
Intro:
If you take care of patients with acute brain injuries then you have probably calculated an ICH score in the last week or two.
The score is simple. You plug in patient’s:
➡️ GCS (3-4, 5-12, 13-15)
➡️ Age (under or over 80)
➡️ The size of the bleed (more or less than 30 mL)
➡️ The presence of absence of IVH
➡️ And if it’s an infratentorial origin- yes or no.
Based on the patient’s characteristics, you get both a number and a predicted 30 day mortality.
For example, let's take this case:
50-something year-old person with a 35cc supratentorial hemorrhage + IVH who presented as a GCS of 4:

You can access MDcalc.com and plug in those stats to get:

97% mortality.
This results in triage calls that sound much like this:
“I’ve got a guy here, pretty young, came in looking terrible. GCS 4, we intubated him. Scan shows a big bleed. ICH score 4. Not sure how much you’ll be able to do, but need to transfer him.”
This is just one example, but something we face in neurocritical care regularly.
There has historically been a sense of nihilism for these patients with high scores. It’s understandable. If almost everyone dies with this injury, shouldn't we just give up?
A post urging “Please don’t!!”
Background on the Score
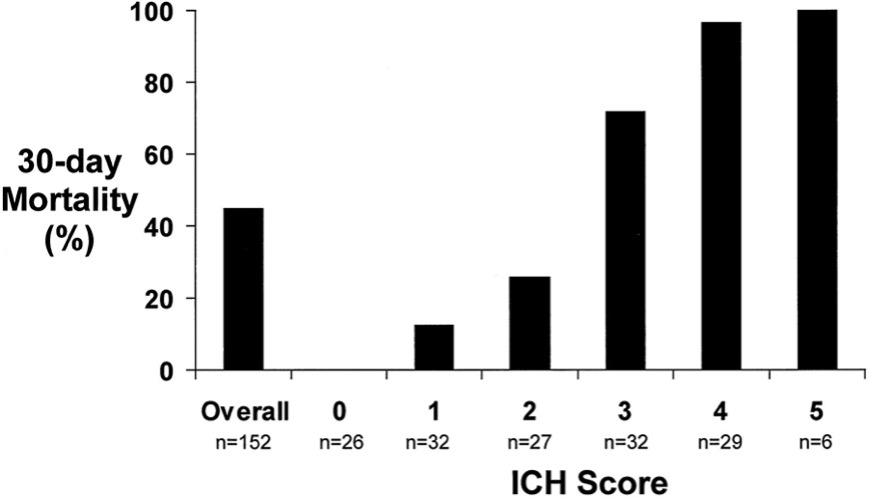
The score was developed as a reliable and easy way to calculate a severity index. It was determined from a retrospective cohort using a logistic regression analysis of independent predictors of mortality (11283388)
Since its initial publication, it has been the most validated of the ICH severity scoring tools (30426449). As such, it has been widely implemented across stroke centers, with the Joint Commission requiring its documentation within the first 6 hours of presentation as a key indicator for comprehensive stroke center certification.
There is a benefit to this: Early scoring allows classification and risk-stratification. It serves to provide a baseline indicator of patient illness, which is helpful for hospitals as they navigate quality metrics. It can be helpful in clinical trials design and entry.
This is not to argue that we shouldn’t use the ICH score, but that the ICH score – as any score – has limitations.
Back to this Case:
The patient is intubated and transferred to our ICU. On arrival the patient opens eyes to noxious stim and the best motor score was a withdrawal on the left (GCS 6T). That’s a significant improvement from GCS 4.
Maybe the first exam was wrong, but probably not! Does anyone really look their best when they are not protecting their airway and aspirating?

More about the spiral of ICP crisis here: https://emcrit.org/pulmcrit/icp/
Intubation and normalization of pH can profoundly affect a neuro exam.
After transfer, an external ventricular drain (EVD) was placed. Several hours later, the patient was opening eyes to voice and mimicking commands on the left (9T).
These were simple interventions. Just good, basic neuroresuscitation. With these interventions the patient more than doubled their GCS and their ICH score decreased by a point
Count that a win! Change the ICH score to 3?
Not exactly. Per the Joint Commission, the score must be calculated before surgical interventions. http://tinyurl.com/y8uf624r.
![]()
For healthcare systems it’s important to understand the admission severity, but there can be a real downside to this: every day we fill out a note that reminds us of a dismal prediction.
A solution here, though: Document the initial ICH score, but also keep a “resuscitated ICH score.” (this is a good strategy for The Hunt-Hess scores in aneurysmal Subarachnoid Hemorrhage patients, too!)
Despite this, an ICH score of 3 would still predict a 72% mortality.
With that in mind, it would feel evidenced-based to have a goals of care conversation citing this data, so why should you not use that number to counsel families?

