
LVAD Emergencies
These patients are super-complicated, luckily I got Zack Shinar, MD from Sharp Memorial in San Diego to try to wade through the morass.
All Situations
- Call the patient's VAD coordinator ASAP
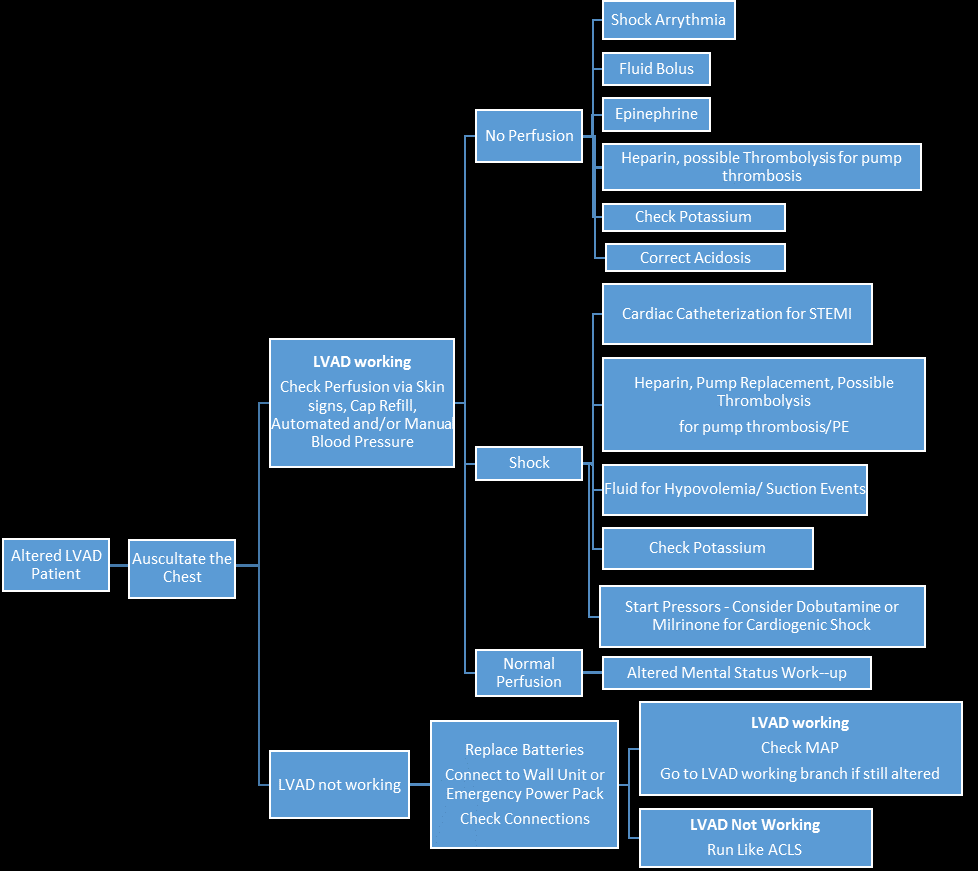
- These patients may not have a palpable pulse. Listen over the heart to hear if the motor is working. Then use mental status, skin color/temp, and the machine flashing Low Flow as indicators that perfusion badness is occurring. Do a bedside echo. The MAP should be ~65 on manual doppler BP, Automated BP devices may give you a MAP as well. A-line MAP is the most accurate.
- Try not to cut or yank out the drive-line, 'cause that is embarrassing.
Poor Perfusion
- When in doubt, consider a fluid bolus. VADS love volume. If you need to improve hemodynamics with a working LVAD, consider preload augmentation and possibly afterload reduction (if MAP is high).
- Consider inotropes–if you think it is right heart failure, give dobutamine. If you think the patient is septic and has markedly reduced afterload, consider norepinephrine.
- On echo:
- Big RV, small LV=pulm hypertension or right heart strain/stemi. Correct hypoxemia and acidosis, consider volume, screen for RV STEMI, consider inotropes.
- Small RV-give volume
- Big RV & LV-pump failure or pump thrombosis.
Consider pump thrombosis–Signs of pump thrombosis are LVAD is hot, working hard, with high RPM, low flow, dilated RV/LV, and low MAP. Zack would give a bolus of 5000 U of Heparin in the decompensating LVAD that he thought was secondary to thrombosis (or if he just couldn't figure out what was wrong with a failing device). He would also consider tPA if he really thought it was pump thrombosis and the patient was decompensating and peri-code.
