
Introduction
Hemorrhage is a common cause of death in cirrhosis, especially variceal bleeding. These patients often have complex coagulopathies. Furthermore, some coagulation abnormalities may precede variceal re-bleeding (Chau 1998). Thus, immediate and definitive coagulation management is important. Unfortunately, the traditional approach is misguided and potentially dangerous.
#1: An elevated INR reveals nothing about coagulation
 The liver synthesizes both clotting factors and endogenous anticoagulants (e.g. antithrombin and protein C). In cirrhosis, levels of all of these proteins are reduced. This typically leads to “rebalanced hemostasis,” wherein levels of pro- and anti-coagulant proteins are reduced to a similar extent. This produces an overall clotting tendency which is close to normal.
The liver synthesizes both clotting factors and endogenous anticoagulants (e.g. antithrombin and protein C). In cirrhosis, levels of all of these proteins are reduced. This typically leads to “rebalanced hemostasis,” wherein levels of pro- and anti-coagulant proteins are reduced to a similar extent. This produces an overall clotting tendency which is close to normal.
The INR measures the level of several clotting factors. Therefore, in this situation the INR will be elevated. However, the INR is only evaluating half of the picture.
The concept of rebalanced hemostasis explains some otherwise puzzling findings. This explains why the INR fails to predict bleeding following procedures (Northup 2013). Rebalanced hemostasis also explains how patients may experience portal vein thrombosis or deep vein thrombosis despite an elevated INR.
There are so many problems with INR as a measure of hemostasis in cirrhosis that its position as an indicator of plasma transfusion is inexplicable, and its use in guidelines at specific values amounts to something of a religious belief. –Northup 2013
INR is not entirely meaningless in the setting of cirrhosis, but rather it may function a bit like a D-dimer. If the INR is normal then enzymatic coagulation is intact. However, if the INR is elevated, then it reveals nothing about coagulation. Most cirrhotics with elevated INR have fairly normal enzymatic coagulation, but many are actually hypercoagulable, and a few are hypocoagulable.
#2: Consider thromboelastography (TEG) to test enzymatic coagulation
Recently TEG has emerged as a more integrative approach which explores both clotting factors and cellular interactions. This involves monitoring thrombosis and thrombolysis within a sample of whole blood (further introduction to TEG here).

The R-time is useful in cirrhosis because it reflects both pro- and anti-coagulants, allowing it to measure the balance of enzymatic coagulation. Thus, the R-time can serve as a replacement for the INR in cirrhosis. Unlike INR, TEG does correlate with bleeding. TEG-based transfusion strategies during liver transplantation have reduced the transfusion requirements, similar to their success in trauma (Clevenger 2014).

Infection may trigger the release of endogenous heparinoids with an anticoagulant effect. These can be distinguished from a true enzymatic hypocoagulability by running a TEG containing heparinase. This distinction is relevant because only true enzymatic hypocoagulability can be treated with fresh frozen plasma. Many labs have a protocol to test this automatically (e.g. a TEG with prolonged R-time will reflexively trigger a repeat TEG with heparinase).
TEG isn't perfect, for example results may vary somewhat with different reagents (Coakley 2006). TEG’s greatest weakness may be that it misses anti-platelet drugs unless they are tested with a specially modified TEG assay. However, TEG is currently the best clinically available test of enzymatic coagulation in cirrhosis. Pending further evidence in this context, a reasonable approach might be to consider data from both TEG and traditional coagulation tests (e.g. fibrinogen)(1).
#3: Giving FFP usually doesn't help

FFP causes no improvement in coagulation when evaluated using global assays capable of detecting rebalanced hemostasis (either TEG and thrombin generation assays; Tripodi 2012, Clayton 1995). Why? FFP increases the level of both pro-coagulant proteins and anti-coagulant proteins. For a patient on warfarin with a severe clotting factor deficiency, the addition of clotting factors has a dominant effect, so FFP works. However, for a patient with cirrhosis who is in a rebalanced state to begin with, the addition of both pro- and anti-coagulant proteins may not tip the balance much.
FFP will reduce the INR, because it increases the absolute level of clotting factors. This has incorrectly reinforced the practice of using FFP for decades. Unfortunately, reducing the INR will not help the patient clot: it fixes the numbers but not the patient.
