trial was pragmatic, so I would love to hear your personal feelings and practice on:
*BP goal
*TXA
*Cryoprecipitate
*Crystalloids - Most studies have a back story—something all of the researchers know, but is not reflected in the word-trimmed, published version. What are we not seeing in the published form of the PROPPR study?
Some key points from the discussion
- Our current definitions of massive transfusion are outdated. Better may be the Critical Administration Threshold–if you give 3 units of blood in any 1 hour period, it is a massive transfusion. But…
- Dr. Holcomb doesn't wait for the 3 unit threshold. At his shop, they try to make the 1st unit transfused plasma or platelets and start matched transfusion from that point forward.
- In the PROPPR trial, only about 2/3 of the patients received TXA, but CRASH2 indications would have had all of them receive it. Dr. Holcomb uses TEG to decide, and wants to see more RCTS (they are being done) to better clarify the role of TXA. For more on that though, see my podcasts with Tim Fabian and Karim Brohi. Vicoelastic tests may be insensitive to fibrinolysis based on these discussions.
- The Kaplan-Meier curves for a 3 hour endpoint showed a statistically significant mortality difference between the two groups, but this was not one of the allowed primary outcomes.
Articles Mentioned in Dr. Holcomb's Discussion
- PROMMTT Trial: Holcomb JB, et al; PROMMTT Study Group. The Prospective, Observational, Multicenter, Major Trauma Transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. (JAMA Surg. 2013;148(2):127-136)
- How I Do It (Blood. 2014;124(20):3052-3058) – Describes how Dr. Holcomb actually practices in his shop
- ABC Score
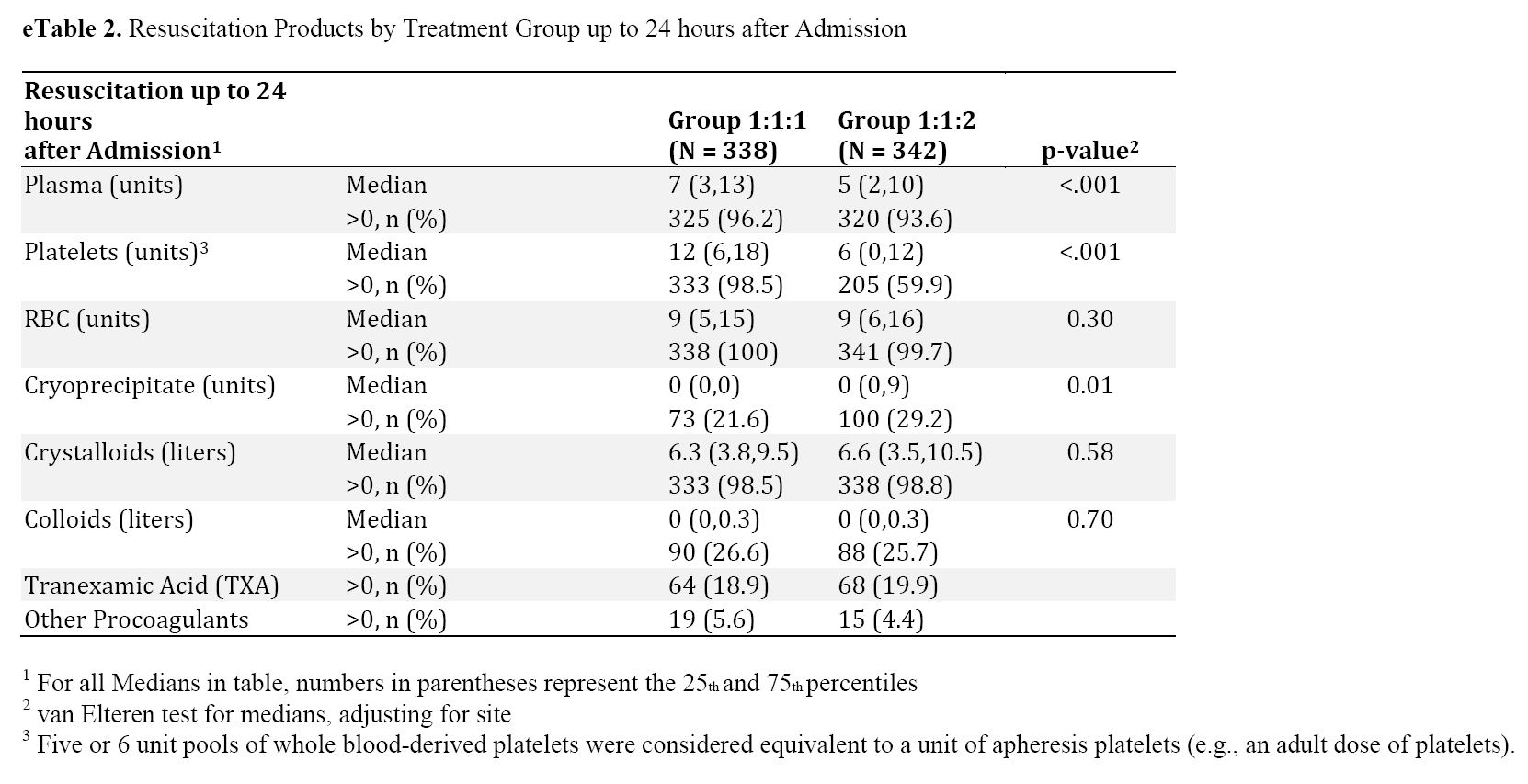
What did the two groups receive in the first 24 hours?
What are others saying?
- Rory Spiegel at EM Nerd: The Adventure of the Blanched Soldier
- Ryan Radecki at EM Literature of Note: The Fixed-Ratio Massive Transfusion Answer
- Salim Rezaie at REBEL EM. The PROPPR Randomized Clinical Trial
- St. Emlyn's Journal Club
Additional New Information
More on EMCrit
EMCrit 197 – The Logistics of the Administration of Massive Transfusion(Opens in a new browser tab)
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Editor-in-Chief, at EMCrit.org
An ED Intensivist from NY.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
