
The Acid Base Series
- EMCrit 44 – Acid Base – Part I
- EMCrit 45 – Acid Base – Part II
- EMCrit 46 – Acid Base – Part III
- EMCrit 50 – Acid Base – Part IV – Choose the Solution Based on the Problem
- EMCrit 96 – Acid Base – Part V – Enough with the Bicarb Already
- EMCrit 97 – Acid-Base – Part VI – Chloride-Free Sodium
- EMCrit 227 – Acid Base Ep. 7 – Bicarb Updates, Quantitative Approach, and Prof. David Story
Time for more discussion of acid-base, a subject you know i obsess about.
Bicar-ICU Trial
- Read the amazing trial by Jaber et al.
- PulmCrit's take
- The Bottom Line
- CCNerd
Keith Corl's Email
Hi Scott,
By now I'm sure you've seen the work from Jaber's group on using bicarb in critically ill academic patients. Obviously there are limitations to the trial, not the least of them a negative primary outcome. And while the study wasn't powered to look a 28 day mortality or 7 day organ failure in those with a AKIN score of 2-3 I am sure many will take this positive secondary finding and run with it.
My biggest criticism was that they didn't break the study down into patients with anion gap metabolic acidosis (AGMA) vs. non-anion gap metabolic acidosis (NAGMA). I'm a big fan of your acid base pods and tend to agree with your take and the Forsythe paper and don't give bicarb to patients with an AGMA. So I went ahead and emailed Jaber and he got back to me. He told me that “90% of the patients enrolled were hyperlactatemic.” Moreover, most GI and renal patients with base loss were excluded b.c. bicarb was considered standard care, therefore the “large majority” had an AGMA. Interesting, now I'm second guessing myself and wondering if I should consider bicarb in AKIN patients with a AGMA.
I'm interested to hear your thoughts. I think it would make a great pod or a topic for Josh or Rory.
I hope all is well,
Keith
then I bring on Dr. David Story to discuss acid base and a set of posts by Jon-Emile Kenny.
Professor David Story
 Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU), Melbourne Medical School, University of Melbourne; Director, Melbourne Clinical and Translational Sciences (MCATS) research platform
Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU), Melbourne Medical School, University of Melbourne; Director, Melbourne Clinical and Translational Sciences (MCATS) research platform
Jon-Emile Kenny Lactate Debate Posts
Gamblegram
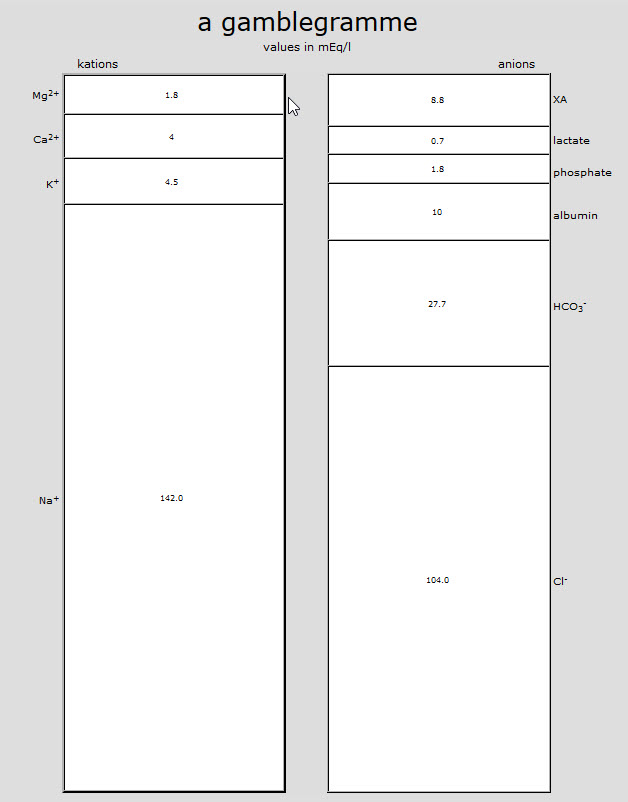
go to acidbase.org and use their analyzer to truly understand the quantitative approach
More Stuff to Read
Intracellular pH always decreases with sodium bicarb (See Table I)
Bicarb administration causes decreased ICal
If you control CO2 and Calcium, then it works (Animal Study-Anesthesiology 2014;120:926)
Additional New Information
David Story Review of Stewart for the OR
More on EMCrit
Additional Resources
You Need an EMCrit Membership to see this content. Login here if you already have one.