It is conceivable that FFP could actually exacerbate bleeding by diluting other clotting elements (e.g. platelets) and by increasing the blood pressure driving the hemorrhage (more on this below). Furthermore, the short half-life of clotting factors within FFP causes any benefit to be transient, whereas the harm from volume expansion persists.
blood products may paradoxically contribute to bleeding rather than prevent it –Weeder 2014
Liver transplant surgeons recognized long ago that they could safely omit pre-operative FFP (Dupont 1996). Ironically, surgeons have been comfortable taking patients with elevated INR for liver transplant, while other specialties continue to balk at performing minor procedures without FFP.
#4: Platelet transfusion probably does help
Available evidence suggests that platelet support is helpful. Unlike INR, platelet count does correlate with post-procedure bleeding (Giannini 2010). Compared to other blood products, platelets seem particularly effective in improving TEG parameters (Clayton 1995). Different in vitro assays suggest a platelet target of roughly 50,000-60,000, which is similar to the traditional platelet target of >50,000 (Solomon 2015, Tripodi 2015).
This is not a departure from traditional therapy, but perhaps a re-prioritization. For example, in a hemorrhaging patient with an INR of 3.5 and a platelet count of 45,000, the primary priority might be platelet transfusion rather than “correcting” the INR.
#5: Don't forget the fibrinogen
Fibrinogen is commonly overlooked, but it shouldn't be. The entire point of the coagulation cascade is activation of fibrinogen so that it can form a clot. The yellow strands holding together this clot are made out of fibrinogen:

With progressive cirrhosis, fibrinogen levels often decrease (Stravitz 2012). Among patients undergoing liver transplantation, fibrinogen supplementation reduced the requirement for platelets, PRBCs, and FFP (Noval-Padillo 2010). Recent guidelines suggest targeting a fibrinogen level of >150-200 mg/dL, an increase compared to prior recommendations to target a fibrinogen level >100 mg/dL (Levy 2015).
#6: Consider tranexamic acid (TXA)
One function of the liver is clearance of proteins involved in fibrinolysis (e.g. endogenous tissue plasminogen activator – that's right, tPA). With worsening cirrhosis, these proteins accumulate in the blood leading to hyperfibrinolysis in perhaps 30-50% of patients (Leebeek 2015). Unfortunately, TEG may be insensitive to this hyperfibrinolysis (e.g. endogenous tPA loses activity within minutes of drawing the patient's blood).
Tranexamic acid (TXA), a fibrinolysis inhibitor, should be well suited to this situation. TXA shows promise in upper GI bleeding, with the most recent Cochrane Review suggesting a mortality benefit (RR 0.6, 95% CI 0.42-0.87; Bennett 2014). In liver transplant surgery, meta-analysis of RCTs found that TXA is safe and effective in reducing blood loss (Molenaar 2007).
The safety of TXA is supported by RCTs in a variety of situations (Ng 2015). However, the efficacy of TXA in GI bleeding remains controversial. Currently TXA may be considered on a case-by-case basis, particularly if there is evidence of hyperfibrinolysis (e.g. increased fibrinolysis on TEG or unusually low fibrinogen levels; Laskiewicz 2014). Hopefully further insight will come from the HALT-IT trial, a large pragmatic multi-national RCT of TXA in GI hemorrhage.
#7: Avoid over-resuscitation
 Variceal bleeding is a setup for over-resuscitation. Patients with cirrhosis are often hypotensive at baseline due to chronic vasodilation. Variceal bleeding often presents with hematemesis. This combination (hematemesis plus hypotension) may create a dramatic presentation leading to aggressive transfusion, even if the patient hasn't actually lost much blood.
Variceal bleeding is a setup for over-resuscitation. Patients with cirrhosis are often hypotensive at baseline due to chronic vasodilation. Variceal bleeding often presents with hematemesis. This combination (hematemesis plus hypotension) may create a dramatic presentation leading to aggressive transfusion, even if the patient hasn't actually lost much blood.