Professor
Nassau University Medical Center
No conflicts of interest (coi).
Latest posts by Scott Weingart, MD FCCM (see all)
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
Scott,
I am way behind in my FOAMed consumption. But just looking at the tables it looks like the 1;1:1 group was closer to 1:2:1. Not sure what that means, but interesting signal?
Scott, thanks much for asking the question about trauma resuscitation using crystalloids. I am constantly telling my staff about the recommendations for its use pre-hospital and this podcast helps. Thanks again
I work at a level 1 trauma center but I also moonlight at a community hospital (not a trauma center). At most community hospitals, you can probably get the patient transferred in the hour or so it will take your lab to thaw your FFP since most community hospitals won’t have pre-thawed plasma. You could probably get platelets in a quicker fashion but FFP will take time. The more progressive helicopter crews will have plasma on board but not all. Obviously you are going to do the best you can with what you have but any advice from you or… Read more »
Hi Scott,
I work at a small district general in the UK and see very little trauma, but I see a lot of upper GI bleeds. Do you think the findings of this study are transferable to other causes of major haemorrhage?
Cheers
Tom
Hi Scott, Great podcasts keep up the great work. Kudos to John and his team for the huge amount of work that must have gone into performing this trial. However I firmly believe that “blind” administration of fixed ratio blood products in major haemorrhage is already an anachronism. To me this study is like debating which blind landmark technique to use when inserting your CVC when the real questions are what is the best technique to follow when you use USS. We changed from a fixed ratio blind algorithm to ROTEM guided therapy for the major obstetric haemorrhage (3-4/week) in… Read more »
Love it as always. Ok group, am in a 28k square mile area with 2 trauma centers on opposite ends from each other. Which journals will best convince our local blood bank medical director to get on board with blood product admin-HEMS specific. YES, we are behind, but in desperate need to catch up. (Been carrying TXA for awhile. Would like to move forward.