Professor
Nassau University Medical Center
No conflicts of interest (coi).
- EMCrit 373 – Mike Weinstock with another Critical Care Bounceback: “Asymptomatic Hypertension” - April 18, 2024
- EMCrit Wee – Ross Prager on 10 Heuristics for the New ICU Attending - April 13, 2024
- EMCrit 372 – FoundStab Intubation SOP - April 5, 2024
On the topic of DKA acidosis Vs Sepsis acidosis. The way we used to talk about the difference at my old shop… where we had a disproportionately high number of young people with electively poorly controlled TIDM is… These DKA patients, particularly the frequent attenders that everyone knows on a first name basis. You know the ones, they have all of the sequelae of diabetes and are even a nightmare to phlebotomise as they have sclerotic IJVs from repeated central access. They live in a perpetual state of acidosis. They control their sugars and thus, their acod-base status, so poorly… Read more »
i have not found this to be the case
these pts are more like asthmatics
they may show up recurrently, but between attacks they are normal if they have access to insulin. (if they don’t then they will be constantly in a state of ketoacidosis. but not sure if there is adaptation so much as the acidosis is not clinically relevant. they come in for dehydration not acidosis and not b/c of tolerance IMO
I agree it is worth noting how well we see DKA patients tolerate severe acidemia with normal BP’s. I’m not so sure, however, that it has to do with habituation to acidemia, as much as the “metabolic mess” underlying the acidemia. Similar to the acute respiratory acidotic with a pH < 7 who is probably obtundation but not in shock or probably even hypotensive. Which brings up the big question for me – is acidemia on its own even a "bad thing" that warrants an attempt at being directly corrected? What tiny amount of human data that exists on the… Read more »
I agree that it is somewhat of a simplistic view to use habituation to acidaemia as a direct causation of this tolerance in DKA. It’s just a way that we came to think about it. The regularity with which this subset of patients tolerate significant acidaemia is impressive. I agree that it definitely lends itself to the argument of how clinically significant isolated acidaemia is. The reality of it is that the confounders are huge, will we ever have a group of people that we can study acidosis in without the major confounders you have already touched on. From my… Read more »
fantastic ?s!! i was right on the fence to give bicarb to renal failure pre-CRRT. my intensivists and nephrologists at both of my EDICU venues both want us to administer and I have held back to do v. little evidence. It could all come down to avoiding HD and we would get just as good outcomes if we just didn’t do HD, but acidosis is an indication at the place I work, so essentially regardless of the reason–bicarb may help my patients (whether it is due to intrinsic benefit or just avoiding CRRT). The reason why not to give it… Read more »
Hi, I was wondering about the assertion that Ringer’s Lactate will cause an immediate acidosis which then converts to a long term alkalosis with proper liver function.
However, in this post by Dr. Farkas (https://emcrit.org/pulmcrit/understanding-lactate-in-sepsis-using-it-to-our-advantage/), he asserts that the lactate in LR is sodium lactate and thus acts more as a buffer than an acid promoting substance.
How do you reconcile these two views?
there is no need for reconciliation–those 2 are the same statement
What is the mechanism for that initial acidosis then?
Because my understanding of Dr. Farkas’ post is that initial administration is pH neutral with a later trend towards alkalosis
lactate is a strong anion that acts as an acid
What I understood so far from your podcasts and the Stewart-book is this: The initial acidosis has nothing to do with lactate acting as an acid (actually its a base), rather the SID of the solution causes the initial acidosis. If lactate is a strong anion (and it is), then the acid-base effects of a lactate solution should be estimated by the SID of that solution. LACTIC ACID leads to acidosis because it decreases SID. On the other hand, Ringer-Lactate/Hartmanns contains SODIUM-LACTATE, not lactic acid, with a SID much lower than the plasma. So if the lactate is not metabolized,… Read more »
lactate is a strong ion that acts in the vernacular as an acid.
yes lactate acts as an acid b/c it reduces the SID. Ringers/Hartmanns has the the exact SID to keep the plasma neutral, (lower than normal plasma SID to make up for dilution of weak acids)–given that the lactate is metabolized. Otherwise it is essentially NS. It doesn’t cause subsequent alkalosis when metabolized, it maintains neutrality.
Great podcast – thanks for the shout-out – and I’m glad that this contributes to clinicians thinking about acid-base..