On ECHO, a dilated RV/LV could be from pump thrombosis or non-working pump (electrical issue for example).if you think that is the problem, heparinize.
Machine Not Running
Check batteries. Make sure all of the lines are connected.
Bleeding
These folks are prone to bleeding from the anticoag (and probably additional plt dysfunction from the device if I had to guess). So if they have altered mental status or neuro findings–consider hemorrhagic stroke.
Patient appears Infected
Drive-line infection-look at the site at entry to the skin. If the patient appears septic and you can't find a source, consider it a device infection until proven otherwise. Don't yank the device. Treat for health-care associated infection covering both hospital gram negatives and MRSA.
Patient is Coding
We need to AVOID CPR until the patient needs it and at point, what is the alternative? Can you rip out the device with CPR-yes! Many of the CT surgeons recommend not to do CPR, but you can't get deader than dead (I was not a philosophy major, so I could be wrong). Avoid CPR if at all possible, some of the 1st gen devices had hand-pumps you could use–the current generation don't. If you're the point where there is NOTHING else to do except CPR you need to use your clinical judgment.
Here is Zack's clinical judgment:
CPR is not recommended by the manufacturers secondary to potential cannula dislodgement. I would not do CPR unless the pump was NOT working and the patient had lost their BP (MAP of 0). This is the one scenario where you have to perfuse the brain no matter what the cost. All other scenarios I would focus on how to get that pump operating better (at all).
Joe Bellezo then adds:
Just agreeing with Zack's thoughts on this. My approach to this is ‘Look, Listen, and feel” – assuming a comatose LVAD patient.
Look: …at all the connections. Everything connected? Ok. Look at the controller. Green Light on? Yes..ok. No? Troubleshoot for a problem with the VAD and keep working until you get the green light on the controller.
Listen: to the hum. Assuming a green light on the controller…there should be an LVAD Hum. No hum? the pump isn't functional (duh). Find out why. Again, check all the connections and then touch the control box and check RPM, flow, etc). Pump thrombosis is your reversible problem here.
Feel: hot control box is not good and usually means thrombosis or dislodgement of the outflow cannula to the aorta…or distal obstruction like a dissection.
Compressions: here is my thought: if you've gone through all of the above and there is nothing to fix…then you have an LVAD patient who does not have a functional LVAD. I would treat them just as if they came to the ED the day before they got their LVAD: a patient with end stage heart failure and no blood pressure. I would begin chest compressions if their MAP was below 60 because they aren't perfusing their vital organs and will die. I know this goes against Zack's recommendations but that shows you that nobody really knows the best answer here. This patient will die. I say start the chest compressions and get inotropes going. Dobutamine or milrinone stat in addition to levophed. In other words…pretend they don't have a VAD and aggressively resuscitate them. Yes, dislodging the pump is possible…but these patients are going to die anyway.
Though if I had to guess Zack and Joe would only do CPR long enough to crash the patient on to ECMO.

Read this PDF Now
An insanely good field guide from mylvad.com.It has device-specific recommendations. Read it NOW!
The site also has some excellent additional resources.
Additional Resources
Another great review on LVADs from Fire Engineering
the images from this post are from mylvad
Update
Great Review (Emerg Med Austral 2014;26:104)
Additional New Information
More on EMCrit
EMCrit 334 – CV-EMCrit – Concise HeartMate 3 LVAD Overview(Opens in a new browser tab)
EMCrit 235 – Cardiac Arrest Science with Zack Shinar(Opens in a new browser tab)
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
about a year ago, we had an LVAD pt who was brought in for being dizzy & weak – he was put in our resus area. we were getting him hooked up to a monitor & while others were flitting about plugging in the LVAD, getting a line, trying to get a bp (which we couldn’t get), etc – when i looked up & noted that he was in VT at 200. oh sh** – following ACLS – is he stable or not? dunno – can’t get a bp reading but he’s awake & talking to us. our next big… Read more »
surreal for sure. almost all of the current gen. devices can be shocked without damage as you discovered. Great stuff.