It was developed as a framework for standardized communication and disease severity rating. The ICH is validated in global cohorts, and it is great for saying that on average a patient with an ICH score of 4 has a more severe injury than a patient with an ICH Score of 3.
Why not use it for Acute Prognostic Decisions?
To answer that – another question: “Why do patients with ICH die?”
Some ways…
👉Progression to brain death
👉Mucus plugging
👉Sepsis
👉PE
But, by far the most common cause of death is withdrawal of life support. Data demonstrates that in ICH about 80% of patients died of withdrawal of life sustaining therapies (WLST) (19726752)
Although families integrate more than just our predictions into their understanding of a patient’s illness (20228686), if we predict that a patient is very likely to die or never regain meaningful function, we dramatically move the needle in how likely this is to become true…because patient’s surrogates opt for WLST.
This “self-profiling prophecy” is inherent to the ICH score, as WLST was allowed within the cohort. Said differently, patients with high grade scores were likely felt to be poor candidates for a meaningful recovery; thus, maximally aggressive care was not continued and they passed, which artificially validates “Most patients with high scores die.”
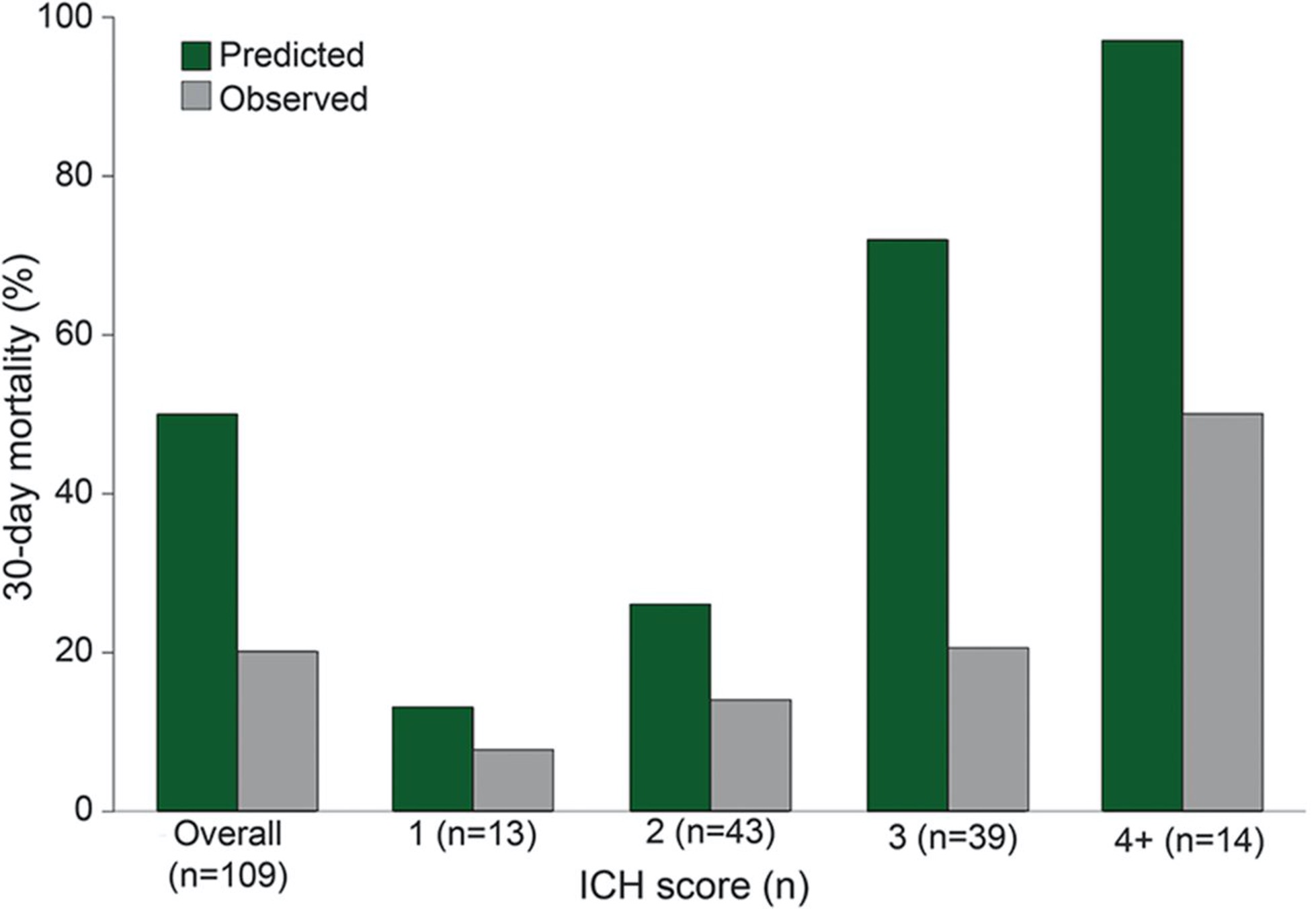
The ICH score investigators fortunately recognized this and repeated the study in a small group (109 patients), who agreed to withhold a decision regarding Do Not Resuscitate or withdrawal care for 5 days. (25817842)
By deferring major de-escalation for just 5 days, while obtaining more data about how the patient was doing and giving the families more time to process, the 30-day mortality shrunk by more than half (from ~ 50% overall death to 20%) with the greatest changes seen in those with higher-grade scores. Demonstrating again, the profound toll of early WLST.
This case captured how the admission GCS score is one way in which the ICH score doesn’t capture a patient-specific trajectory and the immediate potential for improvement with interventions like an EVD.
Similarly, the other binary metrics also may not capture the complexity of an individual patient:
- A whiff of IVH is different from every ventricle being casted with blood.
- A 21 year old and a 79 year old will both score a “0” but have dramatically different neuro-resilience and ability to withstand a critical illness.
- An infratentorial hemorrhage might be one that obliterates the pons or might be a bleed in the cerebellum (which depending on characteristics, may have Level 1A support for a surgical intervention that can dramatically change the illness trajectory ).
We have data demonstrating that younger patients may tolerate their ICH better than predicted even in a study where early WLST was allowed (34247055):