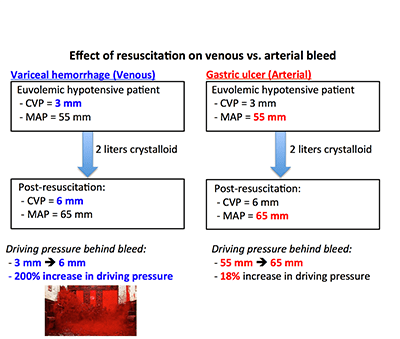 Unfortunately these patients may be particularly harmed from over-resuscitation for two reasons. Unlike most bleeding, variceal bleeding originates from a venous source. Therefore, over-resuscitation which drives up the central venous pressure will directly increase the driving pressure of the bleed (adjacent figure)(4). Secondly, patients with cirrhosis start out with low levels of platelets and fibrinogen, increasing their risk of developing a dilutional coagulopathy.
Unfortunately these patients may be particularly harmed from over-resuscitation for two reasons. Unlike most bleeding, variceal bleeding originates from a venous source. Therefore, over-resuscitation which drives up the central venous pressure will directly increase the driving pressure of the bleed (adjacent figure)(4). Secondly, patients with cirrhosis start out with low levels of platelets and fibrinogen, increasing their risk of developing a dilutional coagulopathy.
When in doubt, it may be better to avoid large-volume resuscitation. To provide insurance in case the patient opens up, establish excellent vascular access and ensure that the blood bank is ready with lots of products on hold.
The crazy idea: Rethinking our targets for factor replacement?
Traditional models of coagulation emphasize linear coagulation pathways, which imply that deficiency of any factor would mandate replacement of that same factor. This model was developed to understand patients with severe deficiency of a single clotting factor, such as hemophilia. It may not work as well for critically ill patients, who often have numerous, moderate factor deficiencies.
TEG suggests an alternative viewpoint, which is that there may be a greater degree of flexibility, redundancy, and synergism between different components of coagulation (figure below). For example, clot strength seems to reflect both platelet count and fibrinogen level. Thus, to a certain extent, a high fibrinogen level may compensate for low platelet count or vice versa (Mallett 2015).

This implies that our exact selection of blood products may be less important than we thought. It is possible that rather than dealing with individual coagulation targets, we may only be dealing with a single holistic coagulation target:
Traditional concept of blood product targets:
(Platelets) > Platelet target
(Fibrinogen) > Fibrinogen target
(Enzymatic coagulation) > Enzymatic coagulation target
Holistic concept of blood product targets:
(Platelets)(Fibrinogen)(Enzymatic coagulation) > Single target
A holistic coagulation target would generally favor the use of cryoprecipitate and platelets over FFP, because cryoprecipitate and platelets are provided as concentrates. In contrast, FFP causes volume expansion which may dilute out platelets, thereby defeating its effectiveness. According to this model, FFP would only be useful if there were a severe deficiency in enzymatic coagulation.
Extending this concept to include fibrinolysis might suggest the equation below (where c is a proportionality constant). This could explain how a fibrinolytic inhibitor might be beneficial in hemorrhage regardless of what the rate of fibrinolysis is, even if it is within the “normal” range (e.g. the success of TXA in the CRASH trials).
Holistic blood product target incorporating fibrinolysis:
[(Rate of fibrin generation) – (Rate of fibrin degradation)] > Single target
[c(Platelets)(Fibrinogen)(Enzymatic coagulation) – (Fibrinolysis)] > Single target
Moving forwards it may be worth re-considering our strategy for blood product repletion. Our current strategy of repleting every component to an individual target (to achieve a roughly euboxic coagulation panel) is effective, but perhaps not ideal. For example, it might be safer to target a supra-normal fibrinogen level, while tolerating permissive thrombocytopenia and focusing on a TEG-based coagulation target (e.g. adequate clot strength as measured by the maximum amplitude).

- Most cirrhotics are in a state of rebalanced hemostasis, due to similar reductions in pro- and anti-coagulant proteins. This often yields a normal overall clotting tendency.
- INR measures the level of clotting factors only, not the overall balance of coagulation. To determine the balance of enzymatic coagulation, thromboelastography (TEG) is needed.
- Responding to an elevated INR by transfusing FFP is a misguided practice which should be abandoned. Cirrhotics rarely have true enzymatic hypocoagulability, so they generally do not benefit from FFP.