Remember that LVADs support only the LV and not the RV (BiVADS are used only in acute situations mostly post-operative situations). RV output is mandatory for the LV to fill and if a patient is in VT or VF, there is not RV output and so LV does not fill and pump cannot function. Thus, its very important to maintain a rhythm- whether native/paced for the RV to function (+/- inotropes) for a normal LVAD function. Hence you would need to cardiovert the patient.
I enjoy reading case reports of sustained VF in these patients; who needs pulsatile blood flow anyways! Although, this leads me to wonder if EMS is in a position to cardiovert or pace in the field, should we have similar coagulation concerns as with “don’t mess with A-fib >48 hours”?
With regards to pump thrombosis, you will see an increase in POWER not necessarily RPMs. Second and Third gen pumps are usually fixed RPM. (With certain pumps you can see an transient decrease in RPMs that can be related to volume status as the pump detects a low flow state and tries to give the LV time to fill.) I agree with the rest, look for a hot controller/hot skin over the pump, lack of hum and high Watts (power). Also consider trans-thoracic echo while looking for aortic valve opening. If your patient appears poorly perfused, is hypotensive and still… Read more »
Great comments, Brandon. I agree with all of your suggestions. Remember that these are left ventricular ASSIST devices, not bypass devices. They augment the left ventricle – not bypass it. So, while you may have a patient in VFIB and awake (we had a patient in VFIB drive themselves to our ED!!!!) it isn’t ideal and not sustainable. Cardiovert.
Thank you for this excellent Podcast. It is also relevent for EMS responders who may have an LVAD patient in their response areas and don’t know a lot about trouble shooting the device. The EMCRIT blog and Podcasts have been excellent learning opportunities, Thanks Scott!
thanks, Jeff.
****UPDATE regarding chest compressions in LVAD patients: We just reviewed every in-hospital LVAD patient who received CPR at our facility. We found 10 patients who received chest compressions after coding because of a nonfunctional LVAD (ie thrombosis, motor dysfunction, etc). 5 patients survived to hospital discharge after the LVAD issue was resolved. 5 patients died after brain-death. No LVADs were dislodged. I will probably publish this data but here are the preliminary results. BOTTOM LINE: LVAD not functioning? MAP 0? Do chest compressions.
Joe, your data is interesting. I would love to do the same for my facility. What types of devices do you primarily see? I have seen one pump dislodgement secondary to chest compressions with a Gen II axial flow device, however, the patient was rushed to O.R. where the pump was successfully re-seated and the patient lived. Pump dislodgment is much more common in the axial flow devices that sit in a pump pocket as opposed to adjacent to the ventricle in the pericardial space. There is a small amount of animal research to support the use of chest compression… Read more »
Brandon, We see Heartmate II LVADs. We are starting to trial HVAD (Heartware), not sure start date. I am unsure about the likelihood of dislodgment by generation or placement of pump, but it’s a great topic. It makes perfect sense that the Heartware device would have a much lower possibility of dislodgment given the size. Certainly, Heartmate II devices would seem less likely to dislodge than the old pulsatile VADs. Joe mentioned our data and I think in the non-working LVAD without perfusion, chest compressions are reasonable. I also fear about medics/physicians doing compressions on patients with a working VAD… Read more »
Zack,
I agree, what is amazing about this patient population is how much you can get from a hands on physical assessment and remembering the basic components of cardiac output. Joe, I love the idea of “look, listen, and feel”. Great podcast and comments. There are some excellent clinical pearls that people should take away across the spectrum, from the pre-hospital environment to the ICU.
Brandon
Zack, thanks for making LVADs less scary. Regarding compressions: the Emergency Physicians Monthly article currently in print, summarizing your EMRAP interview, mentions abdominal compressions being preferable to chest compressions in these patients. Thoughts?
Bill, This has been visited a few times in the past with regards to cardiac arrest, post-cardiac surgery via median sternotomy. The key concept at play here is Coronary Perfusion Pressure, which we all know is the vital component to ROSC. Coronary Perfusion pressure is defined as the “aortic-to-right atrial pressure gradient during the relaxation phase of cardiopulmonary resuscitation” (Paradis et al., 1990). Paradis and gang also found that only those with a CPP of 15 mmHg or greater had ROSC. There were various studies over the decades since that article was written that showed in human, swine and computer… Read more »
Brandon and Bill, I completely agree with the emphasis we need on CPP and the stuff Norm did elucidating this is fantastic. What we also know is that even good chest compressions sometimes does not get adequate CPP. It takes amazing chest compressions (and some favorable anatomy) to get the CPP up to the upper tier of favorable survival (>25 mm Hg). I do not know the AO-CPR data well enough to say for sure but my educated guess is there’s no way in vivo we will be able to obtain these pressures with AO-CPR. My suggestion is forget about… Read more »
Brandon–You have an amazing range of LVAD knowledge. Can you tell us who you are and what you do. Thanks for your comments!