That the ICH score has limitations for acute prognostication and decision making about who gets aggressive care and who gets withdrawal of life support is not a secret! Reflections about this are written by the score’s creator (Dr. Claude Hemphill) right there on the MDCalc website.

MDCalc has also included a disclaimer to the ICH score, but this can be overshadowed by the number that looms large.

Ultimately, neuro prognostication is very challenging. Perhaps the hardest thing we do in the NeuroICU. Fortunately, for ICH, research demonstrates that clinicians are better predictors of mortality and recovery than a score (26674335). One reason is that an algorithm doesn’t account for the subtleties of each case. It doesn’t consider the patient’s medical history and patient specific factors like resilience, cognitive reserve, and frailty.
We know in other specialties that frailty is a major predictor of who returns to high function after critical illness. Although this has not been well studied in the neurocritical ICH population yet, it’s reasonable to hypothesize that those with high admission frailty may have a worse outcome. Thus, even a low-score ICH may have a devastating impact on a patient with high frailty, while a patient with high resilience may regain a higher than predicted functional outcome with a high-grade bleed.
Fortunately, the newest guideline from the AHA/ASA have made intentional space for this diagnostic humility and our desire as neurointensivists to avoid the nihilism of the self-fulfilling prophecy.


In the grand scheme of time, the second full hospital day is such a short amount of time.
Yes, there are instances in which this delay could be detrimental: delaying prognostication in the very rare situation where a patient may suffer a cardiac death (and thus suffer what would be futile CPR); by harm to the family in whom delaying comfort might feel goal-discordant for their loved one (many of these cases would likely have a known limitation on life sustaining treatment and thus be excluded from these guidelines); or by financial burdens to families with limited insurance safety nets.
But, it is clear from the data that early withdrawal of life support dramatically reduces those that might be destined to outperform the early prognostic evaluation.
This case is an example when maximally aggressive care resulted in a survival benefit that was aligned with what the family felt was an acceptable quality of life.
In summary:
✨ The ICH score is a number that is helpful in conveying disease severity
✨ Limitations include that it was determined from a cohort in which early withdrawal of care was allowed which biases towards the self-fufiling prophecy
✨ Like many scores, it captures neither the context of injury nor patient specific factors such as frailty and reserve.
✨ Use it as part of the diagnostic evaluation, but not as a determination of who gets maximally aggressive care and who doesn’t!
- EMCrit 336 – Team NeuroEMCrit's Critical Neuro Cases – Part 2 - November 3, 2022
- NeuroEMCrit – Team NeuroEMCrit's H&R Conference Talk, Part 1 - October 3, 2022
- NeuroEMCrit – The Perils of the ICH Score - August 1, 2022
Just a little note of gratitude for your most recent blog entry. Your thoughts and observations were insightful and stimulating. I value the time and work you invested in writing such a polished and educational post.
Once more, I want to express my gratitude for providing your readers with information and experience. Your commitment to creating excellent information is clear, and I forward reading more of your pieces in the future.
Source – https://www.tharwaniinfrastructures.com/imperial/