- For patients with cirrhosis and bleeding, repletion of fibrinogen and platelets may be more effective in achieving hemostasis.
- A subset of patients with advanced cirrhosis appear to have hyperfibrinolysis. Such patients may benefit from tranexamic acid.
- In the context of a variceal hemorrhage, over-resuscitation may aggravate bleeding by markedly increasing the blood pressure within the varicies.
- Our general strategy of repleting blood factors individually to target a roughly “euboxic” coagulation panel should be questioned. It is possible that focusing on the overall balance of coagulation and fibrinolysis, rather than individually normalizing each component, may allow for a more flexible and effective approach.
- For now, the following approach may be reasonable:

Related posts
- Coagulation, TEG, & TXA:
- Do patients with liver disease need FFP before procedures? (BoringEM)
- TXA in trauma: CRASH2, CRASH2 debate, & Karim Brohi's SMACC talk (EMCrit)
- Insanely entertaining lecture by Mark Walsh about TEG (Maryland CC Project)
- Potential dangers of euboxia by Chris Nickson (LITFL)
- Management of the critical GI bleeder:
- Upper GI Bleed Guidelines (EMCrit)
- Intubating the critical GI Bleeder (EMCrit)
- Blakemore tube placement (EMCrit)
Notes
- Significance of the alpha-angle: Previously it was believed that the alpha-angle was an assay for fibrinogen, whereas the MA was an assay for platelet function. Unfortunately this isn't the case, but rather both are a reflection of a combination of platelet and fibrinogen function (Solomon 2015). Of these two parameters, MA seems more useful because it is more robust across different assays. Fibrinogen function can be measured using a special TEG assay containing a platelet inhibitor, but this approach seems to be more popular in Europe currently (Harr 2013).
- Cutoff value for LY-30: According to the manufacturer, the normal LY-30 is 0-7.5%. However, evidence from trauma-induced coagulopathy reveals that hemorrhage risk increases when the LY-30 is >3%, leading many trauma algorithms to recommend an anti-fibrinolytic agent if LY-30 >3% (Holcomb 2012, Chapman 2013). Among patients with cirrhosis, LY-30 is usually well below 3%. For example, in one series the median LY-30 was 0.25% with a range of 0-3.2% (Stravitz 2012) and in another the LY-30 was 0.14% +/- 0.37% (Pietri 2015). Therefore, a cutoff of >3% might be a reasonable indication for administration of TXA in a hemorrhaging cirrhotic. Until further evidence is available, decisions to administer TXA may be made by combining the LY-30 with other laboratory evidence of fibrinolysis and clinical judgement.
- The author's conclusions were: “This review found that TXA appears to have a beneficial effect on mortality, but a high dropout rate in some trials means that we cannot be sure of this until the findings of additional research are published.”
- Due to portal hypertension, the pressure in the varicies may not be exactly equal to the CVP. Regardless, the general concept should remain valid: over-resuscitation may cause a substantial fractional increase in the pressure within the varices.

- Pulmcrit wee: The cutoff razor - April 15, 2024
- PulmCrit Blogitorial – Use of ECGs for management of (sub)massive PE - March 24, 2024
- PulmCrit Wee: Propofol induced eyelid opening apraxia – the struggle is real - March 20, 2024
Your post about coagulopathy management in cirrhotics is very interesting. I’d go further with a proposal of a protocol. I am a liver transplantation surgeon and i believe that a protocol including the use or not of FFP during liver transplantation should be useful. What do You think about that? I will be the first to join a protocol like that….Thanks a lot
Transplant surgery has historically led the way with regards to understanding TEG and transfusion in cirrhosis. This is a great situation for RCTs because the conditions are reasonably uniform and well controlled. Would love to see some RCTs comparing different TEG-based transfusion algorithms in this setting, for example, one which tries to use more fibrinogen and TXA with avoidance of FFP. To date there have been studies comparing conventional labs vs. TEG-based algorithm, but I’m not aware of any studies in liver transplant comparing between two different TEG-based algorithms.
When I was a resident on the ‘liver service’ we would do paracentesis on tons of end stage liver disease folk. We rarely worried about an elevated INR as our attendings had decades of liver experience. When I got out of training, it was hard to watch as most docs wanted a normal INR before they would let you tap the belly.