Scott, I am a Critical Care Flight RN for a hospital affiliated rotorwing/CCT program. My background is in Cardiothoracic ICU and Cardiovascular Recovery where we would commonly see devices such as HMII, HW, Centrimag for temporary extracorporeal (R, L, And BiVAD) support and of course ECMO. Our flight team also staffs the Level I Trauma center at our flagship hospital, which happens to be the intake point for LVAD emergencies. In my spare time I work with our outstanding VAD team doing pre-discharge patient teaching, and I have begun to work with some of the community healthcare facilities on LVAD… Read more »
Fantastic. It is bringing folks like you, Zack, and Joe together in the same forum that makes this blog so much fun for me.
great overview and discussion. we do IABP transports and a paed ECMO service in the state is just starting. LVAD transports are going to get more common so thankyou for this
Sorry, I’m a little late to the ballgame! We’re looking at establishing guidelines and training our rapid response and step down nurses with respect to coding the LVAD patient. Our CTICU nurses are experienced with it, but less so on the floor/step down. We’re having trouble finding any actual research on the subject, just expert opinion. This discussion will add a lot to it. Does anyone know of any published research data on this subject? Particularly with regard to CPR. Dr. Bellazo, your info is great and you should publish it. I’ve not found anything so far like it.
My husband had his LVAD since September 23 came home October 23,was doing pretty good but recently has been complaining that the site from his line hurts most of the time especially when he trys to get up from bed or a chair has had some bleeding from the site-very slight no oder I am worried about this but he just shakes it off–is any of this normal and if so how long will it take for this to get better?
Thank you for any help you can give me.
So sorry, we can’t answer patient (or patient’s family’s) questions here. I recommend contacting your husband’s physicians. Be well.
Hi Scott, I’m a paramedic here in Ga, and we have been receiving notifications of LVAD patients in our catchment area. Most notably one of my old partners just receivied one, and as such, I am seeking to obtain as much information as available. With regard to the debate of CPR for unconscious patients upon whom blood flow can not be confirmed with a dopler, I am inclined to agree that compressions would be indicated. We currenly use the LUCAS compression devices on our ambulances and my personal experiences with them has been phenominal to say the least. I am… Read more »
definitely. wish i had a LUCAS
I would like to know all about OAC CPR how to perform this how many times breaths hands placement and is approved by the AHA and if so why is it not taught to instructors of CPR?
Has not been proven for prime-time use yet.
Advice I got from Montefiore trained CHF specialists- don’t do chest compressions on an LVAD pt it just doesn’t make sense. If they’re really not perfusing figure out how to troubleshoot the LVAD, or give fluids in the meantime.
Great Article. analysis – I was fascinated by the analysis . Does anyone know if my assistant can access a blank KY KREC Tenant Move-in Move-out Condition Inspection Report example to use ?
I appreciate this discussion, thank you. Joe Bellezzo and Brandon what are the policy’s in your institution regrading CPR? The professional who cares for these devices are well area of the argument AGAINST CPR but like has been mentioned after other attempts and troubleshooting for correctable issues why not CPR. I also would like to see American Hearts Official viewpoint. I correlate it to making the statement “We don’t do CPR on a CABG” which is fine when there is not an open chest cart with a CT surgeon at the bedside but after time is provided what answer is… Read more »
Hi! I don’t take care of LVAD patients, but am interested in learning more. Just to clarify — NO hum is not heard when thrombosis is present? It’s easy to understand the low flow, high pressure idea, but I’m confused as to why the hum would completely go away. Thanks!
Hi there! Just FYI, the link to the “insanely good field guide” does not work.
But here’s a new link: https://www.mylvad.com/sites/default/files/EMS%20Field%20Guides/2019%20Field%20Guides/Total%20Document/2019%20EMS%20Field%20Guide%20Complete%20Document.pdf
Thank YOU!!!!!!!