Thanks for your post…always nice to consolidate the facts in a quick read. Sometimes we know stuff and dont know why we know it…but when somebody puts it all together in a nice package.
Yes, I’ve had very similar experiences with paracentesis in cirrhosis. I was trained that it was OK to do paracentesis in cirrhotic patients despite elevated INRs… have done this for years without a problem but never entirely understood why.
When we are told “we’ve always done it this way,” occasionally that is actually the right way of doing something for reasons which we don’t yet fully understand. Although perhaps more often, it is nonsense.
Interesting piece. I think alot of anticoagulant/procoagulant theory has yet to make a clinical impact, this also applies to the TEG since no standardization in method or clinical protocol for bleeding have been extensively tested. Although I’m a bit skeptical to the endougenous heparinoids part, what are your source? I did my grad project on the effect of endogenous heparinoids in hepatic failure (Defined as INR > 1,5) using the parallel system to TEG, namely ROTEM. We included 40 patients of which about half was septic (SIRS > 2). We found no endogenous heparinoids whatsoever in ANY patient using heparinase… Read more »
Forgot to fill in I’m a House Officer (in Sweden, i think its the correct translation)
Yes, one problem with TEG is a lack of standardization and also the fact that different continents use different systems (e.g. TEG largely in US vs. ROTEM in Europe). On the endogenous heparinoid issue, one reference is Clin Liver Dis 2009; 13: 43-53 by Senzolo M. Different authors have detected these with various frequencies, so it may relate in part to the exact system and reagents used. I am planning to do an entire post on endogenous heparinoids in the future, hopefully this might clarify the issue a bit. Thanks for your skepticism, I will look into this further before… Read more »
Thanks Josh, An excellent summary if i ever have a variceal bleed i want you to look after me! Although you have aimed this post at only bleeding in the context of liver disease in fact I believe that this is the approach that should be used in all major haemorrhage (eg Trauma, obstetrics, vascular), and all of your comments regarding FFP and clot strength etc hold true. TEG or ROTEM guided therapy lets you see what the actual deficiencies are and correct those. Large volumes of FFP administered blindly are usually not what is required- FFP doesn’t help the… Read more »
Alexis EM Resident. Great Article, but have to comment on the pic. Love The Shining! “Here comes Johnny!”
A true classic.
Thanks for a great post.
How about the use of PCC to correct INR in the bleeding cirrotic?
Great question, this is currently under investigation with a pending clinical trial (the PROTON trial).
PCC replaces the vitamin-K dependent clotting factors, but patients with cirrhosis typically have a deficiency in *all* clotting factors. Thus, I am skeptical of the ability of PCC to improve clinical bleeding (although it will probably make the INR look better). Will be interesting to see the results of this study. In the interim, it is not my practice to use PCC in this situation.
Very enlightening! There is one issue which I don’t understand. You often mention giving a cyroprecipitate transfusion. I live in Germany and here this blood product is almost completly unheard of – I have talked to a specialist in transfusion medicine from our local university hospital.
I suppose you transfuse it because it is a source of fibrinogen for which we use pure human fibrinogen that comes in factory-made bottles.
A terrific post as always Josh. A small point though- would bleeding varices not be more dependent on a raised mean systemic filling pressure rather than CVP?
This is fantastic!
Further more – it is another nail to the coffin of giving ffp for “any bleed”
Or what drives me crazy – inr/= 7
Plt > /= 50k
Fibrinogen > / = 100
Interestingly our cost-benefit analysis showed TEG to be cost neutral when compared to getting pt/ptt/inr/fibrinogen/fibrin/fsp/ d dimer
When you add the saving from avoiding inappropriate ffp in lieu of tranexamic acid –
Then the savings come through
That’s our Blood Management Program next step
TEG based algorithms to help MDM in coagulation and hemorrhage
Thanks for your input and sharing your work!
considering re-balanced state. In Warfarin or DIC for example, although there is deficiency of clotting factors, FFP will raise both clotting factors and anti-Coagulant (Protein C). So again they will be in balanced state ( or will be in the same ratio as prior to FFP transfusion).